Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
153 Cards in this Set
- Front
- Back
|
What is the term for gallbladder inflammation?
|
Cholecystitis
|
|
|
What are the clinical manifestations of Acute Cholecystitis?
|
- Prolonged (>4-6 hours), steady RUQ pain / epigastric pain
- Pain may radiate to the shoulder or back - Fever - Leukocytosis - Gallbladder inflammation - Abdominal guarding - Murphy's sign |
|
|
What is Acute Cholecystitis typically associated with?
|
- Gallstones (calculous and xanthogranulomatous)
- Sometimes acalculous |
|
|
What is Chronic Cholecystitis typically associated with?
|
Almost always associated w/ gallstones
|
|
|
What happens in Chronic Cholecystitis?
|
- Chronic inflammatory cell infiltration
- Almost always associated w/ gallstones - No correlation w/ symptoms - Mechanical irritation or recurrent acute cholecystitis → fibrosis |
|
|
What is one type of Chronic Cholecystitis?
|
Porcelain gallbladder
|
|
|
What is the pathogenesis of Acute Cholecystitis?
|
- Cystic duct obstruction in addition to additional irritant → release of inflammatory mediators (prostaglandins?)
|
|
|
What pain occurs in Acute Cholecystitis?
|
- Prolonged (>4-6 hours), steady RUQ and epigastric pain
- Pain may radiate to the shoulder or back |
|
|
What abdominal physical exam findings are there in Acute Cholecystitis?
|
- Abdominal guarding: associated w/ local parietal peritoneal inflammation
- Murphy's sign: increased discomfort when patient takes a deep breath in while examiner palpates RUQ |
|
|
What lab findings are not common in Acute Cholecystitis?
|
Elevated bilirubin and elevated alkaline phosphatase are not common
|
|
|
What imaging is done to diagnose Acute Cholecystitis?
|
- Abdominal ultrasound
- Cholescintigraphy / HIDA scan - CT |
|
|
What are you looking for on abdominal ultrasound to diagnose Acute Cholecystitis? How sensitive / specific is this test?
|
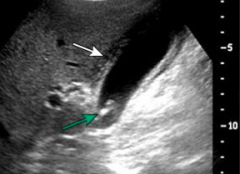
- Cholelithiasis (gallstones in gallbladder)
- Gallbladder wall thickening >4-5 mm or edema - Sonographic Murphy's sign (increased discomfort when patient takes deep breath while palpating RUQ) - 88% sensitive and 80% specific |
|
|
What are you looking for on Cholescintigraph / HIDA scan to diagnose Acute Cholecystitis?
|

- Labeled HIDA injected intravenously → taken up by hepatocytes → excreted in bile
- If there is no visualization of the gallbladder it is d/t cystic duct obstruction |
|
|
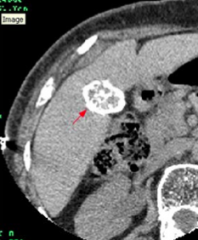
What are you looking for on CT to diagnose Acute Cholecystitis? How sensitive / specific is this test?
|
- Gallbladder wall edema
- Pericholecystic stranding and fluid - High-attenuation bile - Can be particularly useful when complicated cholecystitis is suspected - Not a good modality to detect gallstones |
|
|
What is CT not good at detecting related to the gallbladder?
|
Poor at detecting gallstones
|
|
|
What is the most common complication of Acute Cholecystitis?
|
Gangrene
|
|
|
What are the possible complications of Acute Cholecystitis?
|
- Gangrene
- Perforation (may lead to abscess) - Cholecystoenteric fistula - Emphysematous cholecystitis |
|
|
When do perforations usually occur in Acute Cholecystitis?
|
- After development of gangrene
- May result in an abscess |
|
|
Where can a Cholecystoenteric Fistula (complication of Acute Cholecystitis) lead to?
|
- Usually leads to the duodenum or jejunum
- A gallstone could pass through the fistula ("gallstone ileus") which could cause mechanical bowel obstruction in terminal ileum |
|
|
What is gallstone ileus?
|
- Passage of gallstone through fistula
- Leads to a mechanical bowel obstruction usually in the terminal ileum - Caused by cholecystoenteric fistula (a complication of Acute Cholecystitis) |
|
|
What is Emphysematous Cholecystitis?
|
- Secondary infection of gallbladder wall w/ gas-forming organisms
- Usually leads to gangrene and perforation - Complication of Acute Cholecystitis |
|
|
How do you treat Acute Cholecystitis?
