Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
85 Cards in this Set
- Front
- Back
|
This is the most common form of Acute Glomerulonephritis
|
IgA Nephropathy = Berger Disease
|
|
|
What is the most common age group for IgA Nephropathy?
|
Young adults = 15-30 yoa
|
|
|
Describe the pathology of IgA Nephropathy
|
Focal and segmental glomerulopathy caused by deposition of IgA in the Mesangium
|
|
|
What are the clinical manifestations of IgA Nephropathy?
|
Protean manifestations:
-40% asymtomatic microscopic hematuria -40% bouts of macro hematuria -10% nephrotic syndrome -10% renal failure **many present with recurrent hematuria (red/cola-colored urine) 1-2 days after a respiratory infection |
|
|
What is the histology of IgA Nephropathy?
|
Focal proliferative glomerulonephritis with diffuse mesangial widening
|
|
|
A 15-year old Asian-American boy presents with red-colored urine. After a history, you are informed that he is suffering from a strange flu-like syndrome that began 2 days earlier consisting of vomiting, myalgias, arthralgias, and fever
|
IgA Nephropathy
-postinfectious disease (usually respiratory infection) -Nephritic type syndrome -most commonly seen in young adult males |
|
|
Synonym for Crescentic Glomerulonephritis
|
Rapidly Progressive Glomerulonephritis
|
|
|
List 4 causes of Crescentic Glomerulonephritis
|
1. Anti-GBM nephritis = Goodpasture's Syndrome
2. ANCA granulonephritis = Wegener Granulomatosis, Microscopic Polyarteritis nodosa, Churg-Strauss Syndrome 3. Immune-complex Glomerulonephritis = Henoch-Schonlein purpura, Cryoglobulinemia 4. Non-immune |
|
|
What is important with Crescentic Glomerulonephritis?
|
You must diagnose and treat patients ASAP, or they'll lose both kidneys within a couple weeks
|
|
|
What is the cause of Crescentic Glomerulonephritis in 50% of the cases?
|
Post-streptococcal etiology
|
|
|
When auto-antibodies are more active when the blood is cold
|
Cryoglobulinemia
|
|
|
List the properties of Anti-Glomerular Basement Membrane Antibody Glomerulonephritis
|
1. Rapidly Progressive GN mediated by antibody
2. Antibody is to Collage type IV 3. Linear IF 4. Fibrinoid necrosis of GBM 5. Crescentic GN 6. Goodpasture Syndrome |
|
|
ANCA granulonephritis that does not have granular deposits on Immunofluorescence
|
Wegener granulomatosis
|
|
|
What does ANCA Glomerulonephritis begin as?
|
Necrotizing GN --> becomes Crescentic
|
|
|
ANCA is found in serum and binds to what?
|
PMN myeloperoxidase and Proteinase 3
|
|
|
Besides IgA Nephropathy, what other disease is characterized by a deposition of IgA in the Glomeruli?
|
Henoch-Schonlein Purpura
|
|
|
This disease has no immune deposits in the glomeruli, responds to immunosuppression, and is associated with small vessel polyangiitis
|
ANCA Glomerulonephritis
- Wegener Granulomatosis |
|
|
List the features of Nephrotic Syndrome
|
1. Proteinuria
2. Hypoalbuminemia 3. Generalized Edema 4. Hyperlipidemia = due to increase in lipoprotein synthesis 5. Lipiduria |
|
|
List the diseases associated with Nephrotic Syndrome
|
1. Minimal change disease
2. Membranous Glomerulonephritis 3. Focal Segmental Glomerulosclerosis 4. Diabetic Nephropathy |
|
|
What are 2 other terms for Minimal Change Glomerulonephrpathy?
|
1. Lipoid nephrosis
2. Nil disease |
|
|
This is the most common cause of Nephrotic Syndrome in Children
|
Minimal Change Glomerulopathy
|
|
|
What is the pathology of Minimal Change Glomerulopathy?
|
Under EM there is fusion of epithelial (podocyte) foot processes
**Light Microscope and Immunofluorescence show normal glomeruli |
|
|
What is the treatment for Minimal Change Glomerulopathy?
