Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
105 Cards in this Set
- Front
- Back
|
Is bilateral renal agenesis more common in males or females?
|
* Males - about 75% of the cases are males
|
|
|
What is more important for normal kidney development the ureter or the primitive kidney? When do these steps occur?
|
*Both
*Complete differentiation of the metanephric blastema into adult renal parenchyma requires the presence and orderly branching of a ureteral bud at the 5-7wk of gestation. *However it is theorized that induction of ureteral branching into major and minor calyces depends on the presence of a normal metanephric blastema |
|
|
In BRA are the ureters totally absent?
|
*Complete ureteral atresia occurs in about 50% of cases
|
|
|
What about the bladder, is it normally formed in these patients with BRA?
|
*No, The trigone, if developed, is poorly formed owing to failure of mesonephric duct structures to be incorporated into the base of the bladder.
*The bladder is small too and there are 2 theories behind that either the failure of urine production to initiate growth or that ureteral bud and wolffian duct structures migrating into the ventral cloacal region are needed to initiate bladder development |
|
|
What are typical findings on patients with BRA?
|
*low birth weight 1-2500grams
*IUGR *Oligohydramnios at birth *prominent fold of skin that begins over each eye, swings down in a semi-circle over the inner canthus and extends onto the cheek *Prematurily senile *nose is blunted and a prominent depression between the lower lip and chin is evident. *Low appearing ears w/ wide prominent flattened lobes *legs are often bowed and clubbed, with excessive flexion at the hip and knee joints. Occasionally, the lower extremities are completely fused as well (sirenomelia) |
|
|
What is the cause of the abnormal exam in children w/ BRA? Why do we think that?
|
*Oligohydramnios
*confirmed by an experiment in nature in which one twin with bilateral agenesis did not have the characteristic Potter facies because it shared the same amniotic sac, containing adequate amniotic fluid, with the second twin |
|
|
How long do children with BRA live?
|
*If not stillborn they would usually only live 24-48 hours.
*Longest in Campbell's is around a month. |
|
|
What are several different types of unilateral renal agenesis based on when the insult occurs?
|
*If the insult occurs before the 4th week (type I URA differentiation of the nephrogenic ridge with retardation of the mesonephric and müllerian components results, leading to complete unilateral agenesis of genitourinary structures. The individual has a solitary kidney and a unicornuate uterus.
*In type II anomalies, the defect occurs early in the 4th week of gestation, affecting both the mesonephric duct and the ureteral buds. The maldeveloped mesonephric duct prevents crossover of the müllerian duct and subsequent fusion. As a consequence, a didelphys (Uterus didelphys (sometimes also uterus didelphis) represents a uterine malformation where the uterus is present as a paired organ as the embryogenetic fusion of the mullerian ducts failed to occur. As a result there is a double uterus with two separate cervices, and often a double vagina as well. Each uterus has a single horn linked to the ipsilateral fallopian tube that faces its ovary.) uterus with obstruction of the ipsilateral horn and the vagina is produced. *If the insult occurs after the 4th week (type III), the mesonephric and müllerian ducts develop normally; only the ureteral bud and metanephric blastema are affected. Normal genital architecture is present despite the absence of one kidney. |
|
|
Are there usually associated genital abnormalities with URA in males?
|
*Regardless of the sex, both the ipsilaterally and contralaterally positioned testes are normal and the gonad is usually normal.
*In the male, the testis and globus major, which contains the efferent ductules and which arises from mesonephric tubules, are invariably present; all structures proximal to that point that develop from the mesonephric duct (the globus minor, vas deferens, seminal vesicle, ampulla, and ejaculatory duct) are frequently absent, with an incidence approaching 50% *What you might note on PE is that for men w/ unilateral absence of the vas deferens there may be absence of the ipsilateral kidney. |
|
|
Are there usually associated genital abnormalities with URA in females?
|
*Most common of these is a true unicornuate uterus with complete absence of the ipsilateral horn and fallopian tube or a bicornuate uterus with rudimentary development of the horn on the affected side.