|
- May ablate (surgically remove) in 7-10 days if not treated
- Antibiotics - Pain control: NSAIDs, opioids - Gallbladder drainage (percutaneous cholecystostomy, endoscopy) - Surgery |
|
|
When should you do surgery for treating Acute Cholecystitis?
|
- Immediate cholecystectomy for patients w/ complications or who are low risk
- Delayed cholecystectomy in high risk patients (eg, severe chronic illness, low-risk patient w/ sepsis) |
|
|
What is the prognosis of Acute Cholecystitis?
|
~3% mortality
- <1% in young healthy patients - Up to 10% in high-risk patients or those w/ complications |
|
|
What can cause Acalculous Cholecystitis?
|
Gallbladder stasis and ischemia → local inflammatory response → secondary infection
|
|
|
What are the clinical manifestations of Acalculous Cholecystitis?
|
- Unexplained fever
- Leukocytosis - Abdominal pain - Non-specific liver test elevations - May present similarly to calculous cholecystitis |
|
|
Who is at risk for Acalculous Cholecystitis?
|
Typically seen in hospitalized, critically ill patients
|
|
|
What lab tests can you do to diagnose Acalculous Cholecystitis?
|
- Abdominal US: no cholelithiasis (gallstones), gallbladder wall thickening > 3mm, sonographic Murphy's sign, pericholecystic fluid
- HIDA scan: lack of gallbladder visualization - CT |
|
|
How do you treat Acalculous Cholecystitis?
|
- Antibiotics
- Percutaneous cholecystostomy - Cholecystectomy (not typically required once underlying problem is addressed, only if the cholecystostomy does not lead to improvements or is contraindicated) |
|
|
When would a cholecystectomy be indicated for treating Acalculous Cholecystitis?
|
- If cholecystostomy does not result in clinical improvement
- If cholecystostomy is contraindicated - Typically not required once underlying problem is addressed |
|
|
What is the prognosis for Acalculous Cholecystitis?
|
- High mortality (75%) w/ delayed treatment
- Overall mortality of 30% |
|
|
What is the term for extravasation of bile into the gallbladder wall?
|
Xanthogranulomatous Cholecystitis
|
|
|
What happens in Xanthogranulomatous Cholecystitis?
|
- Extravasation of bile into the gallbladder wall → inflammatory reaction (fibroblasts and macrophages phagocytose biliary lipids in bile) → xanthoma cells
- Gallstones present in ALL patients |
|
|
What kinds of cells phagocytose biliary lipids in bile in Xanthogranulomatous Cholecystitis? What does this lead to?
|
- Fibroblasts and Macrophages phagocytose biliary lipids in bile
- Leads to xanthoma cells |
|
|
What is the clinical presentation of Xanthogranulomatous Cholecystitis?
|
- History suggestive of Acute Cholecystitis
- Can mimic gallbladder cancer - High rate of complications |
|
|
What kind of complications can occur in Xanthogranulomatous Cholecystitis?
|
- Perforation
- Fistulas into adjacent structures - Abscess |
|
|
How do you diagnose Xanthogranulomatous Cholecystitis?
|
- Abdominal US: hypoechoic nodules or bands in gallbladder wall most characteristic
- CT: intramural hypodense nodules |
|
|
How do you treat Xanthogranulomatous Cholecystitis?
|
- Cholecystectomy (usually open)
- Pre-operative cholangiogram to exclude bile duct cancer |
|
|
What does Xanthogranulomatous Cholecystitis mimic?
|
Gallbladder cancer
|
|
|
What causes "Porcelain Gallbladder"?
|
Chronic cholecystitis w/ intramural calcification of gallbladder wall
|
|
|
How common is Porcelain Gallbladder? Who is more likely to get it?
|
- Uncommon (0.06-0.08%)
- More common in females (5:1) |
|
|
What is there increased risk of in Porcelain Gallbladder? What increases the risk?
|
Gallbladder cancer (0-62%) - incomplete calcification of gallbladder wall associated w/ higher risk than complete calcification
|
|
|
What is the clinical presentation of Porcelain Gallbladder?
|
- Asymptomatic
- Biliary type pain - Palpable gallbladder |
|
|
How do you diagnose Porcelain Gallbladder?
|
- Plain abdominal x-ray
- CT - Abdominal ultrasound |
|
|
How do you treat Porcelain Gallbladder?
