![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
72 Cards in this Set
- Front
- Back
|
What is Personality? |
-Lets us distinguish people from each other -Behavior that is caused by internal factors, not environmental -Behaviors that fit together in a meaningful fashion |
|
|
Psychodynamic Perspective of Personality |
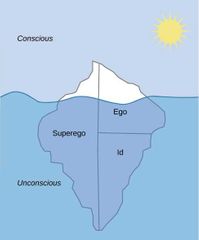
-Personality is an energy system -Psychic energy: generated by instinctual drives pressing for release -Id: Present at birth. Unconscious. Functions irrationally. Basic urges like eat, sleep, sex. Follows Pleasure Principal, maximize pleasure and minimize pain. -Ego: Second to develop. Reality Principal, tests reality to decide when Id can safely be disharged. Controls Id. Balances Superego and Id. -Superego: Last to develop. Ideals internalized from parents and society. Controls ego with pride and guilt |
|
|
3 sources of anxiety in psychodynamic perspective |
-Reality anxity: Fear of real world threats -Neurotic anxiety: Fear of id's desires -Moral Anxiety: Fear of superego's guilt |
|
|
Defense Mechanisms |
Deny or distort reality to deal with anxiety -Repression: Pushed to subconscious -Denial -Sublimation: Released in a socially acceptable manner -Projection: Attributing impulse to other people -Regression: Mentally returning to an earlier safer state -Intellectualization: Situation treated as intellectually interesting event -Reaction formation: Exaggerated opposite behavior -Conversion: Conflict converted into physical symptom -Displacement: Use a secondary goal as an outlet (getting angry at something else) -Rationalization: "Hitting my kids for their good" -Isolation: Memories allowed back into consciousness but without motives or emotion |
|
|
Tapping into the unconsciousness |
-Dreams: Not constrained by reality (ego) and morality (superego). But anxiety can still be around in dreams. Have surface and deep meaning -Free Association: Freud opts for this hypnosis. Patient is to say anything, no matter how trivial, embarrasing or unrelated. Analyst looks for associations and resistance. -Errors of speech and memory: Freudian slips. Absent-mindedness |
|
|
Evidence for and Against Freud |
For: - Subconscious processing: Semantic priming effect - Repression: Memory lapses during therapy Against: - Dreams: People do not necessarily dream about desires. - Anthropological evidence: Oedipus complex is not culturally universal |
|
|
Neoanalysts |
-Disagreed with certain aspects of freud's thinking
-Object relations: Focuses on mental representations people form of themselves and others early in life. Early attatchment has a big impact on later life |
|
|
Humanistic Perspective of personality |
Carl Rogers' Self Theory: Behavior is a response immediate conscious experience of self and environment. -Self: organized consistant perceptions and beliefs about oneself. -Congruence: Consistancy between self-perception and experience. -Need for positive regard: acceptance, Sympathy. (similar to superego).
-Conditions of worth: dictate when we approve of ourselves (simolar to superego). -Self verification: Need to preserbe self concept by maintaining self-consistancy and congruence. -Self Enhancement: Need to regard themselves positively. -Self Esteem: How positively or negatively we feel about ourselves. *Negatives: relies too much on individual reports of experiences
|
|
|
Biological Perspective of personality |
-Cattell's sixteen Personality factors: Found 16 basic behavior clusters. -Eysenck: 3 basic traits. Introversion-Extroversion. Stability-instability. Psychoticism-self control. -Five factor model: 5 universal factors~ Openness, conscientiousness, extraversion, agreeableness, neuroticism (OCEAN). -Introverts are chronocally over aroused. Extroverts were chronically under aroused - Stability of personalities: Introversion/extroversion, optimism/pessimism, activity level, seem to be stable. Self monitoring~ ones tendency to tailor behavior to a situation. |
|
|
Social cognitive theorists on personality |
- Focus on both internal and external causes of personality -Reciprocal determinism: person, behavior, and environment all influence each other * these Theories have strong scientific base |
|
|
Rotter |
Whether we will do something depends on: -Expectancy: What we expecr the behavior to cause -Reinforcement value: How much we desire/dread the expected outcome -Internal/external locus of control: Called a generalized expectancy. (Internalized people think life is under our control. Externalized people think their fate is determined by luck, chance, etc.) *Internalized people do better in school, are independent, cooperative, resistant to social influence, healthier |
|
|
Bandura |
• Human agency - humans are active agents in their own lives, we are self-reflective and self-regulatory Four processes • Intentionality - we plan, modify plans, act with intention • Forethought - we anticipate outcomes, set goals, activelychoose behaviors • Self-reactiveness - motivating and regulating our own actions • Self-reflectiveness - evaluate our own actions |
|
|
Mischel |