|
Steroids (prednisone)
|
|
|
A 4-year-old boy presents to the emergency with a 1-week history of generalized edema and fatigue. You history reveals that he suffered from a viral URI 1 week before the visit. Serum and urine studies show massive Proteinuria, hyperlipidemia, hypoalbuminemia. What pathology would you expect to see?
|
EM showing fusion on epithelial foot processes
= Minimal Change Glomerulopathy |
|
|
Nephrotic syndrome associated with heroin use, morbid obesity, Sickle Cell anemia, and HIV infection
|
Focal Segmental Glomerulosclerosis
|
|
|
Nephrotic syndrome that does not respond to Steroid treatment and most patients progress to ESKD in 5-10 years
|
Focal Segmental Glomerulosclerosis
**if HIV related -> ESKD in 1 year **if child is affected, may take 20 yrs to develop ESKD |
|
|
What is the pathology seen in Focal Segmental Glomerulonephritis?
|
- Sclerosis within Capillary tufts of deep juxtaglomerular glomeruli with Focal distribution and Segmental Distribution
-Hyalinosis = deposition of hyaline masses *Focal = involves some, but not all, glomeruli *Segmental = involves part of the glomerulus |
|
|
Most common cause of Nephrotic Syndrome in Adults
|
Focal Segmental Glomerulosclerosis
|
|
|
Nephrotic syndrome that has Immune-complex deposition that causes basement membrane thickening
|
Membranous Nephropathy
|
|
|
What is the cause of Primary Membranous Nephropathy?
|
Unknown
|
|
|
What is the cause of Secondary Membranous Nephropathy?
|
1. SLE
2. HBV, HCV, & syphillis 3. Drugs = Penicillamine 4. Malignancy = tumor antigens **Immune-complexes deposit in kidney --> Subepithelial |
|
|
What is the pathology seen under light microscope in Mebranous Nephropathy?
|
1. Diffuse membrane-like thickening of the capillary walls
2. Basement membrane "spike-and-dome" appearance is seen in Silver Methenamine stain |
|
|
A 40-year-old woman with a history of SLE presents to your office with a CC of increased swelling in her legs. She had been referred by her primary care physician who suspected a secondary illness to her lupus. Recent lab studies show proteinuria, hypoalbuminemia, hyperlipidemia, and hypercholesterolemia. You suspect that a renal biopsy would demonstrate immune-complex deposition on electron microscopy as well as "spike and dome" appearance on silver methenamine stain
|
Membranous Nephropathy
|
|
|
What pathology is seen on EM in Membranous Nephropathy?
|
Immune-comple deposition in Subepithelial locations
|
|
|
What is the treatment for Membranous Nephropathy?
|
No treatment -> is a slowly progressive disorder
|
|
|
What pathologies does Diabetic Glomerulosclerosis cause?
|
1. Diffuse global thickening of the basement membrane
2. Nodular sclerosis (Kimmelstiel-Wilson nodules) 3. Arteriosclerosis --> HTN 4. Trapping of serum proteins |
|
|
Kimmelstiel-Wilson nodules
|
Diabetic Glomerulosclerosis
= nodular accumulations of mesangial matrix material |
|
|
What is the clinical manifestation of Diabetic Nephropathy?
|
Proteinuria = major manifestation
**Nephrotic syndrome - severe proteinuria - Hyperlipidemia - Lipiduria |
|
|
Leading cause of chronic renal failure in the US
|
Diabetic Glomerulosclerosis
|
|
|
List the 4 diabetic kidney diseases
|
1. Glomerulosclerosis
2. Arteriosclerosis = thickened hyaline walls with narrow lumens --> HTN 3. Pyelonephritis = high concentrations of sugar in the interstitium promotes bacterial growth 4. Papillary necrosis = when the pyramid sloughs off and goes down into the renal pelvis |
|
|
What is Primary Amyloidosis?
|
Deposition of AL amyloid from Multiple Myeloma
**AL = amyloid light chain derived from Bence-jones proteins |
|
|
What is Secondary Amyloidosis?
