![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
What are diuretics? |
Drugs that increase the rate of urine flow by acting on the kidney and producing a net loss of Na+ and water |
|
|
What do Diuretic drugs do? |
Increase excretion of Na and water
Decrease Na reabsorption and accompanying anions Primary effect - natriuresis Secondary - increased water loss |
|
|
Two ways in which diuresis is achieved? |
Direct action on cells of nephron Indirectly modifying filtrate content |
|
|
How much Na is excreted per day? |
150 mmol/day in western diet
Can range from 10-400 mmol/day |
|
|
What are the four basic classes of diuretics? |
Osmotic
Loop Thiazide K+ sparing |
|
|
Describe the kinetics of an indirect diuretic? How is it administered? |
Proximal convoluted tubule osmotic diuretics - freely permeable to water
Mannitol t1/2 = 100 minrenal excretion 90% IV |
|
|
What is the action of mannitol and other effects? |
Freely filtered but cannot be reabsorbed
Cannot cross BBB, draws ECF into plasma Rescues brain volume May prevent herniation |
|
|
Why is water reabsorption reduced in mannitol?
|
The increase in urine flow rate decreases the contact time between fluid and the tubular epithelium, thus reducing sodium as well as water reabsorption. |
|
|
What are the effects of mannitol? |
Osmotic diuresis
Increases osmolarity of blood and renal filtrate. Expands ECF and plasma volume - increases blood flow to kidney. Washes out the cortical medullary gradient - stops loH concentrating urine. Does not affect Na. Other uses: Reduced intracranial pressure (ICP) |
|
|
Name a loop diuretic Where does it act? |
Furosemide
Thick ascending limb |
|
|
What is the mechanism of the loop diuretic?
What is it used for? |
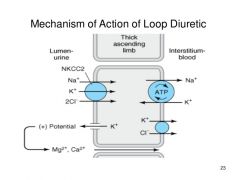
Inhibit Na+/K+/Cl- co-transporter to inhibit Na, K, Cl reabsorption by competing for Cl- binding site Inhibit Ma, Ca reabsorption in ascending limb - as dependent on positive lumen voltage grad. set up by K Reduces hypertonicity of the medulla - less of an osmotic drive to leave collecting duct so reduces water reabsorption in the collection duct system Secondary effect, increase PG production, vasodilation and increased blood supply to kidneys Antihypertensive: reduce plasma volume and produce arteriolar vasodilatation Edema due to congestive heart failure |
|
|
Diagram of Ascending Loop diuretics |
|
|
|
Give an example of a Thiazides diuretic Where does it act? |
Chlorothiazide Distal convoluted tubule |
|
|
What are the kinetics of Bendroflumethiazide? |
t1/2 = 3-4h Bioavailability 100% Protein binding 96% 70% metabolised in liver to active metaboliteEffects within 90 min, lasting 12-24h |
|
|
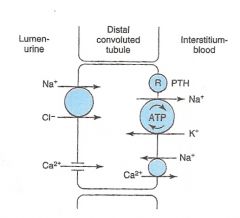
What is the mechanism of Bendroflumethiazide? |
Inhibit Na+/Cl- co-transport in the luminal membrane of tubule cells in the early segment of DCT Increases NaCl excretion - hence water excretion Increased Na+ reaching DCT stimulated an exchange with K+ and H+, with loss of these ions Secondary: Increase Ca reabsorption in distal tubule. Lower Na conc increases Na/Ca antiporter on basolateral membrane. Decreases intracellular Ca so more reabsorped via apical side of lumen |
|
|
Potential side effects of thiazides ? What is it used to treat |
hypokalaemia/alkylosis - reduced K levels Gout: increases reabsorption of urea in PTC , increases plasma uric acid levels, Treats hypertension and edema Pass into breast milk and decrease flow of breast milk |
|
|
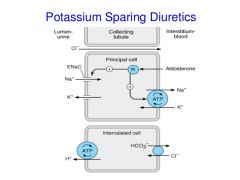
Name a K-sparing diuretic Where does it act? How does it work? |
Amiloride Distal convoluted tubule Blocks Na+/K+ exchange, decreasing K+ excretion Or, compete with aldosterone for intracellular receptor sites - prevents protein of proteins synthesised in reaction to aldosterone so no stimulation of Na/K exchange sites in collecting duct, preventing Na reabsorption, K and H+ secretion. |
|
|
What can K-sparing diuretics be combined with to reduce K loss? |
Sulphonamides (loop diuretics & thiazides) |
|
|
Is a small or large decrease in reabsorption required to cause a marked increase in Na+ excretion? |
Small as large proportion of NaCl and water that passes into the tubule via the glomerulus is reabsorbed |
|
|
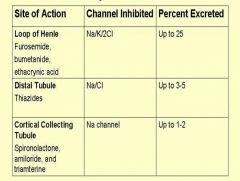
Draw a table to show the channels inhibited at different sites of action and the % excreted |
|
|
|
When are loop diuretics more effective than thiazides? |
Impaired kidney function |
|
|
When are K-sparing drugs used? |
in combination with other diuretics that would tend to lower K levels to potentially dangerous low levels (hypokalemia). |
|
|
How does the body eliminate loop diuretics? |
Secreted by PCT |
|
|
Diagram for thiazide mechanism |
|
|
|
Diagram for loop diurectics mechanism |
|
|
|
Diagram for K sparing diurectics mechanism |
|