|
- Cholecystectomy for incomplete calcification or symptomatic patients w/ complete calcification
- Consider cholecystectomy for asymptomatic patients w/ complete calcification |
|
|
When is Cholecystectomy definitely indicated for Porcelain Gallbladder? When should you only consider it?
|
- Indicated: incomplete calcification or for complete calcification in symptomatic patients
- Consider: complete calcification in asymptomatic patients |
|
|
How commonly are gallbladder polyps found when a patient undergoes a gallbladder US?
|
1.5-4.5%
|
|
|
What are the types of benign gallbladder polyps?
|
- Cholesterol
- Adenomyomatosis - Inflammatory - Adenomas |
|
|
What is found in benign cholesterol gallbladder polyps?
|
Abnormal deposits of TGs, cholesterol precursors, and cholesterol esters into the gallbladder mucosa
|
|
|
What is found in benign adenomyomatosis gallbladder polyps?
|
- Overgrowth of mucosa
- Thickening of muscle wall - Intramural diverticula |
|
|
Adenomyomatosis gallbladder polyps (benign) are associated with what? More common in what? Risk for cancer?
|
- Associated w/ cholelithiasis (gallstones)
- More common in women - No conclusive evidence of increased risk of GB cancer |
|
|
What is found in benign inflammatory gallbladder polyps?
|
Granulation and fibrous tissue w/ plasma cells and lymphocytes
|
|
|
What is found in benign adenoma gallbladder polyps? Relationship to cancer?
|
- Benign glandular tumors w/ potential for malignancy
- Likelihood of malignant transformation related to size: none less than 12 mm in one series |
|
|
What is the clinical presentation of gallbladder polyps?
|
- Asymptomatic / incidental finding
- Biliary pain - Possibly associated w/ dyspepsia w/ cholesterolosis and adenomyomatosis |
|
|
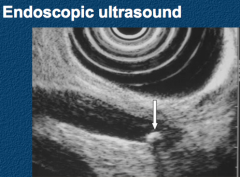
How do you diagnose gallbladder polyps?
|
- Transabdominal US
- Endoscopic US - CT (most useful in GB cancer) |
|
|
What is the most useful imaging tool for diagnosing gallbladder cancer?
|
CT
|
|
|
How do you manage gallbladder polyps? What are the criteria for this procedure?
|
Cholecystectomy
- Cholelithiasis irrespective of size of gallbladder polyps - Primary Sclerosing Cholangitis (PSC) irrespective of size of GB polyps - Biliary cholic (form of pain which starts and stops abruptly) or pancreatitis - Polyps >10 mm |
|
|
What is Acute Cholangitis?
|
- Infection of the bile duct (cholangitis)
- Usually caused by bacteria ascending from its junction with the duodenum - It tends to occur if the bile duct is already partially obstructed by gallstones |
|
|
Bacteria entering the small intestine or portal system via a disruption in the sphincter of Oddi causes what?
|
Acute Cholangitis
|
|
|
What infections are responsible for Acute Cholangitis? How does this infection occur?
|
G- and G+ colonic bacteria:
- E. coli (25-50%) - Klebsiella (15-20%) - Enterococcus species (10-20%) - Enterobacter species (5-10%) *Bacteria most likely enter via the Sphincter of Oddi |
|
|
What are the symptoms of Acute (Ascending) Cholangitis?
|
Charcot's Triad (50-75%):
- Fever - Jaundice - Abdominal pain Reynolds' Pentad: - Charcot's Triad + - Confusion - Hypotension |
|
|
What is the term for fever, abdominal pain, and jaundice in Acute Cholangitis? How commonly do these symptoms present?
|
Charcot's Triad (50-75%)
|
|
|
What is the term for fever, abdominal pain, jaundice, confusion, and hypotension in Acute Cholangitis? Implications?
|
Reynolds' Pentad (high morbidity and mortality)
|
|
|
What lab tests are seen in Acute Cholangitis?
|
- Cholestatic liver test elevations
- Leukocytosis |
|
|
How do you diagnose Acute Cholangitis?
|
- Clinical signs
- Imaging: dilated biliary system, choledocholithiasis |
|
|
How do you treat Acute Cholangitis?