|
deposition of AA amyloid in chronic suppurative conditions, such as purulent osteomyelitis or bronchiectasis
|
|
|
Where are Amyloid deposits found in the kidney?
|
1. Glomeruli (mesangium, GBM)
2. Arterioles 3. Tubular basement membranes |
|
|
What are the clinical manifestations of Amyloidosis?
|
1. Nonselective proteinuria (100% of cases)
2. Nephrotic syndrome (60% of cases 3. Renal failure develops over 2-5 yrs 4. Kidneys infiltrated with Amyloid become large!!! |
|
|
List 5 causes of Nephrotic Syndrome
|
1. Minimal Change disease
2. Focal and Segmental Glomerulosclerosis 3. Membranous Nephropathy 4. Diabetes Mellitus 5. Amyloidosis |
|
|
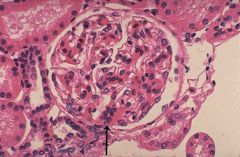
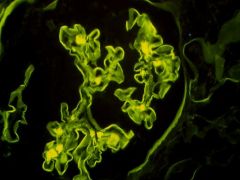
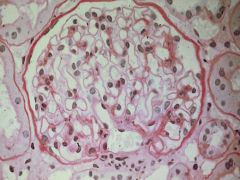
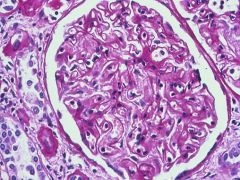
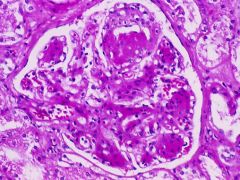
IgA Nephropathy
Focal proliferative glomerulonephritis with diffuse mesangial widening -Focal & Segmental mesangial widening -Hematuria |
What Nephritic Syndrome is this?
How do you know? What would be the usual presentation with this? |
|
|
IgA Nephropathy
-IgA is deposited mainly within the Mesangium -Focal Proliferative Glomerulonephritis with diffuse mesangial widening |
What Nephritic Syndrome would this be?
|
|
|
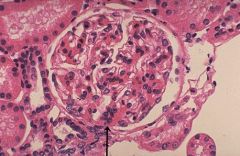
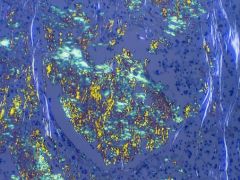
IgA Nephropathy (Berger Disease)
-MESANGIAL deposits of IgA and C3 |
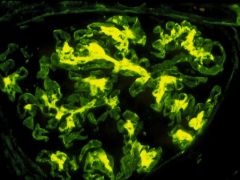
What Nephritic Syndrome is this?
|
|
|
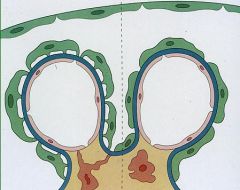
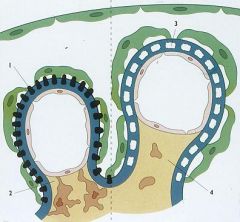
IgA Nephropathy = proliferative mesangial disease
-there are 2 mesangial cells -normally there is 1 mesangial cell per 3 capillary loops |
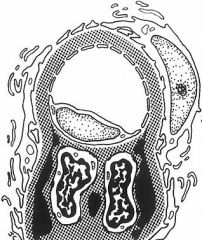
What is this schematic showing?
|
|
|
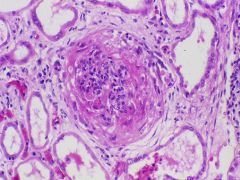
Rapidly Progressive Glomerulonephritis = Crescentic Glomerulonephritis
-crescent-shaped proliferation of parietal epithelial cells encroaching on the glomerulus |
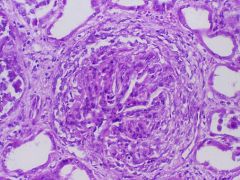
What is this Nephritic Syndrome?
|
|
|
Goodpastures's Syndrome
Type II = Cytotoxic = Auto-Ab's directed toward GBM |
What is this typical of?
