![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
42 Cards in this Set
- Front
- Back
|
What is pharmacokinetics? |
the study of the movement of drugs into, within and out of the body. |
|
|
What is absorption? |
Passage of drug from its site of admin into plasma |
|
|
Name some absorption routes |
• Enteral (GI tract), oral, sublingual, rectal (diazepam) Cutaneous - poor absorption. |
|
|
What is the fastest route? |
inhalation - used for volatile and gaseous anaesthetics. Large Sa and blood flow. Bronchodilators |
|
|
What is the advantage of IV?
|
100% absorption and no loss of drug
|
|
|
What does ionisation affect? |
• Ionisation will affect ability to cross plasma membrane for absorption through epithelial cells into the circulatory system |
|
|
What is Bioavailability? |
proportion of drug dose which appears in the systemic circulation following admin. Oral admin – determined by stability in gut (gastric acid, flora), extent of absorption and extent of first-pass metabolism – fraction of drug lost to liver/gut. F = AUCoral/AUCIV. Does not account for rate of absorption - a drug completely absorbed in 30 min reach a much higher peak plasma conc. than if slowly |
|
|
Factors that affect bioavailability |
Variations in enzyme activity of gut wall or liver Gastric pH or intestinal motility. |
|
|
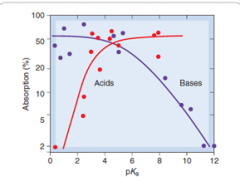
Graph for absorption of drugs from intestine, as a function of Pka for acids and bases |
|
|
|
• Absorption in intestine affected by? |
GI motility Splanchnic blood flow - increased by meal, reduced by hypovolaemia or heart failure particle size Physicochemical factors - |
|
|
What is Distribution? |
movement of drug around the body through membrane barriers |
|
|
What are compartments? |
ECF – blood plasma and interstitial fluid and lymph, ICF and TCF Heparin is confined to plasma - too molecular to cross capillary wall. |
|
|
What is • BBB? |
Continuous layer of endothelial cells joined by tight junctions and surrounded by pericytes. Inaccessible to many drugs with low lipid solubility. However, inflammation can disrupt integrity of BBB- pencillin given IV for bacterial meningitis. Active uptake system transport nutrients and metabolites. Lipophilic molecules pass through. Bypassed by injection into spinal canal. Bradykinin and enkephalins increase BBB permeability - treatment in brain tumours. |
|
|
What is • Volume of distribution (Vd? |
the volume of fluid required to contain the total amount, Q, of drug in the body at the same concentration as that present in the plasma V, Cp. Vd = Q/Cp. High value - extensive distribution to other compartments in the body (tissue binding) Must avoid IDing a given range of Vd too closely with a particular anatomical compartment. |
|
|
What does ionisation affect? |
distribution steady state distribution of drugs between aqueous compartments. pKa governs and pH of compartment governs the ration of ionised to unionised drug. |
|
|
Examples of drugs bound to plasma |
Albumin binds many acidic (warfarin) and some basic drugs (chlorpromazine) |
|
|
What does distribution depend on? |
• vascular permeability• regional blood flow• cardiac output and perfusion rate of tissue • ability of drug to bind tissue and plasma proteins• lipid solubility |
|
|
What is Metabolism? |
Enzyme- catalysed chemical modifications of drug molecules to inactivate and facilitate excretion |
|
|
Where does first pass metabolism occur? |
• Liver |
|
|
What is first pass metabolism? |
concentration of a drug is greatly reduced before it reaches the systemic circulation It is the fraction of drug lost during the process of absorption which is generally related to the liver and gut wall. Issues: marked individual variation occur in extent of FPM |
|
|
How do phases affect lipid solubility? |
decrease it - increasing renal elimination
|
|
|
What is phase I? |
catabolic (oxidation, reduction and hydrolysis). Oxidation mediated by cytochrome P450 enzymes (haem proteins) in liver carry out small-molecule drug metabolism. Paradoxically: sometimes more toxic or carcinogenic than parent drug Introduce a reactive group (-OH) – functionalisation. Serves as point of attack for conjugating system to attach a substituent e.g. glucuronide. Many hepatic enzymes embedded in SEM. Drug must cross plasma membrane - lipid-solbule so less so for polar. Often involve a monooxygenase system in which cytochrome P450 plays a key role. |