|
- Antibiotics
- Biliary drainage (ERCP, PTC - percutaneous transhepatic cholangiography, or surgery) |
|
|
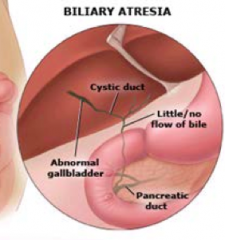
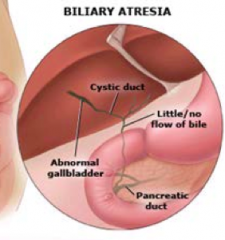
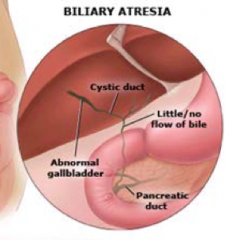
How does Biliary Atresia present?
|
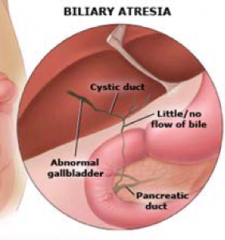
- Biliary obstruction exclusively in the neonatal period
- Progressive, idiopathic, fibro-obliterative disease of the extra-hepatic biliary tree *Complete obstruction of bile flow caused by destruction or absence of all or part of the extra-hepatic bile ducts |
|
|
Which part of the biliary tree is affected by Biliary Atresia?
|
Extra-hepatic region
|
|
|
What are the types of Biliary Atresia?
|
- Biliary Atresia: 70-85%
- Biliary Atresia Splenic Malformation (BASM): 10-15% |
|
|
How often does Biliary Atresia occur with other congenital malformation? Which ones?
|
5-10% associated w/ other congenital abnormalities:
- Intestinal atresia - Imperforate anus - Kidney anomalies - Heart malformations |
|
|
What are the possible causes of Biliary Atresia?
|
- Viral
- Toxic - Genetic (possibly in BASM subtype) - Immune dysregulation |
|
|
What is the clinical presentation of Biliary Atresia?
|
- Infant usually born full term, w/ normal birth weight, and initially they thrive
- Jaundice: birth to 8 weeks - Acholic stools - Dark urine |
|
|
How do you diagnose Biliary Atresia?
|
- Abdominal US
- Liver biopsy - Cholangiogram (intraoperative, PTC, endoscopic - ERCP) |
|
How do you treat Biliary Atresia?
|
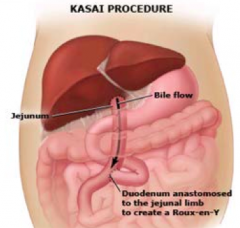
- Kasai procedure: perform ASAP, jejunum attached to liver to drain bile and duodenum is attached lower down on jejunum
- Liver transplantation |
|
|
When should a liver transplant be done for treatment of Biliary Atresia?
|
- 60-80% of patients w/ Biliary Atresia will eventually require a transplant despite optimal management
- Should be deferred as long as possible d/t improved outcomes w/ weights > 10 kg |
|
|
How does survival / prognosis improve when Biliary Atresia is treated with a liver transplantation?
|
Without transplant:
- 30-55% 5 year survival - 30-40% 10 year survival - 20-40% 20 year survival With transplant: - 92% 1 year survival - 70-80% 5-10 year survival Vastly improves prognosis! |
|
|
What are the characteristics of Biliary Cysts? Location?
|
Cystic dilations that may occur singly or in multiple throughout the biliary tree
|
|
|
What are most Biliary Cysts associated with?
|
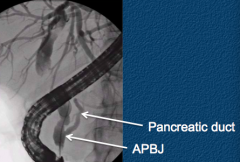
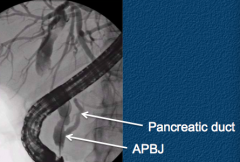
70% associated w/ Abnormal Pancreaticobiliary junction (APBJ)
- Pancreatic and bile duct join outside the duodenal wall |
|
|
What is an Abnormal Pancreaticobiliary Junction (APBJ)? What is it associated with?
|
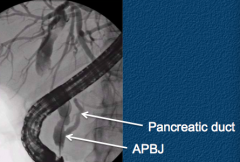
- Pancreatic and bile ducts join together outside the duodenal wall
- Associated with biliary cysts - Associated with increased risk of gallbladder cancer independent of biliary cysts |
|
|
How common are Biliary Cysts? In whom are they more common?
|
- 1:100,000 to 150,000
- More common (1:1000) in some Asian countries - More common in women (3-4:1) - Equal numbers in children and adults |
|
|
What are the types of Biliary Cysts? How common is each type? Location?