What type of Hypersensitivity Reaction? |
|
|
Goodpasture Syndrome
-Anti-GBM Ab's cause focal fibrinoid necrosis where rupture occurs and fibrin leaks out thru the BM |
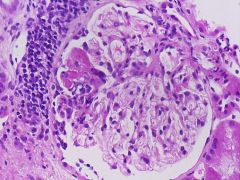
Explain this slide
|
|
|
Male dominant Rapidly Progressive Glomerulonephritis Nephritic Syndrome with a LINEAR IF
|
Goodpasture Syndrome
-fibrinoid necrosis of GBM |
|
|
Goodpasture Syndrome
-hypercellularity -crescents -fibrin |
What disease?
|
|
|
Goodpasture Syndrome
-glomerulus is hyalinized due to Anti-GBM Ab's = Hyaline leaks out from the capillaries |
What disease?
|
|
|
-Goodpasture Syndrome
- Capillary loops are being compressed by the Crescent -GFR will decrease to ZERO in a couple weeks = Rapid Progressive Glomerulonephritis |
What disease?
What process is happening? What does this cause? |
|
|
Normal Kidney
-one mesangial cells per 3 capillary loops |
What is this?
|
|
|
Minimal Change Nephropathy
-fused foot processes of the epithelial cells |
Pathology seen on the right
|
|
|
Minimal Change Disease (Lipoid Nephrosis = Nil Disease)
-Fused foot processes |
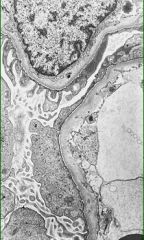
What Nephrotic Syndrome is this?
|
|
|
Focal Segmental Glomerulosclerosis
-Sclerosis within capillary tufts of deep JG glomeruli HIV, AIDS, Obesity, Sickle Cell |
What Nephrotic Syndrome is this?
What is it associated with? |
|
|
Membranous Nephropathy
|
Nephrotic Syndrome associated with these 2 pathologies
|
|
|
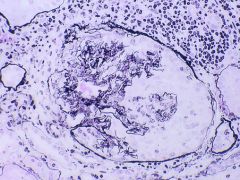
Membranous Nephropathy
-diffuse capillary wall thickening and basemement membrane thickening -there is NO hypercellularity |
What Nephrotic Syndrome is this?
|
|
|
Membranous Nephropathy
-capillary wall and basement membrane thickening -NO hypercellularity |
What Nephrotic Syndrome is this?
|
|
|
Membranous Nephropathy
-immune-complex deposition in SUBEPITHELIAL locations |
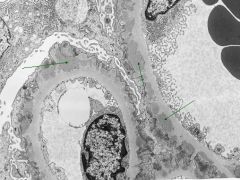
What Nephrotic Syndrome is this?
|
|
|
IgG and C3 deposits
|
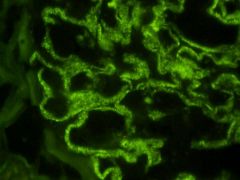
This is Membranous Glomerulonephropathy. What is deposited in the Subepithelium?
|
|
|
What is deposited in the Sclerotic lesions in Focal Segmental Glomerulosclerosis?
|
IgM & C3
**vs. IgG/C3 for Membranous Nephropathy |
|
|
Membranous Glomerulonephritis
-Spike-and-Dome appearance on Silver Methenamine stain |

What Nephrotic Syndrome is this?
|
|
|
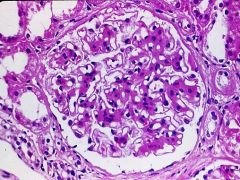
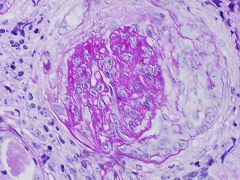
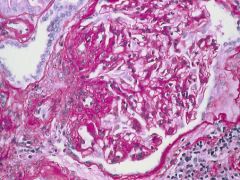
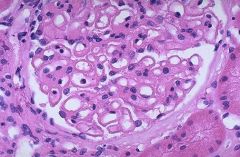
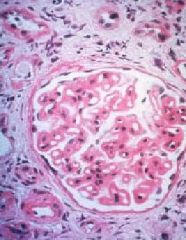
Diabetic Glomerulosclerosis
Nodular Sclerosis = Kimmelstiel-Wilson nodules -nodular accumulation of mesangial matrix material |
What Nephrotic Syndrome is this?
