Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
111 Cards in this Set
- Front
- Back
|
Acute Renal Failure associated with reversible injury to the tubular epithelium
|
Acute Tubular Necrosis
|
|
|
List the 3 gereral causes of Acute Tubular Necrosis
|
1. Ischemia (hypoperfusion)
2. Nephrotoxins 3. Heme proteins |
|
|
List the possible Ischemia causes of Acute Tubular Necrosis
|
1. Hypovolemic shock
2. Sepsis 3. Burns 4. Prolonged surgical operations |
|
|
List the possible Nephrotoxic causes of Acute Tubular Necrosis
|
1. Toxic chemicals = CCl4 & Ethylene Glycol (Antifreeze)
2. Heavy metals = Hg 3. Drugs = Cisplatin, Aminoglycosides |
|
|
List the Heme protein causes of Acute Tubular Necrosis
|
Crush injuries
1. Myoglobin = rhabdomyolysis -can be observed after intense exercise 2. Hemoglobin = Hemolysis |
|
|
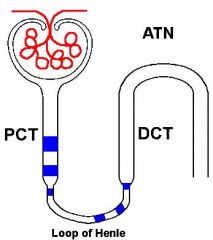
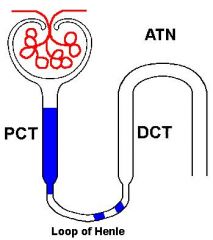
Why is the Proximal Convoluted Tubule (PCT) commonly damaged in Acute Tubular Necrosis?
|
1. PCT's are the first place a toxin will reach after they have been filtered in the glomerulus
2. PCT has alot of fxns = requires alot of Energy = very susceptible to Hypoxia -> material will slough off and occlude Loop of Henle -> Oliguria |
|
|
Describe the pathology of Acute Tubular Necrosis
|
1. Cortex > Medulla
2. Necrotic tubular cells slough off 3. Intratubular cast in the Medulla Collecting Ducts = decreases GFR 4. Regeneration of tubules occurs fast = takes about 2 weeks to replace cells |
|
|
Acute Tubular Necrosis:
-Death due to __1__ from __2__ can occur during the __3__ phase |
1. Arrhythmia
2. Hyperkalemia 3. Oliguric |
|
|
Urinalysis shows "dirty brown GRANULAR CASTS" and "epithelial casts"
|
Acute Tubular Necrosis
|
|
|
What are 85% of the cases of Acute Pyelonephritis due to?
|
Ascending bacterial infection due to a gram-negative microbe
**KEEPS -Klebsiella -E. coli -Enterobacter -Pseudomonas -Serratia |
|
|
What usually precedes Acute Pyelonephritis?
|
Lower UTI
|
|
|
Bacterial infection involving the Renal Pelvis, Tubules, and Interstitium
|
Acute Pyelonephritis
**spares Glomeruli |
|
|
What are the clinical manifestations of Acute Pyelonephritis?
|
1. Fever
2. Flank pain with Costoverterbral angle 3. Neutrophilia 4. Leukocyte casts in the urine |
|
|
List 8 predisposing conditions for developing Pyelonephritis
|
1. Urinary Stones
2. Hydronephrosis 3. Cystitis 4. Prostatic Hyperplasia 5. Tumors 6. Pregnancy 7. Vesico-ureteric reflux 8. External ureteric compression (fibrosis |
|
|
What is the mnemonic for predisposing conditions to Pyelonephritis?
|
URINE
-Urolithiasis = urinary stones -Reflux (vesico-ureteric) -Infections of Lower UT -Neoplasms (Ureteric, Vesical, Prostatic) -External Compression = Pregnancy, Retroperitoneal Fibrosis |
|
|
What gender is most commonly affected by Acute Pyelonephritis?
|
Females
**have shorter urethra **Acute Pyelonephritis is most commonly associated with ascending infections |
|
|
Acute Pyelonephritis:
1. Usually unilaterial or bilateral? 2. Focal or diffuse? 3. ____ in tubules --> interstitium 4. ______ with tissue destruction |
1. Unilateral
2. Focal 3. PMNs 4. Abscesses |
|
|
Describe the pathologies seen in Chronic Pyelonephritis
|
1. Cortical scars
2. Loss of Papillae 3. Dilation of Calices 4. Hydronephrosis = dilation of the renal pelvis and calices |
|
|
What is the most common cause of Nephrotoxic type of Acute Tubular Necrosis?
|
Aminoglycosides
-Gentamicin |
|
|
What is the gross pathology of Chronic Pyelonephritis?
|
irregularly shrunken small kidney
|
|
|
What is pathognomonic for Acute Pyelonephritis?
|