*The fimbriated end of the fallopian tube, however, is usually fully formed and corresponds in its development to the globus major in the male *Partial or complete midline fusion of the müllerian ducts may result in a double (didelphys) or septate uterus with either a single or a duplicated cervix *Complete duplication or separation of the vagina, proximal vaginal atresia associated with a small introital dimple, and even complete absence of the vagina have been reported. *Obstruction of one side of a duplicated system is not uncommon, and unilateral hematocolpos or hydrocolpos associated with a pelvic mass and/or pain has been described in the pubertal girl |
|
|
What other conditions are associated with URA?
|
*septal and valvular cardiac defects; imperforate anus and anal or esophageal strictures or atresia; and vertebral or phalangeal abnormalities
*Many syndromes such as: Turner's syndrome, Poland's syndrome, Frazer's syndrome, BOR (brachio-oto-renal) syndrome, DiGeorge anomaly when associated with insulin-dependent diabetes mellitus in the mother, dysmorphogenesis, Kallmann's syndrome |
|
|
What is VACTERL & is it associated with URA?
|
*Twenty to 30 percent of children with the VACTERL association (vertebral, imperforate anus, cardiac, tracheo-esophageal atresia, renal, and limb anomalies) have URA
|
|
|
How is renal ectopia different from nephroptosis?
|
*differentiated from renal ptosis, in which the kidney initially is located in its proper place (and has normal vascularity) but moves downward in relation to body position
|
|
|
What urologic issues are associated with ectopic kidneys?
|
*enal pelvis is usually anterior (instead of medial) to the parenchyma because the kidney has incompletely rotated. As a result, 56% of ectopic kidneys have a hydronephrotic collecting system. Half of these cases result from obstruction at either the ureteropelvic or the ureterovesical junction (70% and 30%, respectively); 25% from reflux grade 3 or greater, and 25% from the malrotation alone
*vesicoureteral reflux has been found in 30% of children with ectopic kidneys |
|
|
Are there associated genital anomalies with renal ectopia?
|
*most striking feature is the association of genital anomalies in the patient with ectopia. The incidence varies from 15% to 45%
*Females - bicornuate or unicornuate uterus with atresia of one horn; rudimentary or absent uterus and proximal and/or distal vagina); and duplication of the vagina *Males - 0% to 20% have a recognizable associated genital defect; undescended testes, duplication of the urethra, and hypospadias are the most common |
|
|
Is cystoscopy in general helpful in diagnosing renal ectopia?
|
*Cystoscopy alone is rarely useful, because the trigone and ureteral orifices are invariably normal unless the ureteral orifice is also ectopic-a rare event
|
|
|
Is the thoracic kidney within the pleural space?
|
*No kidney is situated in the posterior mediastinum and usually has completed the normal rotation process (Fig. 113-10). The renal contour and collecting system are normal. The kidney usually lies in the posterolateral aspect of the diaphragm in the foramen of Bochdalek. The diaphragm at this point thins out, and a flimsy membrane surrounds the protruding portion of kidney. Therefore, the kidney is not within the pleural space. The lower lobe of the adjacent lung may be hypoplastic secondary to compression by the kidney mass. The renal vasculature and the ureter enter and exit from the pleural cavity through the foramen of Bochdalek.
|
|
|
Which is more common right to left or left to right ectopia?
|
*For renal ectopia it is left to right.
|
|
|
What is the most common type of crossed renal ectopia?
|
*Unilateral left to right crossed ectopia with the crossed kidney in the caudal position.
|
|
|
What is the sigmoid or S shaped kidney with crossed renal ectopia?
|
*second most common anomaly of fusion
*Fusion of the two kidneys occurs relatively late, after complete rotation on the vertical axis has taken place. Therefore, each renal pelvis is oriented correctly, and they face in opposite directions from one another. The lower convex border of one kidney is directly opposite the outer border of its counterpart, and there is an S-shaped appearance to the entire renal outline |
|
|
True or False the isthmus of the horseshoe kidney has its own blood supply?
|
*True
|
|
|
Are there associated abnormalities with the horseshoe kidney?
|
*Hypospadias and undescended testes each occurred in 4% of males, and a bicornuate uterus or septate vagina or both were noted in 7% of the females.
*Also other systems such as increased neural tube defects, etc. *More than 50% have VUR *Stone formation occurs commonly, but is not just due to delayed drainage, so metabolic testing should be considered. *UPJ obstruction causing significant hydronephrosis occurs in as many as one third of individuals |
|
|
What are other alternative treatments for calyceal diverticulum that have indications for treatment?
|
*ureteroscopic enlargement of the diverticular communication with removal of the stones
*extracorporeal laparoscopic stone removal with marsupialization of the diverticulum |
|
|
What is hydrocalycosis?
|
*Hydrocalycosis is a very rare cystic dilation of a major calyx with a demonstrable connection to the renal pelvis; it is lined by transitional epithelium.