|
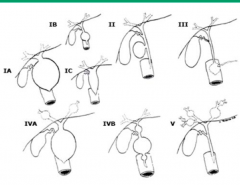
Type I:
- 50-85% - Extra-hepatic only Type IV: - 15-35% - Multiple cysts - Extrahepatic ± intrahepatic Type V: - 20% - Intrahepatic only - Assoc. w/ Caroli's disease |
|
|
Which type of Biliary Cyst is only found extra-hepatically? How common is it?
|
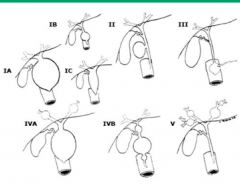
Type I (50-85%)
|
|
|
Which type of Biliary Cyst is found both extra-hepatically and intra-hepatically? How common is it?
|
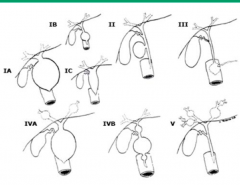
Type IV (15-35%)
- Multiple cysts |
|
|
Which type of Biliary Cyst is only found intra-hepatically? How common is it?
|
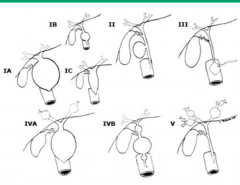
Type V (20%)
- Caroli's disease |
|
|
What is the cause / pathogenesis of Biliary Cysts?
|
- Possibly genetically or environmentally predisposed
- Can be associated w/ developmental anomalies - Can be congenital or acquired (from APBJ) |
|
|
What can Biliary Cysts be acquired from?
|
APBJ: Abnormal Pancreaticobiliary Junction
|
|
|
What are the clinical manifestations of Biliary Cysts?
|
- Majority present before age 10
- Infants: jaundice, failure to thrive, abdominal mass - Patients > age 2: chronic intermittent abdominal pain, pancreatitis, intermittent jaundice, cholangitis |
|
|
How do you diagnose Biliary Cysts?
|
- Abdominal US
- Cholangiography: ERCP, PTC, intraoperative, MRCP - CT |
|
|
What type of cancer is a patient with Biliary Cysts at increased risk for? How much is their risk increased?
|
20-30 fold increased risk for Cholangiocarcinoma
|
|
|
What types of Biliary Cysts are at increased risk for Cholangiocarcinoma?
|
- Type I and Type IV biliary cysts
- Increased risk confined to patients only w/ APBJ in one study |
|
|
What disease is caused by progressive inflammation, fibrosis, and stricturing of the intrahepatic and extrahepatic bile ducts?
|
Primary Sclerosing Cholangitis (PSC)
|
|
|
What can cause Secondary Sclerosing Cholangitis?
|
- Recurrent pyogenic cholangitis
- Choledocholithiasis - Cholangitis - AIDS cholangiopathy |
|
|
How common is Primary Sclerosing Cholangitis (PSC)? Who is more likely to get it?
|
- 1 in 100,000 persons
- 70% men - Mean age: 40 years - Women generally diagnosed later than men |
|
|
What is Primary Sclerosing Cholangitis (PSC) associated with?
|
Inflammatory Bowel Disease:
- Ulcerative Colitis (UC) > Crohn's Disease - Up to 90% of patients w/ PSC have UC - < 10% of patients w/ UC have PSC |
|
|
What is the cause / pathogenesis of Primary Sclerosing Cholangitis (PSC)?
|
- Immune activation: humoral and cellular abnormalities
- Genetic factors - Cystic fibrosis transmembrane conductance regulator mutations |
|
|
What are the clinical manifestations of Primary Sclerosing Cholangitis (PSC)?
|
- 50% asymptomatic
- Fatigue - Pruritus - Jaundice |
|
|
What are the lab results of a patient with Primary Sclerosing Cholangitis (PSC)?
|
- Elevated liver tests in a cholestatic pattern
- 30% Hypergammaglobulinemia - 40-50% increased IgM - 30-80% P-ANCA positive |
|
|
What areas of the bile ducts are affected by Primary Sclerosing Cholangitis (PSC)?
|
Classic PSC:
- Intrahepatic and extrahepatic (87%) - Intrahepatic alone (11%) - Rarely extrahepatic alone (2%) Small duct PSC: - Normal cholangiogram - Involves small caliber bile ducts |
|
|
How do you diagnose Primary Sclerosing Cholangitis (PSC)?