• We need to consider individual ways of perceiving and understanding events • Consistency paradox - we expect and perceive high consistency of personality, but inreality it varies greatly with situations • Cognitive-affective personality system - both the person and the situation matter |
|
|
Personality Assessments |
Interviews • Structured interviews - standardized situation • Must look at more than what they’re saying:appearance, speech patterns, posture Personality Scales • Objective: standard set of questions • Easy to score. *People can lie however Projective Tests • Psychodynamic theorists say we can’t use interviews/questions becausethe things we want to know are unconscious • e.g. Rorschach inkblots, Thematic Apperception Test. What you see or feel tells what your personality is *• Psychodynamic theorists prefer projective tests, Humanists prefer self-report |
|
|
Stressors |
Negative life changes -Microstressors: daily hassles and annoyances. -Catastrophic events: natural disasters, war. -Major negative events: victim of major crime/abuse, loss of loved one, academic failure. |
|
|
Stress Response |
4 aspects of Appraisal 1. Primary appraisal of the demand the situation. 2. Secondary appraisal of resources available to cope with it. 3. Judgements of what the consequences could be if you fail. 4. Appraisal of the personal meaning - what outcome might imply to us.
|
|
|
General Adaptation Syndrome (GAS) |
Physiological response pattern to strong & prolonged stressors *good figure in textbook* 1. Alarm Reaction •Rapid increase in physiological arousal • “Fight or flight” response • Adrenal medulla produces epinephrine 2. Resistance -Body is resisting the parasympatheticnervous system that istrying to calm it down as it continues to fight the stressor. Exhaustion -After the stressor, there is an increased vulnerability to disease (or even death). This is why you get sick after exams.
|
|
|
Anxiety |
• Subjective distress • Physiological activation • Avoidance/escape behavior towards theperceived cause • Interference/restriction in daily routine,occupational or social functioning |
|
|
PTSD |
• Caused by specific event: torture, rape, accident, war • Onset immediate or months later • Severe anxiety, physiological arousal and distress • Painful, uncontrollable reliving of the event in flashbacks, dreams and fantasies • Emotional numbing and avoidance of stimuli associated with the trauma |
|
|
Stress and Illness |
• Stress increases risk of heart attack, cancer and death after death of a loved one • Also increases arthritis, rheumatism, bronchitis, ulcers, earth disease, asthma, migraines • Stress reduces fat metabolism, increasing artery blockage • Reduces immune system • Makes people more likely to behave unhealthily (e.g. diabetics don’t take medication) |
|
|
Protecting against stress |
Social Support • Ability to rely on and talk to others • People without social support are more likely to die earlier • Talking about a traumatic event in a study makes you less likely to visit the campus hospital later in the year • Makes immune system stronger Physiological toughness A relationship between two classes of hormones secreted by adrenalglands in response to stress. • Catecholamines - epinephrine and NE (boosts immune system) • Corticosteroids - mainly cortisol (damages it)
People with high physiological toughness respond to stress with low levels of cortisol and quick strong jump in catecholamines. |
|
|
Type A vs Type B personalities |
• Type A - live under great pressure, demanding of themselves and others. • Type B - more relaxed and agreeable, far less time urgency. |
|
|
Cognitive protective Factors |
Hardiness Three parts trait: 1. Commitment to work/family 2. Perception of control over situation (biggest factor) 3. Viewing the situation as a challenge Optimism - Optimism makes you healthier, increases immune system Coping self-efficacy -The conviction that we can copesuccessfully Finding meaning instressful life events -Religion can increase or decrease stress |
|
|
Problem focused vs emotional focused Coping |
-Problem-focused coping: Confront & deal directly with demands of stressor -Emotion-focused coping: Manage the emotional response (much worse thanproblem-focused)
*Seeking social support: Turning to others for assistance during times of stress -seeking social support, and problem focused coping are usually more healthy |
|
|
Transtheoretical Model Of Behavior Modification |
6 stages: -Pre-contemplation: problem unrecognized -Contemplation: problem recognized -Preparation: Preparing to change behavior -Action: implementing change strategy -Maintenance: behavior change maintained -Termination: permanent change; no maintenance required *Can take several cycles. Usually 3-5 for smokers. |
|
|
Bandura’s social cognitive theory |
People learn from those they admire • Produce highly engaging “entertainment-education” radio dramas to increaseawareness and counteract false beliefs • Positive role models with positive consequences • Negative role models with negative ones • Transitional models who start out bad and get better |
|
|
SUBSTANCE ABUSE TREATMENT/PREVENTION: Motivational Interviewing |