White cell casts in urine
|
|
|
Describe the histology of Chronic Pyelonephritis
|
1. Chronic inflammatory infiltrates = Plasma Cells, Lymphocytes
2. Tubular atrophy with Eosinophilic casts = "Thyroidization" of the kidney |
|
|
Chronic Pyelonephritis
|
"Thyroidization" of the kidney
|
|
|
What gender is more prone to getting Renal Calculi?
|
Males
|
|
|
2 types of Renal Calculi that are visible on X-ray
|
1. Calcium
2. Struvite = Ammonium-Magnesium Phosphate |
|
|
What type of stones are 75% of Renal Calculi?
|
Calcium Oxalate or Calcium Phosphate
|
|
|
What are Struvite Stones associated with?
|
Urease + bacteria = split urea into Ammonium
-Proteus vulagaris -Staphylococci |
|
|
What environment worsens Struvite stones?
|
Alkaline urine
|
|
|
Stone type that often form Staghorn Calculi
|
Struvite stones = Ammonium-Magnesium Calcium Phosphate
|
|
|
Under what 3 conditions are Uric Acid stones seen?
|
1. Gout
2. Leukemia = due to high cell turnover 3. Acidic urine **Purine -> Hypoxanthine -> Xanthine -> Uric Acid |
|
|
What are Cystine stones usually due to?
|
Cystinuria = hereditary impaired reabsorption of Cystine
|
|
|
What is the treatment for recurrent Calcium stones?
|
Hydrochlorothiazide
|
|
|
What is the treatment for Uric Acid stones?
|
Allopurinol = inhibits Xanithine Oxidase
|
|
|
Dilation of the renal pelvis and calyces caused by urinary outflow obstruction and is associated with progressive atrophy of the kidney
|
Hydronephrosis
|
|
|
What % of Americans are affected by Urolithiasis?
|
5-10%
|
|
|
What part of the US are Renal Calculi more common?
|
"Stone belt" = Southeastern US
|
|
|
How do patients with Renal Calculi present?
|
1. Flank pain radiating toward the Groin & colicky abdominal pain
2. Hematuria 3. Pyelonephritis 4. Hydronephrosis |
|
|
Patient with Flank pain radiating to the Groin and has been having large amounts of blood in the urine
|
Renal Stones
|
|
|
Are most Renal Tumors benign or malignant?
|
Malignant
|
|
|
Benign Renal tumor composed of uniform cells that have round nuclei and well developed Eosinophilic cytoplasm
-cytoplasm contains numerous mitochondria |
Oncocytoma
|
|
|
What is an Angiomyolipoma?
|
Benign Hamartoma composed of FAT (lipoma), SMOOTH MUSCLE (myo), and Blood vessels (angio)
|
|
|
What syndrome are Angiomyolipoma's associated with?
|
Tubular Sclerosis Syndrome
-Mental retardation & epilepsy -multisystem hamartomas |
|
|
What is the most common Renal tumor?
|
Renal Cell Carcinoma
|
|
|
What is the peak age for Renal Cell Carcinoma?
What is the gender ratio? |
60 years old
M:F = 2:1 |
|
|
What are the risk factors for Renal Cell CArcinoma? (3)
|
1. Tobacco = Smoking
2. von Hippel-Lindau disease = deletion on chr 3 (found in 98% of sporadic RCCs) 3. Adult Polycystic Kidney Disease |
|
|
Large solitary yellow mass found most commonly in the Upper Pole
|
Renal Cell Carcinoma
|
|
|
Tumor that often invades the Renal Vein and may extend into the Vena Cava and Right Atrium
|
Renal Cell Carcinoma
|
|
|
What is the most common mode of spread of Renal Cell Carcinoma?
|
Renal vein invasion
|
|
|
What does Renal Cell Carcinoma arise from?
|
Tubular Epithelium
|
|
|
What are the common hematogenous sites of spreading of Renal Cell Carcinoma?
|
Lungs
Bone Brain |
|
|
Polygonal clear cells
|
Renal Cell Carcinoma
|
|
|
What is the classic triad of Renal Cell Carcinoma?
|
1. Hematuria (50%)
2. Flank pain 3. Palpable mass |
|
|
Patient presents with cola-colored urine and flank pain. After taking a careful history you find that the man has low-grade fever & has lost 10 lbs over the past month. He is a chronic smoker. On physical exam you feel a large mass in the left kidney. Lab demonstrates Secondary Polycythemia
|
Renal Cell Carcinoma
|
|
|
What is the 5-year survival for Renal Cell Carcinoma?
|
40%
|
|
|
What paraneoplastic syndromes are associated with Renal Cell Carcionoma?
|
1. Secondary Polycythemia = due to EPO secretion
2. Hypercalcemia = due to PTH 3. Hypertension = due to renin secretion 4. Amyloidosis |
|
|
What is the most common symptom of Renal Cell Carcinoma?
|
Hematuria
|
|
|
Childhood renal tumor
|
Wilms tumor
|
|
|
Most common abdominal solid tumor in childhood
|
Wilms tumor
|
|
|
Are most cases of Wilms Tumor sporadic or familial?
|
Sporadic = 90%
Familial - 5% |
|
|
What is the peak age for Wilms tumor?
|
2 years old
*98% < 10 years |
|
|
What syndrome is Wilms Tumor associated with?
|
WAGR syndrome
-Wilms tumor -Aniridia = no iris -Genitourinary malformation -Mental-motor Retardation |
|
|
When is Bilateral Wilm's tumor more common?
|
in familial cases
**instead of Sporadic |
|
|
90% of Wilms tumors are uni- or bilateral?
|
Unilateral
|
|
|
Describe the histology of Wilms tumors
|
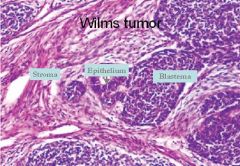
-Immature stroma with primitive tubules and glomeruli
-Mixture of immature cells = metanephric, stromal, tubular |
|
|
What is Wilm's tumor also known as? What is the significance of this?
|
Nephroblastoma
-composed of cells in the Renal Blastema (fetal metanephros) |
|
|
What is the treatment and prognosis of Wilm's tumor?
|
Chemotherapy + Surgery = 5 years = 90% survival
|
|
|
What indicates a better prognosis in Wilms tumor?
|
Children < 2 years = better prognosis
|
|
|
What is the cause of Wilm's tumor?
|
deletion of WT-1 gene (tumor suppressor) on the short arm of Chromosome 11
|
|
|
What does Wilm's tumor originate from?
|
Primitive Metanephric tissue
|
|
|
What 4 things is Transitional Cell Carcinoma of the Kidney associated with?
|
Pee SACS
-Phenacetin -Smoking -Aniline dyes -Cyclophosphamide -Schistosomiasis |
|
|
What part of the kidneys does Transitional Cell Carcinoma occur in?
|
Renal Calyces and Pelvis
*also in Ureters and Bladder |
|
|
How does Transitional Cell Carcinoma of the Kidney present?
|
Painless hematuria in Smokers
|
|
|
What classic diad does Wilm's tumor present with?
|
Unilateral Flank mass
Hypertension = HTN |
|
|
Ischemic = more segmental
|
Would the cause of this Acute Tubular Necrosis commonly be due to Ischemic or Toxic effects?
|
|
|
Toxic = diffuse effects
|
Would the cause of this Acute Tubular Necrosis more commonly be due to Ischemic or Toxic effects?
|
|
|
Acute Tubular Necrosis
-Cortex is pale -Medulla is congested and contains all the sloughed off crap |