|
|
|
What are possible causes for hydrocalycosis?
|
*It may be caused by a congenital or acquired intrinsic obstruction such as a parapelvic cyst
*Dilation of the upper calyx due to obstruction of the upper infundibulum by vessels or stenosis *Cicatrization of an infundibulum may result from infection or trauma *chalasia of a ring of muscle at the entrance of the infundibulum into the renal pelvis causes a functional obstruction |
|
|
Why might someone accidentally do a UPJ repair on a patient with megacalycosis?
|
*Sometimes calyces are dilated and usually increased in number, but the infundibuli and pelvis may not be enlarged. Although the UPJ does not appear obstructed, there may be segmental dilation of the distal third of the ureter or an ipsilateral segmental megaureter.
*Not infrequently this anatomic picture has been mistaken for congenital ureteropelvic or ureterovesical junction obstruction, with surgery being performed to correct the suspected defect. Postoperatively, the calyceal pattern remains unchanged. |
|
|
What are extrarenal calyces?
|
Extrarenal calyces are an uncommon congenital anomaly in which the major calyces as well as the renal pelvis are outside the parenchyma of the kidney
|
|
|
If someone has an upper tract tumor is it common to see an occurance on the other side at the same time or synchronously?
|
*No, extremely rare.
|
|
|
Who, as far as epidemiologic data, is more likely to develop upper tract TCC based on age, sex, and race?
|
Men are about twice as likely to develop upper tract tumors as are women ( Greenlee et al, 2000 ). In addition, whites are
about twice as likely as African Americans to develop upper tract tumors ( Greenlee et al, 2000 ). On the other hand, SEER data suggest that disease-specific annual mortality is greater in black men than in white men |
|
|
What is the risk of upper tract recurrence after bladder cancer?
|
On the basis of SEER data from the period 1973 to 1996, upper tract cancers developed in 657 of 91,245 cases of bladder cancer with adequate follow-up (4.1 years median) ( Rabbani et al, 2001 ). The relative risk for upper tract tumors for white
men and women was 64.2% and 75.4% at or before 2 years, 44.3% and 40.5% at 2 to 5 years, 50.8% and 42.1% at 5 to 10 years, and 43.2 and 22.2% at more than 10 years. |
|
|
How much do the kidneys contribute to the amniotic fluid & when? What about before that?
|
*Urine from the developing kidney is the major source of amniotic fluid, accounting for more than 90% of its volume by the third trimester
*skin, gastrointestinal tract, and central nervous system also contribute small amounts, particularly before urine production begins at 14 weeks. Therefore, the absence of kidneys reduces severely the amount of amniotic fluid produced during the latter stages of pregnancy. |
|
|
What are associated findings in female patients with BRA?
|
*Rare, but they get abnormal or no ovaries, abnormal or bicornuate uterus, abnormal or short vagina, or completely absent
|
|
|
What might be the first presenting sign of BRA?
|
*Well 40% are stillborn, if not identified w/ prenatal u/s which they would be, so it would prob. be a mother that had no prenatal care.
*If born alive you would note the PE fidings. *If for some reason you didn't know, just thought the kid was syndromic the first signs would be pulmonary. *If the child didn't urinate in the first 24 hours you would not be concerned, but after that you would evaluate. *Renal u/s shows no distention of bladder or no kidneys, no renal arteries then you have your dx. |
|
|
What if you suspect BRA and the renal ultrasound is inconclusive?
|
*Could do radionucleotide scan.
|
|
|
What is the most common cause of unilateral renal agenesis?
|
*These imaging studies have revealed that a substantial number of cases are caused by involution of a multicystic or dysplastic kidney before birth
|
|
|
Is unilateral renal agenesis like BRA in its male to female preponderance?
|
*NO, but still more common in males 2:1.
|
|
|
How might one diagnose URA on prenatal ultrasound?
|
*You may note the absence of one kidney
*If not you might notice the enlargement of the contralateral kidney suggetsing that it is working overtime |
|
|
If URA arises from involution of a multicystic dysplastic kidney should you worry about the normal kidney at all?
|
*There may be association with UPJ obstruction.
|
|
|
Is the supernumerary kidney usually the same size or smaller?
|
*Reniform shape but smaller
|
|
|
Can you have a normal appearance to the trigone while doing cystoscopy in a patient with a supernumerary kidney?
|
*Convergence of the ipsilateral ureters distally to form a common stem and a single ureteral orifice occurs in 50% of the cases.