What is the pathology? |
|
|
Diabetic Nephropathy
-Diffuse Glomerulosclerosis = diffusely distributed increase in mesangial matrix -Hyalinization of Efferent and Afferent Arterioles |
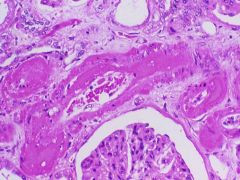
What Nephrotic Syndrome is this?
|
|
|
Hyalinized Arterioles due to Diabetic Nephropathy
Hypertension |
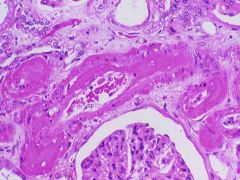
What is seen here?
What is the consequence? |
|
|
1. Necrotic Renal Papilla
2. Diabetic nephropathy 3. Drops off and falls into Calyx -> RENAL COLIC = contraction of the ureter b/c it contains foreign material |
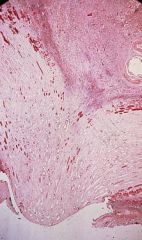
What is this?
What is the cause? How might it manifest clinically? |
|
|
Amyloidosis
Congo Red stain which when polarized under the light microscope results in an APPLE GREEN BIREFRINGENCE pattern |
What is the cause of this?
What stain? |
|
|
Accumulations of cells composed of proliferating Parietal Epithelial Cells and infiltrating Leukocytes
|
Crescents
|
|
|
What has proliferated to form Crescents in Rapidly Progressive GN?
|
Parietal epithelial cells
|
|
|
Type of Glomerulonephritis defined by the lack of anti-GBM Ab's or Immune-complexes by immunofluorescence and EM. Most patients with this type of Rapidly Progressive GN have Antineutrophil Cytoplasmic Antibodies (ANCA), which play a role in some vasculitides
|
Pauci-immune = ANCA granulonephritis
-Wegener Granulomatosis (c-ANCA) |
|
|
Nephritic that is usually progressive over a matter of weeks and culminates in severe oliguria
|
Crescentic GN = Rapidly Progressive GN
|
|
|
List the diseases associated with Nephritic Syndrome
|
1. Post-streptococcal GN
2. Rapidly Progressive GN 3. Membranoproliferative GN 4. IgA Nephropathy |
|
|
Unlike Nephritic Syndrome, what 3 things does Nephrotic Syndrome not have?
|
1. Hematuria
2. Oliguria 3. Hypertension |
|
|
Unlike Nephrotic Syndrome, what 2 things does Nephritic Syndrome not have?
|
1. Hyperlipidemia
2. Lipiduria |
|
|
What is the initial event leading to Nephrotic Syndrome?
|
derangement in Glomerular Capillary Walls resulting in INCREASED PERMEABILITY TO PLASMA PROTEINS
-low-weight proteins, such as albumin |
|
|
What is the initial event leading to Nephritic Syndrome?
|
inflammatory RUPTURE of glomerular capillaries with resultant bleeding into the urinary space
|
|
|
Sclerosis of some, but not all, glomeruli & only a portion of the capillary tuft is involved
|
Focal Segmental Glomerulosclerosis
|
|
|
Membranous Glomerulonephropathy
-diffuse thickening of capillary wall -NO cellular proliferation |
What Nephrotic Syndrome is this?
|
|
|
Diabetes causes Hyalinizing Arteriolar Sclerosis and increases the susceptibility to the development of these 2 Kidney lesions
|
1. Pyelonephritis
2. Papillary Necrosis |
|
|
Focal proliferative Glomerulonephritis with Diffuse Mesangial widening
|
IgA Nephropathy = Berger Disease
|