|
|
What is phase II?` |
Anabolic. Conjugation reactions – methyl/acetyl/sulphate. (acetyl CoA) Aspirin – attachment of glycine/glucuronic acid. Conjugate is pharmacologically inactive (usually), more water-soluble, and easily excreted. |
|
|
How does detoxification of paracetamol occur? |
• The tripeptide glutathione can conjugate drugs or their phase 1 metabolites via its sulfhydryl group |
|
|
Can metabolites be active? |
Yes,. pharmacologically active – sometimes more than parent drug |
|
|
How is aspirin metabolised? |
metabolised by the attachment of glycine or glucuronic acid |
|
|
Which enzyme metabolises ethanol? |
By a soluble cytoplasmic enzyme - alcohol dehydrogenase Not involved in P450 system |
|
|
What is Excretion? |
excretion of drug and/or metabolites |
|
|
Where does it occur? |
• Kidney, hepatobiliary system, lungs (volatile anaesthetics) and glandular secretions. Waste products of metabolism and other non-useful materials are eliminated from an organism. • Some drugs secreted into bile via the liver, but most are reabsorbed from intestine. |
|
|
Renal excretion: Filtration |
20k Da. If drug binds plasma albumin, only free drug is filtered. Warafin, 98% bound to albumin, conc. in filtrate is 2% of that in plasma – reduced clearance Heparin too large to cross. |
|
|
• Tubular secretion |
20% filtered, 80% pass to peritubular capillaries of pt. OAT transports acidic drugs while OCT handles organic bases. OAT carrier – against electrochemical gradient - can reduce plasma conc. to almost zero OCT – transport down ec gradient. Unlike filtration, carrier-mediated transport can achieve maximal drug clearance even when most of drug is bound to plasma. Penicillin – 80% protein bound – is almost completely removed by pt secretion.Diazepam - cleared extremely slowly Drugs compete for same transport system - drug interactions |
|
|
• Passive diffusion across tubular epithelium |
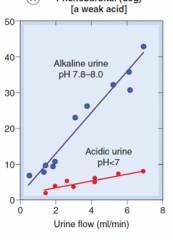
Volume of urine only 1% of filtrate. Lipid-soluble drugs are excreted poorly (as reabsorbed) whereas polar drugs of low tubular permeability remain in lumen. The ion-trapping effect –a basic drug is more rapidly excreted in an acid urine which favours the charged form and thus inhibits reabsorption (and vice versa). |
|
|
• Excretory products |
carbon dioxide, ammonia, urea, uric acid, guanine and creatine |
|
|
What is pH trapping? |
build-up of a higher concentration of a chemical across a cell membrane due to the pKa value of the chemical and difference of pH across the cell membrane. • Results in basic chemicals accumulating in acidic bodily fluids (cytosol) and acidic chemicals accumulating in basic fluids. |
|
|
pH trapping - energy requirement? |
• No energy required. |
|
|
Explain pH trapping further? |
• Cells are more acidic inside than outside so basic drugs are more charged inside cells. • Once non-changed molecule of basic chemical crosses membrane, ionised due to gaining H+ ion – unable to cross back. To maintain tm equilibrium, another unionised molecule enters cell. • Explains by basic drugs are secreted in acidic stomach (morphine) and acidic drugs excreted in urine (alkaline). |
|
|
What is half life? |
time taken for plasma concentration to fall to half its initial value. After single IV dose - Cp = C0e-Kelt, where C0 = initial plasma concentration and Kel = elimination rate constant; Kel = clearance / volume of distribution |
|
|
What causes variation between individuals? |
absorption, first-pass metabolism, Vd, clearance, effects of disease on pharmacokinetics, drug interactions |
|
|
Main routes by which drugs and their metabolites leave the body |
Kidneys - most drugs leave in urine, uncharged or as polar metabolites
Hepatobiliary system - some drugs are secreted in bile via liver. Most are reabsorbed from intestine. Lungs - occurs only with highly volatile or gaseous agents. |
|
|
Relevance of stereoselectivity |
Warfarin mixture of stereoisomers Differ in pharmacological effects and metabolism |
|
|
Clearance |
Volume of plasma containing the amount of substance that is removed from the body by kidneys in unit time Urine conc x urine flow rate/ plasma conc. Varies greatly - less than 1 ml/min to 700 ml/min - (renal plasma flow) |
|
|
Graph for effect of clearance of weak acid in alkaline and acidic urine |
|