*Two completely independent ureters, each with its own entrance into the bladder, are seen in the other 50% of cases |
|
|
Does a supernumerary kidney follow the Weigert-Meyer principle?
|
Yes, 90% of the time.
|
|
|
What are the usual presenting complaints of a supernumerary kidney?
|
*Pain, fever, hypertension, and a palpable abdominal mass are the usual presenting complaints. Urinary infection or obstruction, or both, are the major conditions that lead to an evaluation. Ureteral ectopia from the supernumerary kidney may produce urinary incontinence, but this is extremely rare because of the hypoplastic nature of the involved renal element
*A palpable abdominal mass secondary to development of carcinoma in the supernumerary kidney has been noted in two patients |
|
|
What is renal ectopia?
|
*When the mature kidney fails to reach its normal location in the "renal" fossa, the condition is known as renal ectopia. The term is derived from the Greek words ek ("out") and topos ("place") and literally means "out of place
|
|
|
What is a calyceal diverticulum?
|
*A calyceal diverticulum is a cystic cavity lined by transitional epithelium, encased within the renal substance, and situated peripheral to a minor calyx, to which it is connected by a narrow channel.
|
|
|
Which calyx is most affected?
|
*Upper calyx
|
|
|
What is the difference between a type I and a type II calyceal diverticulum?
|
*Most diverticula, labeled type I, occur adjacent to an upper- or occasionally a lower-pole calyx. *Type II diverticula are larger and communicate with the renal pelvis directly; they tend to be the symptomatic ones
|
|
|
What is the preferred treatment for a calyceal diverticulum?
|
*but now percutaneous removal of the stones and ablation of the mucosal surface and communication with the collecting system
*Used to be partial nephrectomy |
|
|
What is megacalycosis?
|
*Megacalycosis is best defined as nonobstructive enlargement of calyces resulting from malformation of the renal papillae
|
|
|
Are there associated abnormalities with unipappilary kidney?
|
*The contralateral kdney is often absent.
*Genital anomalies are often present. The condition is frequently asymptomatic, being discovered fortuitously in most instances. More often than not there are abnormalities of the proximal ureter (i.e., megaureter, reflux, or ectopic insertion), |
|
|
What is a bifid renal pelvis?
|
Approximately 10% of normal renal pelves are bifid, the pelvis dividing first at or just within its entrance to the kidney to form two major calyces. A bifid pelvis should be considered a variant of normal.
|
|
|
Why is pulmonary hypoplasia involved in bilateral renal agenesis? Why is it not from the oligohydramnios?
|
*There is a significant reduction in the number of airway generations & decrease in acini formation in these fetuses. Airway divisioning occurs between the 12th & 16th weeks of gestation. A reduction in # of divisions implies an interference before 16th wk of gestation.
Contribution from the kidneys to the amniotic fluid volume before that time is small, if any *Anephric fetus fails to produce proline, which is needed for collagen formation in the bronchiolar tree. The kidney is the primary source of proline |
|
|
Are the adrenal glands affected in this syndrome?
|
*No, you may notice that they lie flatter than normal on ultrasound, just b/c kidneys are gone
|
|
|
What is amnion nodosum?
|
*small white, keratinized nodules found on the surface of the amniotic sac-
|
|
|
What is the embryological defect in unilateral renal agenesis?
|
*The fault lies most probably with the ureteral bud. Complete absence of a bud or aborted ureteral development prevents maturation of the metanephric blastema into adult kidney tissue.
|
|
|
What is a different possible mechansim besides the embryological theories behind unilateral renal agenesis?
|
*Again it could be involution of a multicystic dysplastic kidney. n fact, the presence of the splenic flexure of the bowel in its normal location and not in the left renal fossa suggests that a dysplastic or multicystic kidney may have started to form in the proper location but involuted before delivery.
|
|
|
In the cases of unilateral renal agenesis are there associated abnormalities on the contralateral side?
|
*Really the only things that are at increased incidence is ectopia or malrotation of the kidney or ureter is it.