|
- CT
- Abdominal US - Cholangiography: MRI, ERCP - If cholangiogram is diagnostic, don't need liver biopsy - Consider liver biopsy for small-duct PSC |
|
|
What characteristic finding is seen on liver biopsy of Primary Sclerosing Cholangitis (PSC)?
|
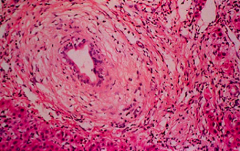
Onion skin pattern around bile ducts
|
|
|
What are the complications of Primary Sclerosing Cholangitis (PSC)?
|
- Progressive hepatic fibrosis → cirrhosis and portal HTN
- Decreased bile acids → steatorrhea and fat-soluble vitamin malabsorption - Osteoporosis (not d/t vitamin D malabsorption usually) - Dominant biliary strictures - Acute cholangitis - Cholelithiasis - Hepatobiliary and colon cancer |
|
|
What does the progressive hepatic fibrosis in Primary Sclerosing Cholangitis (PSC) lead to?
|
- Cirrhosis
- Portal HTN |
|
|
What does the decreased bile acids in Primary Sclerosing Cholangitis (PSC) lead to?
|
- Steatorrhea
- Malabsorption of fat-soluble vitamins |
|
|
What cancers are you at increased risk for if you have Primary Sclerosing Cholangitis (PSC)?
|
Hepatobiliary:
- Cholangiocarcinoma (10-15% lifetime risk) - Gallbladder (3-14% prevalence) - Hepatocellular in setting of cirrhosis Colon: - Approximately 4-fold increased risk w/ PSC and UC compared to UC alone |
|
|
How do you treat Primary Sclerosing Cholangitis (PSC)?
|
- Medical therapy not recommended
- ERCP for dominant extra-hepatic strictures - Surgery: biliary reconstruction (avoid if possible) or liver transplantation *Liver transplantation has better long-term outcomes, biliary reconstruction can complicate future liver transplantation surgery |
|
|
What gallbladder disease is associated with AIDS?
|
AIDS Cholangiopathy
|
|
|
What causes AIDS Cholangiopathy?
|
Biliary obstruction resulting from infection-related (classically Cryptosporidium parvum) strictures of the biliary tract
|
|
|
What AIDS patients are at risk for AIDS Cholangiopathy?
|
AIDS patients w/ CD4 count < 100 / mm3
|
|
|
What are the symptoms of AIDS Cholangiopathy?
|
- RUQ pain
- Epigastric pain - Diarrhea |
|
|
What lab tests are seen in AIDS Cholangiopathy?
|
Cholestatic liver enzyme elevations
|
|
|
How do you diagnose AIDS Cholangiopathy?
|
- Transabdominal US (high negative predictive value)
- MRCP - ERCP if ultrasound is positive |
|
|
How do you treat AIDS Cholangiopathy?
|
- Biliary sphincterotomy (cutting the biliary sphincter during ERCP)
- Stenting of dominant extra-hepatic strictures - Anti-microbial treatment NOT effective - Ursodeoxycholic acid may be helpful in small series |
|
|
What parasites can infect the biliary tree?
|
- Ascaris lumbricoides
- Echinococcus granulosus - Clonorchis sinensis (Chinese Liver Fluke) - Opistohorchiasis - Fasciola hepatica (Sheep Liver Fluke) |
|
|
What parasites can affect the biliary tree? Where are they found?
|
Ascaris lumbricoides
- Roundworm that is found world-wide - Adult worms inhabit human small intestine Echinococcus granulosus - Tapeworm found in S. America, Middle East, E. Mediterranean, some sub-Saharan countries, China, and former Soviet Union - Canines are hosts Clonorchis sinensis (Chinese Liver Fluke) - Far East and far eastern Russia - Dogs and cats are reservoirs Opistohorchiasis - Liver fluke in SE Asia and Central / Eastern Europe - Cats, dogs, and fish-eating mammals Fasciola hepatica (Sheep Liver Fluke) |
|
|
Which biliary parasites are:
- Roundworms? - Tapeworms? - Liver Flukes? |
- Roundworm: Ascaris lumbricoides
- Tapeworm: Echinococcus granulosus - Liver Fluke: Clonorchis sinensis (Chinese), Opisthorchiasis (cats, dogs), Fasciola hepatica (sheep) |
|
|
How do you treat the biliary parasites?
