Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
74 Cards in this Set
- Front
- Back
|
Defien Acute Lymphoblastic Leukemia
|
Bone Marrow neoplasm of Lymphoid Stem cells
|
|
|
This is the most commmon malignancy of children
|
Acute Lymphoblastic Leukemia
|
|
|
Leukemia that is most responsive to therapy and may spread to CNS and testes
|
Acute Lymphoblastic Leukemia
|
|
|
What is a known etiology of Acute Lymphoblastic Leukemia?
|
Several chromosomal abnormalities
-t(9;22) is seen in very aggressive cases |
|
|
What is the blood pathology in ALL?
|
Pancytopenia = due to proliferation of blasts in BM
Lymphoblasts |
|
|
What is the Bone Marrow pathology in ALL?
|
1. Increased Lymphoblasts
-Terminal Deoxynucleotidyltransferase (TdT) -B cell phenotype (CD19, CD20) 2. Decreased normal hematopoiesis |
|
|
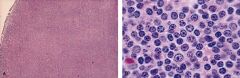
Histologically how do you differentiate between ALL and AML?
|
ALL = lymphoblasts show more condensed nuclear chromatic and small to absent nucleoli; scant cytoplasm
AML = myeloblasts have more dispersed nuclear chromatic; large nucleoli; abundant cytoplasm |
|
|
What are the clinical features of ALL?
|
1. occurs in Children
2. Bone Marrow failure 3. Splenomegaly 4. Lymphadenopathy 5. Focal neurological deficits = due to CNS infiltration 6. Testicular mass |
|
|
This is a marker of immature T and B lymphocytes and is present in 95% of ALL cases
|
TdT
|
|
|
What are the B cell antigens in ALL?
|
1. CALLA = common acute lymphoblastic leukemia antigen
2. CD19 3. CD20 |
|
|
What is the prognosis for ALL?
|
Cure rate = 70%
|
|
|
What are poor features to have in ALL?
|
<2 or >10 in age
t(9;22) ** = unfavorable prognosis |
|
|
What is the treatment for ALL?
|
1. Multiagent chemo
2. BM transplant **radiation might want to be used if ALL has infiltrated the CNS or Testes due to Blood-barriers |
|
|
A 6-year-old boy presents to your office complaining of fatigue, fever, and history of recurrent epistaxis and UTI's. He has an enlarged liver and spleen and a petechial rash over his entire body. Concerned, you send him for some blood tests, which demonstrate pancytopenia with the presence of multiple blasts. You fear that a bone marrow biopsy may demonstrate cells that would stain positive for TDT and CALLA
|
Acute Lymphoblastic Leukemia
|
|
|
What is the definition of Chronic Lymphocytic Leukemia?
|
Mature CD5 B cell neoplasm
Blood lymphocytosis **CD5 is normally seen in T lymphocytes |
|
|
This is the most common Leukemia in adults
|
Chronic Lymphocytic Leukemia
|
|
|
What is the pathogenesis of Chronic Lymphocytic Leukemia?
|
Several chromosomal abnormalities
|
|
|
What is the blood pathology seen in CLL? (3)
|
1. increased Small mature lymphocytes (>4000/uL)
2. Increased Smudge cells 3. Anemia, neutropenia, thrombocytopenia |
|
|
Smudge cells
|
Chronic Lymphocytic Leukemia
|
|
|
What are the clinical features of Chronic Lymphocytic Leukemia?
|
1. Elderly MALES (>60)
2. Asymptomatic, generalized lymphadenopathy 3. Hepatosplenomegaly |
|
|
What are the possible complications in CLL? (4)
|
1. Warm autoimmune hemolytic anemia --> spherocytes
2. Hypogammaglobulinemia --> bacterial infections 3. Prolymphocytic Leukemia transformation --> neoplasm that becomes more acute and like ALL 4. transformation into Diffuse Large B cell Lymphoma = Richter's Syndrome |
|
|
What is the prognosis of CLL?
|
median survival is 5 years
|
|
|
What is the treatment for CLL?
|
Palliative = Fludarabine, Rituximab, Campath-1H
- there is NO cure - drugs relieve symptoms |
|
|
A 67-year-old man presents to your office for his annual check-up. You learn that he has been very tired, has had several nose bleeds over the past 6 months, and that he has also noticed a few lumps on his neck. Phsical exam reveals Lymphadenopathy and Hepatosplenomegaly. You order peripheral blood smear, which demonstrates multiple smudge cells.
