Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
45 Cards in this Set
- Front
- Back
|
What are the types of liver lesions?
|
Primary
- 3 Benign - 2 Malignant Metastatic (1) 3:2:1 |
|
|
What are the types of Benign Primary liver lesions?
|
- Hemangioma
- Focal Nodular Hyperplasia (FNH) - Adenoma |
|
|
What are the types of Malignant Primary liver lesions?
|
- Hepatocellular Carcinoma (HCC)
- Cholangiocarcinoma (CCA) |
|
|
If a patient tells you they are on oral contraceptives, what kind of liver lesion are you worried about?
|
Hepatic Adenoma
|
|
|
If a patient tells you they have a history of extra-hepatic malignancies, what kind of liver lesion are you worried about?
|
Metastatic liver lesion
|
|
|
If a patient tells you they have underlying liver disease, what kind of liver lesion are you worried about?
|
Hepatocellular Carcinoma (HCC)
|
|
|
If a patient tells you they have a history of primary sclerosing cholangitis (PSC), what kind of liver lesion are you worried about?
|
Cholangiocarcinoma (CCA)
|
|
|
In a non-cirrhotic liver, what are the most common causes of liver lesions?
|
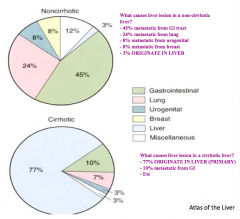
- 45% metastasize from GI tract
- 24% metastasize from lung - 8% metastasize from urogenital tract - 8% metastasize from breast ONLY 3% originate in liver |
|
|
In a cirrhotic liver, what are the most common causes of liver lesions?
|
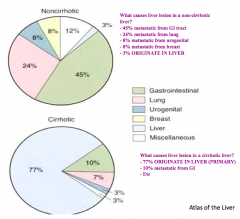
77% originate in liver
- 10% metastasize from GI - 7% metastasize from lung - 3% metastasize from urogenital tract |
|
|
How does the presence of cirrhosis in the liver help you predict what type of cancer is in the liver?
|
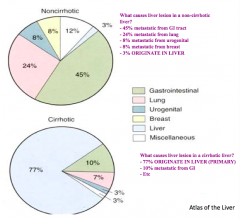
- Non-cirrhotic: most likely to be a metastases from elsewhere (only 3% originate in liver)
- Cirrhotic: most likely to be a primary lesion (77% originate in liver) |
|
|
What is the most common benign liver lesion?
|
Hemangioma (found in 1% of all autopsies)
|
|
|
Will you find cirrhosis with Hemangiomas?
|
No - they are primarily found in non-cirrhotic livers
|
|
|
What are Hemangiomas? Size?
|
- Congenital vascular malformations (blood-filled cavities lined by endothelium)
- Range from 1-20 cm (>10 cm called a "giant hemangioma") |
|
|
When are most Hemangiomas diagnosed?
|
- Majority during 3rd-5th decade
|
|
|
Are Hemangiomas unitary lesions or do they present with multiple lesions?
|
- Unitary in 70% of cases
- Multiple in 30% of cases |
|
|
What is the risk for malignancy with a Hemangioma?
|
NO malignant potential!
|
|
|
What symptoms are caused by Hemangiomas?
|
Mostly asymptomatic unless they are at the surface of the liver and stretch the capsule
|
|
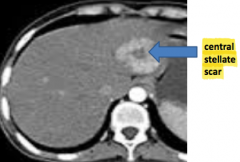
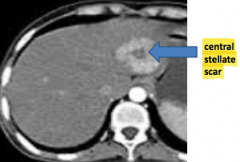
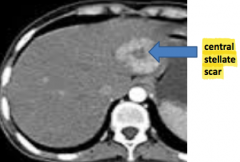
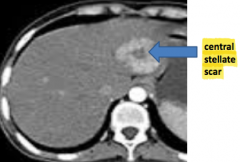
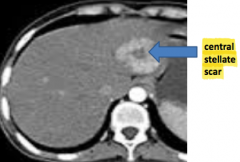
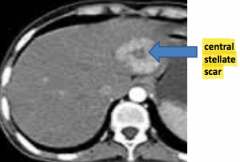
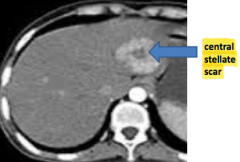
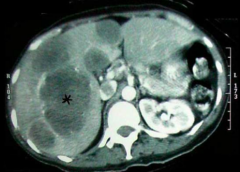
What kind of liver lesion is this?
|
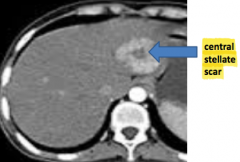
Focal Nodular Hyperplasia (FNH) - benign
|
|
|
What is the second most common benign liver lesion?