What is this pathology?
|
|
|
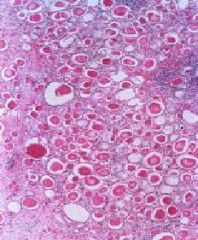
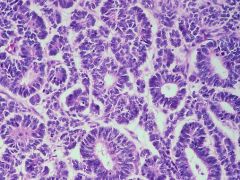
Acute Tubular Necrosis:
-Coagulative necrosis in the Collecting Ducts -Oblong tubule @ 3 o'clock -> will regenerate within 2 wks |
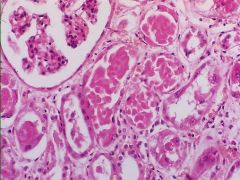
What is this showing?
|
|
|
Acute Tubular Necrosis
-Proximal Convoluted Tubules are thin walled when they should be Tall columnar |
What is this?
|
|
|
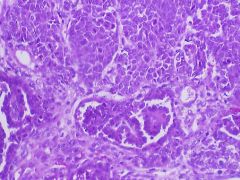
Acute Tubular Necrosis
-epithelium of the tubules seen here are rugged from undergoing necrosis from Ischemia -Heart failure with hypotension precipitated the ATN |
What is this pic showing?
|
|
|
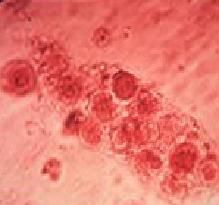
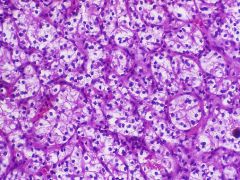
Acute Tubular Necrosis
-The tubular vacuolization and tubular dilation here is a result of the toxic effect of ethylene glycol poisoning. This is representative of acute tubular necrosis (ATN), which has many causes. ATN resulting from toxins usually has diffuse tubular involvement, whereas ATN resulting from ischemia (as in profound hypotension from cardiac failure) has patchy tubular involvement. |
What is seen here?
|
|
|
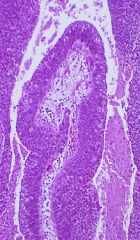
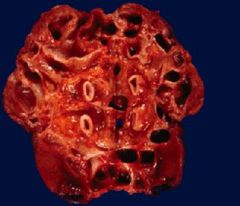
Acute Pyelonephritis
-This is a gross photograph of a kidney showing scattered grey-white areas representing collections of acute inflammatory cells. The pelvis is dilated, which is consistent with hydronephrosis. The most common pathogen associated with acute pyelonephritis is E. coli. Acute PN is secondary to an ascending infection usually beginning in the bladder. Vesicoureteral reflux is the most common cause of acute pyelonephritis. |

