![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
19 Cards in this Set
- Front
- Back
|
What are the two methods for tubular reabsorption? |
Transepithelial transport Passive reabsorption –down electrochemical or osmotic gradients Active reabsorption –against an electrochemical gradient (glucose, Na+) |
|
|
How is Na+ reabsorbed? |
Using an active Na+-Ka+ ATPase pump in basolateral membrane. Passive - Na+ symporter (proximal tubule), Na+ leak channel (collecting duct) Conc grad in lateral space so Na diffuses into interstitial fluid then peritubular capillary |
|
|
Percentage of energy of kidney spent on Na+ transport |
80% |
|
|
Where is Na reabsorbed? |
67 % proximal tubule
25 % l of H - conc. urine 8 % - distal and collecting tubules under hormal control. |
|
|
What is the function of aldosterone? |
Stimulates Na+ reabsorption in the distal and collecting tubules. (prox. is constant) In response to ANG II acting on adrenal cortex |
|
|
What are the two types of tubular cells in distal and collecting ducts? |
Intercalated and principle |
|
|
What is the function of RAAS? |
Na retaining, blood-pressure raising system
|
|
|
What do natiuretic peptide hormones do? |
Inhibit Na+ reabsorption, blood pressure- lowering system Promote natriuresis (excretion of Na) and accompanying diuresis, decreasing the plasma volume and directly influence the CVS to lower blood pressure |
|
|
Name the two NPHs |
Atrial natriuretic peptide (ANP) - Atrial cardiac muscle cells (more effective) Brain natriuretic peptide (BNP)- Ventricular cardiac muscle cells |
|
|
How do NPHs work? |
Directly inhibit Na+ reabsorption in the distal parts of the nephron Inhibit secretion of: Renin (kidney), aldosterone (adrenal cortex), vasopressin Increase GFR |
|
|
How do NPHs increase GFR? |
Vasodilate afferent arteriole] Vasoconstrict efferent arteriole Relax glomerular mesengial cells to increase Kf |
|
|
How are glucose and amino acids reabsorbed? |
Na+ -dependent secondary active transport in proximal tubule Symport carriers sodium and glucose cotransporter (SGLT) SGLT allows passive Na+ across luminal membrane and basolateral pump, pumps Na+ out into lateral space Pulls glucose through SGLT against concentration gradient (GLUT) |
|
|
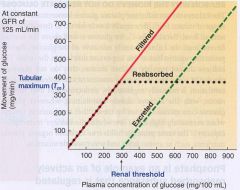
What is tubular maximum? |
Increase in conc. does not increase movement across membrane Tm - all SGLT are occupied Above Tm, appears in urine |
|
|
Why does Na+ not have Tm? |
Na+ carriers can be fully saturated in proximal tubule
BUT aldosterone promotes insertion of more Na+ -K+ carriers in distal and collecting tubules as required |
|
|
How to calculate filtered load of a substance? What is glucose's? |
plasma concentration x GFR of the substance Glucose - 100 mg/100 ml x 125 ml/min = 125 mg/min |
|
|
Tm for glucose? |
375mg/min |
|
|
Graph for Tm glucose |
|
|
|
Reason why the kidneys do not regulate glucose but do regulated phosphate and calcium |
Renal threshold of these ions equal their normal plasma concentrations |
|
|
What is active Na+ reabsorption also responsible for? |
Na+ actively reabsorbed. Water and urea follow by osmosis AQP-1 proximal tubule always open Hypertonicity in lateral space (water enters) AQP-2 distal part of nephron under vasopressin control |