|
Ascaris lumbricoides:
- ERCP for removal - Anti-helminthic therapy Echinococcus granulosus: - Surgical resection - Percutaneous injection of scolicidal agents - Anti-helminthic therapy Clonorchis sinensis AND Opisthorchiasis AND Fasciola hepatica (all liver flukes): - Anti-helminthic therapy - ERCP for acute cholangitis |
|
|
Ascaris lumbricoides:
- Type - Location - Reservoir - Diagnosis - Treatment |
- Roundworm
- Worldwide - Inhabits human small intestine - Diagnose w/ US (long, linear, parallel echogenic structure w/o acoustic shadowing) or w/ ERCP - Treat by removing w/ ERCP or w/ anti-helminthic therapy |
|
|
Echinococcus granulosus:
- Type - Location - Reservoir - Symptoms - Treatment |
- Tapeworm
- S. America, Middle East, E. Mediterranean, some Sub-Saharan countries, China, former Soviet Union - Canines are hosts - Rupture of hepatic cyst into biliary system, jaundice and hepatomegaly - Treat by surgically resecting or percutaneous injection of scolicidal agents in addition to anti-helminthic therapy |
|
|
Clonorchis sinensis:
- Type - Location - Reservoir - Symptoms - Treatment |
- Chinese liver fluke
- Far East and far eastern Russia - Reservoirs are cats and dogs - Asymptomatic, cholangitis, chronic infection associated w/ cholangiocarcinoma - Treat w/ anti-helminthic therapy or ERCP for acute cholangitis |
|
|
Opisthorchiasis:
- Type - Location - Reservoir - Symptoms - Treatment |
- Liver fluke
- SE Asia and C/E Europe - Found in cats, dogs, and fish-eating mammals - Asymptomatic, cholangitis, chronic infection associated w/ cholangiocarcinoma - Treat w/ anti-helminthic therapy or ERCP for acute cholangitis |
|
|
Fasciola hepatica:
- Type - Cause - Reservoir - Symptoms - Treatment |
- Sheep liver fluke
- Eating raw vegetables infected w/ metacercariae - Human infection - Penetrates duodenal wall, migrates across peritoneum, and enters biliary system - Treat w/ anti-helminthic therapy and ERCP for acute cholangitis |
|
|
Which biliary disease is found almost exclusively in patients from SE Asia?
|
Recurrent Pyogenic Cholangitis
|
|
|
What causes Recurrent Pyogenic Cholangitis?
|
- Pigment stone formation in intra-hepatic biliary system
- Results in intra-hepatic stricturing and biliary obstruction - Leads to recurrent bouts of acute cholangitis |
|
|
Which patients are affected by Recurrent Pyogenic Cholangitis?
|
Almost exclusively in patients from SE Asia
|
|
|
What are the clinical manifestations of Recurrent Pyogenic Cholangitis?
|
Acute cholangitis
- Infection of the bile duct (cholangitis) - Usually caused by bacteria ascending from its junction with the duodenum - It tends to occur if the bile duct is already partially obstructed by gallstones |
|
|
How do you diagnose Recurrent Pyogenic Cholangitis?
|
- Abdominal US
- MRI - CT - PTC - ERCP |
|
|
How do you treat Recurrent Pyogenic Cholangitis?
|
- Treat acute cholangitis (antibiotics and biliary drainage)
- Stone clearance (ERCP, PTC, surgical) - Consider Ursodeoxycholic acid (limited data) - Hepatic resection and reanastomosis |
|
|
What are the potential complications of Recurrent Pyogenic Cholangitis?
|
- Cirrhosis from secondary sclerosing cholangitis
- Increased risk for cholangiocarcinoma |
|
|
What is the term for gallstones?
|
Cholelithiasis
|
|
|
What are the symptoms of Cholelithiasis?
|
- Often asymptomatic (up to 90%)
- Approximately 20% will become symptomatic - Higher likelihood of continued symptoms or complications (eg, pancreatitis or cholecystitis) w/ symptomatic gallstones |
|
|
What does the term Cholelithiasis indicate?
|
Gallstones or sludge in the gallbladder
|
|
|
What are the potential complications of Cholelithiasis?
|
- Pancreatitis
- Cholecystitis |
|
|
What are the risk factors for Cholelithiasis?