Leads people to their own conclusions by asking questions, revealing their discrepancies between self and ideal-self. |
|
|
SUBSTANCE ABUSE TREATMENT/PREVENTION: Harm Reduction Approaches |
• Designed not to eliminate a behavior, butrather to reduce the harmful effects of abehavior when it occurs •E.g. Safe needle clinics, methadone for heroinaddicts |
|
|
SUBSTANCE ABUSE TREATMENT/PREVENTION: Relapse Prevention |
• Dropout rates are a big problem for substance abusetreatment • Relapses are caused by lapses - one time slips due toa high stress situation • Not enough self-efficacy to resist temptation |
|
|
What is Abnormal? |
Something that causes (3D's): -Distress: to self or others -Dysfunction: for person or society -Deviance: violate social norms Abnormal behavior -Personally distressing, dysfunctional and/or so culturally deviant so that other people judge it to be inappropriate or maladaptive. |
|
|
Major psychological disorder Categories |
Anxiety disorders: intense,frequent, inappropriate anxiety but no loss of contact with reality (phobias, panic, OCD, PTSD) Mood (affective) disorders -marked disturbances in mood(depression, mania) Dissociative disorders -problems of consciousness or self-identification (amnesia, multiplepersonalities Schizophrenic and otherpsychotic disorders - disorders ofthinking, perception and emotion -loss of contact with reality Somatoform disorders - physicalsymptoms such as blindness,paralysis or pain with no physicalbasis Substance abuse disorders -personal and social problems withpsychoactive substances Sexual and gender identitydisorders - sexual dysfunctions,deviant sexual behaviors(molestation, fetishes), Eating disorders - anorexia andbulimia Personality disorders - rigid,stable and maladaptive personalitypatterns (antisocial, dependent,paranoid, narcissistic) |
|
|
Until Mid 70’s, Psychological disorders were either: |
Neurosis - anxiety, suchas a phobia (still in touchwith reality) Psychosis - thought disturbance,such as schizophrenia (lost touchwith reality) |
|
|
Anxiety Disorders |
-Frequency and intensity of anxiety responses are out of proportions to the situations that trigger them Characteristics • Subjective-emotional distress • Avoidance-escape behavior • Interference in daily routine and socialfunctioning • Onset in young adulthood. • Most prevalent psychological disorderin North American • More common in females • High occurrence: affects 25% of people |
|
|
Phobia |
- strong and irrational fears of certain objects or situations • They realize they are irrational but can’t help it |
|
|
Generaized anxiety Disorder |
- chronic “free-floating” anxiety that is not attached to specific situations or objects |
|
|
OCD |
• Obsessions - repetitive and unwelcome thoughts, images, orimpulses (cognitive) • Compulsions - repetitive behavioral responses, like cleaningrituals (behavioral) • Doing the compulsions prevents great anxiety and panic attacks • Patients know the compulsions don’t make sense, and wish theycould stop • Occurs in 2% of men and women |
|
|
Causes of anxiety Disorderes |
Biological Factors • 40% concordance rates for identical twin, only 4% for fraternal twins. • Genetics and Oversensitive autonomic nervous system lead to symptoms. Psychodynamic View - unacceptable impulses threaten to overwhelm the ego's defenses Learned Response (Behavioral View) • Classical conditioning - develop phobia after being bitten by snake • Observational learning - develop fear from watching TV Sociocultural - some anxiety disorders are culture specific • E.g. Koro: Southeast Asian fear that your penis will retract into stomach and kill you -People |
|
|
Eating Disorders |
Anorexia Nervosa • Intense fear of being fat • 90% female • View themselves as fat despite being tiny • Bone loss, heart strain, stops menstruation Bulimia Nervosa • Vomiting, laxatives to avoid gaining weight • Consume thousands of calories during binges • Normal body weight but gastric problems, teeth erosion |
|
|
Mood Disorders |
• Disturbance in mood (known as affect) rather than in thought • Emotional highs are called “manias”, and lows are called “depression” Bipolar Disorder • Bipolar disorder is depression with periods of mania • About 10 episodes of each state during the course of the patient’s life |
|
|
Somatoform Disorders |
• Complaints of physical symptoms that are not physiologically possible. • Differ from psychophysiological disorders - psychological factors cause or contribute to a real medical condition (ulcer, asthma, blood pressure) Conversion disorder: serious neurological symptoms(blindness, paralysis, sensation loss) suddenly occur Hypochondriasis: beingalarmed about any physicalsymptom, convinced they haveserious illness |
|
|
Dissociative Disorders |
Dissociative Identity Disorder (DID) • Used to be called “multiple personality” • Two or more separate personalities coexist in the same person •Trauma-Dissociation Theory: new personalities occur in response to severestress, usually in childhood about physical/sexual abuse Psychogenic Amnesia: Person responds to a stressful event with extensive but selective memory loss.