What is seen here?
|
|
|
Acute Pyelonephritis
Ascending Gram - infection |
What is this?
What is the most common cause? |
|
|
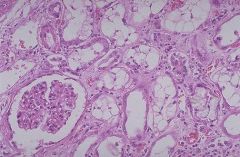
Acute Pyelonephritis
-PMN's within Tubules and the Interstitium *spares Glomeruli |
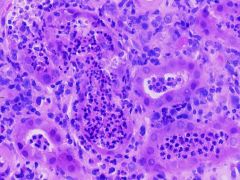
What is seen here?
|
|
|
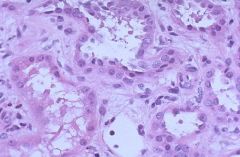
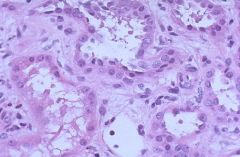
Chronic Pyelonephritis
|

What is the cause of this?
|
|
|
Chronic Pyelonephritis
-Tubules contain Eosinophilic casts = "Thyroidization" of the kidney -due to obstruction of the tubules |
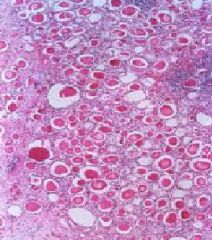
What is the cause of this?
|
|
|
Chronic Pyelonephritis
|
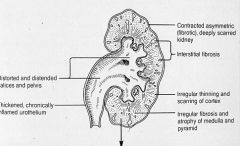
What is the cause of all these pathologies?
|
|
|
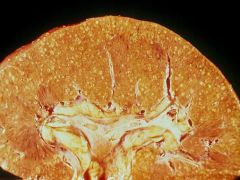
Chronic Pyelonephritis
-Dilated calyces -narrow Cortex |

What is the cause of this pathology?
|
|
|
Staghorn stone = Struvite stone = Ammonium-magnesium Calcium Phosphate
|