|
- Pregnancy and estrogen and oral contraceptives
- Terminal ileal resection - Gallbladder stasis (DM, total parenteral nutrition) - Reduced physical activity (men) - Age (increased risk w/ age) - Gender (females) - Ethnicity (50-75% prevalence of cholesterol gallstones in Pima Indians and certain other Native Americans) - Obesity - Rapid weight loss - Cirrhosis - Hemolytic anemias - Hypertriglyceridemia |
|
|
What is the term for intermittent cystic duct obstruction? Symptoms?
|
Biliary Colic:
- Crescendo steady pain in RUQ that can radiate to back and right shoulder - Nausea - After ingestion of fatty foods - Lasts < 4 hours before abating completely |
|
|
What causes biliary colic?
|
- Intermittent cystic duct obstruction
- Brought on after ingestion of fatty foods |
|
|
How long does Biliary Colic last?
|
Less than 4 hours at a time before abating completely
|
|
|
How do you diagnose Cholelithiasis? Sensitivity / specificity?
|
- Transabdominal US: sensitivity 84% and specificity 99%
- Endoscopic US: sensitivity 96% and specificity 86% |
|
|
Which method of diagnosing Cholelithiasis is more sensitive? Specific?
|
- Sensitive: Endoscopic Ultrasound
- Specific: Transabdominal Ultrasound |
|
|
How do you treat asymptomatic Cholelithiasis?
|
Prophylactic cholecystectomy ONLY for patients with risk factors
|
|
|
What makes a cholecystectomy for asymptomatic Cholelithiasis indicated?
|
- Biliary cysts
- Caroli's disease - APBJ - Gallbladder adenomas - Porcelain gallbladder - Patients w/ Sickle Cell Disease, hereditary spherocytosis, or undergoing gastric bypass surgery |
|
|
How do you treat a patient with Cholelithiasis and Biliary Cholic?
|
- Cholecystectomy
- Non-surgical: Ursodeoxycholic acid, extracorporeal shockwave lithotripsy |
|
|
What is the term for gallstones or sludge in the common bile duct?
|
Choledocholithiasis
|
|
|
What is Choledocholithiasis?
|
Stones or sludge in the common bile duct
|
|
|
What causes most Choledocholithiasis?
|
- Mostly secondary to passage of Cholelithiasis
- Primary is less common (eg, cystic fibrosis, periampullary diverticulum large bile ducts) |
|
|
What are the clinical manifestations of Choledocholithiasis?
|
- Asymptomatic
- Intermittent RUQ pain (more prolonged than biliary cholic and resolves w/ stone passage, removal, or ball-valve effect (does not obstruct opening) - Nausea / vomiting - Elevated liver tests typically in cholestatic patient |
|
|
How do you diagnose Choledocholithiasis?
|
* Endoscopic US: 94% sensitivity and 95% specificity
- Abdominal US has poor sensitivity (38-42%) b/c overlying bowel gas, negative study does not exclude - Cholangiography: ERCP, MRCP, intra-operative |
|
|
How do you treat Choledocholithiasis?
|
- ERCP
- Intra-operative bile duct exploration |
|
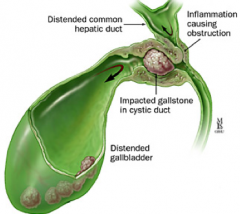
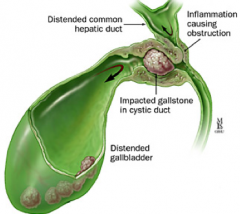
|
What is the syndrome that causes common hepatic duct obstruction from extrinsic compression by an impacted stone in the cystic duct or Hartmann's pouch of the gallbladder?
|
Mirizzi Syndrome
|
|
|
What are the features of Mirizzi Syndrome?
|
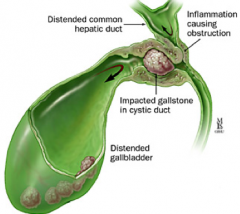
- Common hepatic duct obstruction from extrinsic compression
- May be by an impacted stone in the cystic duct or Hartmann's pouch of the gallbladder |
|
|
What are the clinical manifestations of Mirizzi Syndrome?
|
- Jaundice
- RUQ pain - Fever - Elevated liver tests in cholestatic pattern |
|
|
What is Mirizzi Syndrome associated with?
|
Gallbladder cancer
|
|
How do you diagnose Mirizzi Syndrome?
|
- Abdominal US
- Cholangiography (ERCP > PTC, MRCP) |
|
How do you treat Mirizzi Syndrome?
|
- Surgery: cholecystectomy ± bilioenteric anastomsis
- Endoscopic: limited role |