Dissociative fugue: Lose sense of identity, give up on life, wander |
|
|
Schizophrenia |
-Detatchment from the world • Severe disturbances in thinking, speech, perception,emotion and behavior • Schizophrenia means split-mind, but it is not same as (DID). • The components of the mind (thoughts, speech,perception, emotion) become disconnected. Types: •Type-I Positive symptoms: delusions, hallucinations, disordered speech/thoughts. •Type-II Negative symptoms: lack of emotion, loss of motivation, absence of normal speech. |
|
|
Personality Disorders |
Antisocial: irresponsibleand antisocial, impulsiveneeds, lack of empathy,highly manipulative, no conscienceHistrionic: dramatic,attention seeking,promiscuous, highlyimpressionable, out of touchwith negative feelings Narcissistic: grandiosefantasies, lack ofempathy, need foradmiration from others,proud self-display Borderline: severe instabilityof self- image, relationships,emotions. Extreme love andhate of same person.Manipulative and suicidal. Avoidant: extremesocial discomfort, fearof being negativelyevaluated Dependent: extremesubmissive anddependent behavior,fear of separation Obsessive-compulsive: perfectionism,orderliness,inflexibility Schizoid: indifferent to socialrelationships, restricted rangeof emotions Schizotypal: odd thoughts,appearance, behavior.Discomfort in social situations. Paranoid: unwarrantedtendency to interpretbehavior as threatening |
|
|
Childhood Disorders |
ADHD • 7-10% of children, most commonchildhood disorder • More likely in boys • Boys act aggressive, girls act inattentive Autistic Disorder • Extreme unresponsiveness to others • Poor communication • Repetitive and rigid behavior patterns |
|
|
Psychotherapy |
• 200 different forms • Therapy through psychological techniques, not drugs • Most therapists are eclectic therapists - use all different kinds of therapies • “Psychologist” is a protected term. To call yourself one you must be licensed. Usually have PhD or Masters. • Therapist, counselor, psychotherapist and hypnotist are not protected terms,so anyone can call themselves these. |
|
|
Psychoanalysis |
• Goal: achieve insight: conscious awareness of underlying problems. Therapist interprets: Free association: sit behind client and tell them to say anything. Dream interpretation: the “royal road to unconscious”. Resistance: defensive mechanism against therapy, sign of a sensitive topic. • Patient becomes angry, avoids topic, misses appointments. • Analyzed to promote insight and prevent therapy dropping. Transference: client responds irrationally to the analyst as if they were animportant figure from client’s past. • Can be positive (love, dependency) or negative (hate, anger). • Very important part of therapy Interpretation: provide client with insight into their behavior • Interpretations should be near the surface of awareness • Deep interpretations are bad, cannot be informative •Client must eventually arrive at the insight themselves |
|
|
Humanistic Therapy |
• Focus on future and present, rather than past. • We need to find out what is preventing you from realizing full potential. Client-Centered Therapy (AKA Person-Centered): • Relationship develops between client and therapist to foster self-exploration. Therapist has an unconditional positive regard, and has to be geuniune. Gestalt Therapy: • Patient is ignoring the background - important feelings, wishes thoughts that are blocked • Bring them into awareness, get in touch with inner self • Often done in groups • Much more confrontational than client-centered therapy |
|
|
Cognitive Therapy |
• Concerned with present rather than past • Very directive, tell you exactly what is wrong and what to do about it. Ellis' Rational-Emotive Therapy: - A (activating ebent triggers emotion) -B (Belief system that appraises the event) -C ( consequences of appraisal) -D (Disputing erroneous belief system) |
|
|
Classical Conditioning Treatments |
Exposure: assumes phobias are learned • Flooding (Lots of Exposure) to disassociate the CS with the UCS Aversion Therapy: pair an unwanted behavior (drinking, pedophilia) with a bad USC (nausea, shock)
|
|
|
Operant Conditioning Treatments |