|
Focal Nodular Hyperplasia (FNH)
|
|
|
Will you find cirrhosis in patients with Focal Nodular Hyperplasia (FNH)?
|
No - FNH is found in non-cirrhotic livers
|
|
|
What causes Focal Nodular Hyperplasia (FNH)?
|

- Reaction to intra-hepatic anomolous artery leading to hyper-perfusion
- Hyper-perfused area enlarges until it outgrows it's blood supply |
|
|
Who is most commonly affected by Focal Nodular Hyperplasia (FNH)?
|
- Women
- Ages 20-50 |
|
|
What is the size of Focal Nodular Hyperplasia (FNH)?
|
Majority < 5 cm (rarely exceeds 10 cm)
|
|
|
Does Focal Nodular Hyperplasia (FNH) present as a unitary lesion or does it present with multiple lesions?
|
- Unitary in 80-90% of cases
- Multiple in 10-20% |
|
|
What risk for malignancy is there with Focal Nodular Hyperplasia (FNH)?
|
NO malignant potential
|
|
|
What is the third most common benign liver lesion?
|
Hepatic Adenoma
|
|
|
Is there cirrhosis in livers with Hepatic Adenoma?
|
No - found in non-cirrhotic livers
|
|
|
What is a Hepatic Adenoma?
|
Benign proliferation of hepatocytes
|
|
|
Who is primarily affected by Hepatic Adenoma?
|
- Majority in women of child-bearing age
- Associated with contraceptive use - Glycogen storage disease - Diabetes Mellitus |
|
|
What is there a risk for in Hepatic Adenoma, unlike in Hemangiomas and Focal Nodular Hyperplasia (FNH)?
|
- Hemorrhage
- Malignant transformation |
|
|
What type of liver lesion is associated with pregnancy? What can happen?
|
Hepatic Adenoma - growth and rupture can occur during pregnancy
|
|
|
How do you treat Hepatic Adenoma?
|
- Contraceptives should be discontinued (associated w/ contraceptive use)
- Avoid pregnancy (this could lead to growth and rupture of adenoma) - Surgical resection to avoid risk of cancer and tumor rupture |
|
|
Where is there higher incidence of Hepatocellular Carcinoma?
|
- China
- Parts of Africa - SE Asia |
|
|
How has the incidence and 5-year survival of Hepatocellular Carcinoma changed in the last 40 years?
|
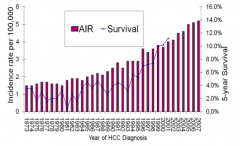
- Cases of HCC is increasing
- 5-year survival is increasing |
|
|
What ethnicity is HBV most frequent in? HCV?
|
- HBV most frequent in Asians
- HCV most frequent in Non-Asians |
|
|
What are the most common viral causes of Hepatocellular Carcinoma?
|
- HCV - 47% of cases
- HBV - 15% of cases |
|
|
What happens to the blood flow in Hepatocellular Carcinoma?
|
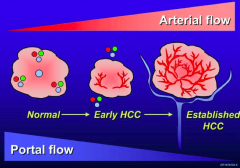
- Normal: blood flow is 70% from portal vein and 30% hepatic artery blood flow
- HCC: switches so that 95% of blood flow supplied by arterial blood and only 5% from portal vein |
|
|
What happens in Hepatocellular Carcinoma when a radiologist infuses IV contract?
|
- First 60 seconds is the arterial phase (where contrast goes first) - lights up the cancer
- Arterial blood flow disappears and venous blood flow goes away and now it is hard to see the lesion |
|
|
Which protein is elevated in 60-70% of patients with Hepatocellular Carcinoma? How much?
|
Alpha Fetoprotein (AFP) - > 200 ng/mL
|
|
|
Where is Alpha Fetoprotein (AFP) produced? When is it elevated?
|
- Produced by fetal liver and placenta
- Elevated in 60-70% of patients w/ HCC - Can be elevated w/ hepatic inflammation or cirrhosis in the absence of HCC |
|
|
What diagnostic features are consistent with a diagnosis of Hepatocellular Carcinoma?
|
- Alpha Fetoprotein (AFP) > 200 ng/mL
- Liver lesion on imaging Don't need to biopsy!! |
|
|
How do you prevent Hepatocellular Carcinoma?
|
- HBV vaccination
- Treatment of viral hepatitis - Coffee? |
|
|
What are the most common primary sites that metastasize to the liver?
|
- GI: colon, pancreas, esophageal, gastric
- Lung - Urogenital - Breast - Melanoma |
|
|
Why are pseudocysts not true cysts?
|
- Lack of epithelial lining (fibrous and granulation tissue)
- No malignant potential |
|
|
How do you classify pancreatic cysts?
|
Non-neoplastic, benign:
- True cysts - Retention cysts - Mucinous, non-neoplastic cysts - Lymphoepithelial cysts |