|
Chronic Lymphocytic Leukemia
-Elderly man -Pancytopenia = fatigue, bleeding, infections -generalized Lymphadenopathy |
|
|
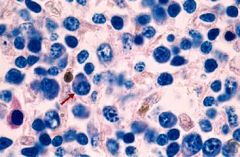
Diagnostic stain is Tartrate-resistant Acid Phosphatase (TRAP)
|
Hairy Cell Leukemia
|
|
|
Treatment for this disease is 2-chlorodeoxyadenosine, which is very effective
|
Hairy Cell Leukemia
|
|
|
Define Hair Cell Leukemia
|
Mature B cell neoplasm of bone marrow, spleen, blood
Small lymphocytes with hair-like cytoplasmic projections |
|
|
Bone marrow fibrosis causing a "dry tap" when performing bone marrow biopsy
Pancytopenia, splenomegaly, and infections with Atypical Mycobacteria Expression of CD11c and CD25 |
Hairy Cell Leukemia
|
|
|
Define Multiple Myeloma
|
Monoclonal Plasma Cell neoplasm with multifocal bone marrow involvement
|
|
|
Describe the pathogenesis of Multiple Myeloma
|
Plasma cell proliferation under the influence of IL-6 or HHV-8
Plasma cells lead to bone demineralization by secreting osteoclast activators IL-6 and IL-1beta |
|
|
What bone marrow pathologies are seen in Multiple Myeloma?
|
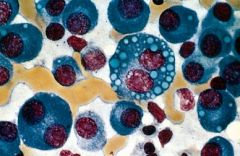
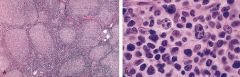
1. Plasmacytosis (>10%)
2. Plasma cell atypia (nucleoli) 3. Decreased normal hematopoiesis |
|
|
What bone pathologies are seen in Multiple Myeloma?
|
Osteolytic bone lesions = "punched-out" lesions
|
|
|
What pathology is seen in the blood in Multiple Myeloma?
|
1. Monoclonal M protein spike
-IgG (55%) -IgA (25%) |
|
|
What urine pathology is seen in Multiple Myeloma?
|
Free monoclonal light chains = Bence-jones proteins
|
|
|
What kidney pathologies are seen in Multiple Myeloma?
|
1. Light chain cast nephropathy
2. Glomerulonephropathy |
|
|
Bone marrow showing neoplastic Plasma Cells with "fried egg" appearance
|
Multiple Myeloma
|
|
|
What are the clinical features of Multiple Myeloma?
|
1. Bone pain
2. Hypercalcemia 3. Anemia = due to crowding of BM by proliferating Plasma Cells 4. Renal failure 5. Infection = due to suppression of normal Ig's |
|
|
What is the prognosis of Multiple Myeloma?
|
Median survival is 4 years
|
|
|
What is the treatment for Multiple Myeloma?
|
1. Melphalan + Prednisone
2. BM transplant = can extend survival to about 8 years |
|
|
A 69-year-old man presents with severe pain in his back. Upon history he reveals that he has been extremely tired and has suffered from several UTI's over past 4 months. An x-ray of his back reveals fractures in the L2 & L3 vertebrae as well as punched-out lytic bone lesions in several other vertebrae. When urine alaylsis suggests proteinuria and peripheral blood smear demonstrates rouleaux formation of RBC's, you admit him the oncology for further evaluation
|
Multiple myeloma
|
|
|
Blood smear demonstrates Rouleaux formation of RBC's (roll of coins looking)
|
Multiple Myeloma
|
|
|
Non-contiguous spread: Non-hodgkins or Hodgkins?
|
Non-Hodgkins
|
|
|
List the general features of Non-Hodgkin Lymphoma
|
1. B or T lymphocyte neoplasm
2. originate in lymph nodes or extranodal lymphoid tissue 3. localized or generalized lymphadenopathy 4. non-contiguous spread 5. nodular or diffuse growth pattern histologically |
|
|
Describe Low Grade Non-Hodgkin Lymphoma clinical behavior
|
1. Slow progression (>10 year survival)
2. INCURABLE |
|
|
Describe High Grade Non-Hodgkin Lymphoma
|
1. Rapid progression (< 1 year survival)
2. CURABLE |
|
|
List the 4 Low Grade Non-Hodgkin Lymphomas
|
1. SMall Lymphocytic Lyphoma
2. Lymphoplasmacytoid Lymphoma 3. Follicular Lymphoma 4. Marginal Zone Lymphoma (MALToma) |
|
|
List the 2 Intermediate Grade Non-Hodgkin Lymphomas
|
1. Mantle Cell Lymphoma
2. Diffuse Large B-cell Lymphoma |
|
|
List the 2 High Grade Non-Hodgkin Lymphomas
|
1. Lymphoblastic Lymphoma
2. Burkitt Lymphoma |
|
|
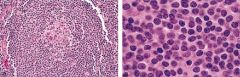
Diffuse infiltrate of small mature Lymphocytes and mimics CLL morphologically and clinically
|
Small Lymphocytic Lymphoma
|
|
|
Hyperviscosity syndrome most often associated with IgM-producing plasmacytic lymphocytes (hybrids of plasma cells and B lymphocytes)
|
Waldenstrom Macroglobulinemia = Lymphoplasmacytoid Lymphoma
|
|
|
Diffuse infiltrate of small round lymphocytes with scattered plasma cells
|
Waldenstrom Macroglobulinemia = Lymphoplasmacytoid Lymphoma
**SLL only has Small round lymphocytes |
|
|
A 72-year-old man presents to your office complaining of fatigue, blurry vision, headaches, and weight loss over the past 6 months. Physical exam reveals hepatosplenomegaly, generalized lymphadenopathy, and retinal vascular dilation. An abdominal x-ray and urinalysis and normal, although blood tests demonstrate anemia and increased serum viscosity.