*However, abnormalities of the contralateral collecting system are not uncommon, including ureteropelvic and ureterovesical junction obstruction in 11% and 7%, respectively *VUR around 30% |
|
|
Is the ipsilateral adrenal gland affected in URA?
|
*NO
|
|
|
What PE findings are clues to a possible URA?
|
*vas deferens or body and tail of the epididymis is missing or when an absent, septate, or hypoplastic vagina is associated with a unicornuate or bicornuate uterus. Bilateral absence of the vas and seminal vesical cysts have been associated as well. Radiologically, an absent left kidney can be surmised when a plain film of the abdomen demonstrates the gas pattern of the splenic flexure of the colon in a medial position because the colon now occupies the area normally reserved for the left kidney When this characteristic gas pattern is present, it is a very reliable sign. A similar finding showing the hepatic flexure positioned in the right renal fossa suggests congenital absence of the right kidney
|
|
|
Can people with one kidney engage in contact sports?
|
*You just have to tell them their risks, but yes.
|
|
|
What defines a supernumerary kidney?
|
*The supernumerary kidney is truly an accessory organ with its own collecting system, blood supply, and distinct encapsulated parenchymal mass.
It may be either totally separate from the normal kidney on the same side or connected to it by loose areolar tissue *ipsilateral ureters may be bifid or completely duplicated. The condition is not analogous to a single kidney with ureteral duplication, in which each collecting system drains portions of one parenchymatous mass surrounded by a single capsule. |
|
|
Can a supernumerary kidney cause incontinence?
|
*Rarely, the supernumerary kidney has a completely ectopic ureter opening into the vagina or introitus
|
|
|
In a patient with a supernumerary kidney are there usually associated GU anomalies?
|
*Except that associated with the ipsilateral ureter usually not.
|
|
|
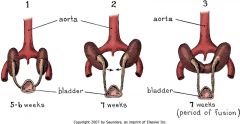
What is the embryological cause of renal ectopia?
|
*The ureteral bud, arising from the wolffian duct at the end of the 4th week, grows craniad toward the urogenital ridge, acquiring a cap of metanephric blastema by the 5th week
*The developing metanephric tissue and ureteral bud migrate cephalad, rotating medially on its long axis as it does so. The entire process is completed by the 8th week of gestation. *Factors that may prevent the orderly movement of kidneys include ureteral bud maldevelopment, defective metanephric tissue that by itself fails to induce ascent, genetic abnormalities, and maternal illnesses or teratogenic causes, because genital anomalies are common |
|
|
Is the ureter in an ectopic kidney usually normal or not?
|
*Usually it is. It is usually not redundant like in the situation of ptosis. It usually enters the bladder in the appropriate position at the trigone in the case of simple renal ectopia.
|
|
|
Are there usually abnormalities in the contralateral kidney in a patient with renal ectopia?
|
*No, usually the contralateral kidney is normal...however things are wrong more commonly than in general population.
*Hydronephrosis secondary to obstruction or reflux may be seen in as many as 25% of nonectopic contralateral kidneys. *Contralateral renal agenesis may be associated as well. |
|
|
Is there an increaesd risk of cancer in an ectopic kidney?
|
*NO
|
|
|
How can you get a more cephalad position of the kidney in renal ectopia?
|
*The mature kidney may be positioned more craniad than normal in patients who have had a history of omphalocele (Pinckney et al, 1978). When the liver herniates into the omphalocele sac with the intestines, the kidneys continue to ascend until they are stopped by the diaphragm. In all reported cases, both kidneys were affected and lay immediately beneath the diaphragm at the level of the 10th thoracic vertebra. The ureters are excessively long but otherwise normal
|
|
|
How in the world can you get a thoracic renal ectopia?
|
*The kidney reaches its adult location by the end of the 8th week of gestation. At this time, the diaphragmatic leaflets are formed as the pleuroperitoneal membrane separates the pleural from the peritoneal cavity. Mesenchymal tissues associated with this membrane eventually form the muscular component of the diaphragm. It is uncertain whether delayed closure of the diaphragmatic anlage allows for protracted renal ascent above the level of the future diaphragm or whether the kidney overshoots its usual position because of accelerated ascent before normal diaphragmatic closure
|
|
|
Do patients with a thoracic kidney usually have symptoms?
|
*Usually no
|
|
|
What is crossed renal ectopia?
|
*When a kidney is located on the side opposite from which its ureter inserts into the bladder, the condition is known as crossed ectopia.
|
|
|
In crossed renal ectopia are the kidneys on the ipsilateral side fused or not?
|
*90 of the time they are fused.
|
|
|
What is a lump kidney?
|
`*lump or cake kidney is a relatively rare form of fusion (Fig. 113-14). Extensive joining has taken place over a wide margin of maturing renal anlage. The total kidney mass is irregular and lobulated. Usually ascent progresses only as far as the sacral promontory, but in many instances the kidney remains within the true pelvis. Both renal pelves are anterior, and they drain separate areas of parenchyma. The ureters do not cross
|
|
|
What is the least common type of crossed renal ectopia?