• Use positive/negative reinforcement or punishment. (E.g. token economy) • Works well for schizophrenics, disturbed children, mental retardation |
|
|
Mindfulness Based treatments |
• Mindfulness is mental state of awareness, focus, openness and acceptive of experience • Learn a meditation technique to focus on your sensations, thoughts and feelings andovercome them without struggle • Used for stress, depression, drug relapse prevention |
|
|
Dodo bird verdict |
All therapies appear to be equally effective |
|
|
Drug Therapies |
Anti-Anxiety Drugs: reduce anxiety withoutdisturbing alertness • Tranquilizers, Xanax, Valium • Prone to dependency Anti-Mania Drugs • Lithium Carbonate • For bipolar disorder: eliminate manicphase and depression does not return • Correct dosage is critical Antidepressant Drugs • Relapse is more likely for drugs alone than drugs with therapy Typea of drugs: -Trycyclics: prevent reuptake -MAO inhibitors: reduce breakdown -SSRIs: prevent reuptake
|
|
|
Electroconvulsive Therapy |
• Someone noticed that schizophrenia and epilepsy never happen together. Came up with the crazy idea of inducing seizures to treat schizophrenia. • Less than 1 second electrical current is applied to the head *Turns out its not useful for anxiety disorders, or schizophrenia. Can be used for severe depressionor suicidal patients. |
|
|
Psychosurgery |
• Remove brain tissue to change disordered behavior, inabsence of obvious organic damage • Used to be done very often, but stopped due to safetyconcerns and increased availability of drugs Cingulotomy: still done today, surgeon cuts abundle near the corpus callosum (cingulum bundle) • Treats depression and OCD |
|
|
Situation vs Competancy Focussed Prevention |
Situation focussed prevention: reduce environmentalcauses of disorders and enhance the factors that prevent them • Reduce unemployment, discrimination, poverty Competency focussed prevention: increase personalresources and coping skills • Increase stress resistance, social and vocationalcompetencies, self esteem |
|
|
Neoanalysts: Adler |
-Adler: Humans are motivated by social interest. Humans strive for superiority, compensating for imagined defects. |
|
|
Neoanalysts: Jung |
-Jung: Humans have a personal and collective unconscious. Memories are represented by archetypes (inherited tendencies to interpret experiences a certain way) |
|
|
Stress on health |
Death, divorce, etc is correlated with lowered psychological well being |
|
|
Vulnerability vs protective factors |
-Vulnerability factors: increases peoples susceptability to stressful life events -Protective factors: environmental or personal resources that help people cope more effectively with stressful events. |
|
|
Health psychology |
Stress plays a role in 50-70% of all physical illness |
|
|
SUBSTANCE ABUSE TREATMENT/PREVENTION: Multimodal treatment |
-Aversion therapy -Relaxation -Self-monitoring |
|
|
Positive psychology |
The study of happiness, well being, etc |
|
|
What is the DSM |
Diagnostic and statistical manual -Defines a mental disorder as a clinically significant behavior or psychological syndrome that is associated with distress. |
|
|
Panic disorder |
Occur suddenly and unpredictably without stimulus, and are much more intense. Symptoms can be intense and terrifying |
|
|
Basic goal of all treatment |
To change maladaptive, self-defeating thoughts, feelings and behavioral patterns Map on pg 683 |
|
|
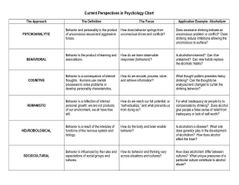
Different perspective of Behavior SUMMARIZED |
|
|
|
Freuds view of human mind |
|
|
|
Freuds 5 psychosexual stages |

|
|
|
Diagnosing Psychological Disorders |
Multiaxial approach - 1. Clinical disorders 2. Personality disorders 3. General Medical Conditions 4. Psychosocial and environmental problems 5. Level of current functioning DSM-IV VS DSM-V -DSM-IV is categorial. You either fit the criterion or not. Uses multiaxial. -DSM-IV is dimensional. Relevant behaviors are measured on a continuum. Disorders differ in severity, rather than kind. |
|
|
Psychotherapy Approaches SUMMARIZED |

|
|
|
Aphasia, apraxia, agnosia |
Memory impairments: -Aphasia: Language comprehension -Apraxia: Motor (speech production) -Agnosia: Recognition |