|
Waldenstrom Macroglobulinemia = Lymphoplasmacytoid Lymphoma
|
|
|
Russell bodies (cytoplasmic eosinophilic Ig inclusion bodies) & Dutcher bodies (intranuclear Ig)
|
Waldenstrom Macroglobulinemia = Lymphoplasmacytoid Lymphoma
|
|
|
Neoplastic nodules of small CLEAVED lymphocytes derived from germinal center B cells of secondary follicles
|
Follicular lymphoma
|
|
|
BCL-2 proto-oncogene overexpression from a t(14;18) translocation resulting in inhibited apoptosis
|
Follicular lymphoma
|
|
|
What is the translocation in Follicular Lymphoma?
|
t(14:18)
**bcl-2 = inhibits Apoptosis |
|
|
Most common Lymphoma in adults
|
Follicular Lymphoma
|
|
|
What are the sites of origin of Marginal Zone Lymphomas (MALTomas)
|
MALT
-Stomach due to H. pylori -Thyroid due to Hashimoto Thyroiditis -Salivary gland due to Sjogren syndrome 2. Lymph node or spleen |
|
|
Diffuse infiltrate of Small mature B lymphocytes
-mimics SLL histologically, but is CD5 negative |
Marginal Zone Lymphoma = MALToma
|
|
|
Neoplastic nodules of small irregular lymphocytes derived from Mantle Zone B-cells of secondary follicles
|
Mantle Cell Lymphoma
|
|
|
t(11:14) translocation
|
Mantle Cell Lymphoma
-Bcl-1 = Cyclin D1 = Chromosome 11 -Ig heavy chain = chromosome 14 |
|
|
What is the translocation in Mantle Cell Lymphoma?
|
t(11;14)
-Cyclin D1 (BCL-1) |
|
|
Define "Diffuse Large B cell Lymphoma"
|
Diffuse infiltrate of large lymphocytes (4x normal size)
|
|
|
What are the 2 subtypes of Diffuse Large B cell Lymphoma
|
1. Immunodeficiency Associated Lymphoma
-HIV or post-transplant -pathogenesis involves EBV 2. Body Cavity Lymphoma -pathogenesis involves HHV-8 -tumor is limited to Pleural or Ascitic fluid |
|
|
Left = ALL
Right = AML |
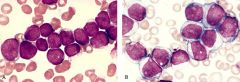
What is on the Left? Right?
|
|
|
CLL
-Smudge cells -Lymphocytosis |
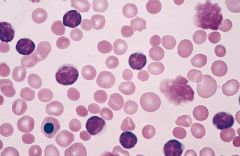
What disease? How do you know?
|
|
|
Hairy Cell Leukemia
|
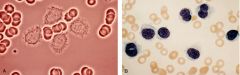
What disease?
|
|
|
Multiple Myeloma
|

What disease?
|
|
|
Multiple Myeloma
-"Fried egg" Plasma cells in the BM |
What disease?
|
|
|
Small Lymphocytic Lymphoma
-complete effacement of lymph node architecture -back to back cells with round nuclei |
What disease?
|
|
|
Waldenstrom Macroglobulinemia
-Small round lymphocytes with the presence of Plasma Cells |
What disease?
|
|
|
Follicular Lymphoma
t(14;18) = bcl-2 expression |
What disease?
What translocation? |
|
|
Mantle Cell Lymphoma
t(11;14) = cyclin D1 (bcl-1) |
What disease?
What translocation? |
|
|
Diffuse Large B cell Lymphoma
|
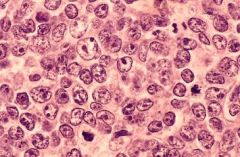
What disease?
|