What is seen here?
|
|
|
Oncocytoma
|

What renal tumor is this?
|
|
|
Oncocytoma
-benign tumor that has a pink cytoplasm and small nucleus -cytoplasm has abundant mitochondria |
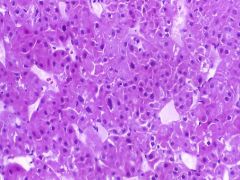
What tumor is this?
|
|
|
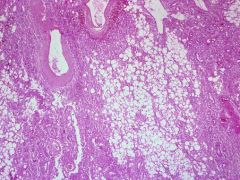
Angiomyolipoma
|

What renal tumor is this?
|
|
|
Angiomyolipoma
-Blood vessels -Smooth Muscle -Fat Tubular Sclerosis Syndrome |
What is shown here?
What is it associated with? |
|
|
Angiomyolipoma
-This is the low power microscopic appearance of an angiomylolipoma. There is normal renal parenchyma at the left. The tumor has a strip of adipose tissue (the "lipoma" part) that then blends in with interlacing bundles of smooth muscle (the "myo" component) in which are scattered vascular spaces (the "angio" component). |
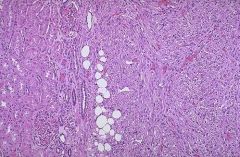
What is seen here?
|
|
|
Renal Cell Carcinoma
-large solitary yellow mass found most commonly in the upper pole |

What is this showing?
|
|
|
Renal Cell Carcinoma
-Polygonal cells with Clear Cytoplasm |
What is this showing?
|
|
|
Wilms tumor
*has been split open |

What is seen here?
|
|
|
Wilms tumor
|
What is seen here?
|
|
|
Transitional Cell Carcinoma
|
What is seen here?
|
|
|
Transitional Cell Carcinoma
|

What is seen here?
|
|
|
Transitional Cell Carcinoma
|

What is seen here?
|
|
|
Transitional Cell Carcinoma
|
What is seen here?
|
|
|
What 2 parts of the kidney are particularly susceptible to Ischemic Acute Tubular Necrosis?
|
1. Straight portion of the Proximal Tubule
2. Ascending thick limb |
|
|
What part of the kidney is particularly susceptible to Nephrotoxic Acute Tubular Necrosis?
|
Proximal Convoluted Tubule
|
|
|
Which is usually more severe, Ischemic or Nephrotoxic Acute Tubular Necrosis?
|
Ischemic
|
|
|
List the 3 stages of Acute Tubular Necrosis
|
1. Initiation Stage
-reduced blood flow thru the kidneys = decrease in urine output -slight increase in BUN 2. Oliguric Stage -urine volume is significantly reduced -salt and water overload -rising BUN conc.'s -Hyperkalemia -Metabolic Acidosis 3. Polyuric stage -glomerular fxns reestablished -regenerating tubules cannot concentrate the urine = large quantities of dilute urine are formed -Loss of Sodium and Potassium --> dehydration -Patients who reach this phase usually recover completely |
|
|
A 60-year-old hospitalized man being treated with long-term IV Gentamicin suddenly becomes nauseous and oliguric. Your physical exam is significant for development of rales and a new arrhythmia. An ECG shows peaked T waves with a prolonged QT segment. When his lab values come back, they indicate Hyperkalemia, Hyperphosphatemia, Azotemia, and elevated Urine Sodium. Urine sample shows muddy brown casts
|
Acute Tubular Necrosis
|
|
|
Fever + Flank pain + Neutrophilia = ?
|
Acute Pyelonephritis
|
|
|
What abnormality allows bacteria to ascend the ureter into the renal pelvis and cause Acute Pyelonephritis?
|
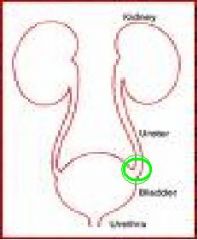
Vesicoureteral reflux
|
|
|
Corticomedullary scar overlying a dilated calyx
|
Chronic Pyelonephritis
-Calyces of the upper pole are dilated with reduced renal parenchyma between calyces |
|
|
What is the chemical composition of urinary calculi caused by chronic urinary infection?
|
Magnesium Ammonium Phosphate (struvite) stones
|
|
|
Associated with WT-2
Clinical features: -Wilms tumor -Hemihypertrophy of the body -Macroglossia (big tongue) -Visceromegaly (enlargement of the abdominal organs) |
Beckwith-Wiedmann Syndrome
|