|
*Least common variety of renal fusion is the crossed ectopic kidney that lies superior to the normal kidney
|
|
|
Do most patients with crossed ectopia have a normal trigone?
|
*Except for solitary crossed ectopia, in which there may be a hemitrigone or a poorly developed trigone with a rudimentary or absent ureter on the side of the ectopic kidney, most patients with crossed ectopia have a normal trigone with no indication that an anomaly of the upper urinary tract is present
|
|
|
What is a horseshoe kidney? How common is it amongst the other abnormalities of renal ectopia? More common in males or females?
|
*most common of all renal fusion anomalies.
*consists of two distinct renal masses lying vertically on either side of the midline and connected at their respective lower poles by a parenchymatous or fibrous isthmus that crosses the midplane of the body *More common in males than females |
|
|
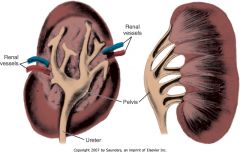
What is the anatomy of the horseshoe kidney?
|
*Note that the pelvis is anterior to the fused isthmus
*Usually this lies inferior to the IMA which prevents the ascent of the renal units as the isthmus gets stopped. *The isthmus most often lies anterior to the aorta and vena cava, but it is not unheard of for it to pass between the inferior vena cava and the aorta or even behind both great vessels |
|
|
What is the orientation of the collecting system in the horseshoe kidney?
|
*The calyces, normal in number, are atypical in orientation. Because the kidney fails to rotate, the calyces point posteriorly, and the axis of each pelvis remains in the vertical or obliquely lateral plane (on a line drawn from lower to upper poles).
|
|
|
What is the so called Rovsing sign associated with Horseshoe Kidney?
|
*abdominal pain, nausea, and vomiting on hyperextension of the spine-has been infrequently observed
|
|
|
IF patients have a stone in a horseshoe kidney can you do ESWL as a treatment?
|
*Yes, extracorporeal shock wave lithotripsy can render 68% of patients stone free, but percutaneous stone removal has achieved an 87.5% stone free rate
|
|
|
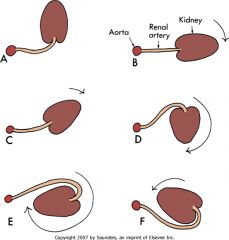
How does renal rotation occur during development?
|
*medial rotation of the collecting system occurs simultaneously with renal migration. The kidney starts to turn during the 6th week, just when it is leaving the true pelvis, and it completes this process, having rotated 90 degrees toward the midline, by the time ascent is complete, at the end of the 9th week of gestation.
|
|
|
What are anomalies of renal rotation in the vertical axis?
|
|
|
|
What symptoms do you see from rotation anomalies of the kidney?
|
*Realy the main one you might see is that of obstruction.
|
|
|
What is the correct nomenclature for various vascular issues with the kidney?
|
*Multiple renal arteries is the correct term to describe any kidney supplied by more than one vessel. The term anomalous vessels or aberrant vessels should be reserved for those arteries that originate from vessels other than the aorta or main renal artery. The term accessory vessels denotes two or more arterial branches supplying the same renal segment.
|
|
|
What is the division of the kidney based on its vasculature?
|
*On the basis of vascular supply, the renal parenchyma is divided into five segments: apical, upper, middle, lower, and posterior
|
|
|
Where do you incise an obstructed UPJ endourologically?
|
authors have noted a close association between the inferior branch to the main renal vein and the anterior inferior aspect of the renal pelvis in 40% of kid-neys. They cautioned that an endourologic incision of an obstructed UPJ should be done laterally and posteriorly instead of anteriorly to avoid injury to this vessel.
|
|
|
What is the most common type of renal artery aneurysm?
|
*saccular aneurysm, a localized outpouching that communicates with the arterial lumen by a narrow or wide opening, is the most common type, accounting for 93% of all aneurysms
|
|
|
What is a fusiform renal artery aneurysm?
|
*When the aneurysm is located at the bifurcation of the main renal artery and its anterior and posterior divisions or at one of the more distal branchings, it is considered to be congenital in origin and is called the fusiform type
|
|
|
What are potential symptoms of a renal artery aneurysm?
|
*Most renal artery aneurysms are silent, especially in children (48%). Some produce symptoms at a later age in relation to their size because there is a tendency for them to enlarge with time.
*Pain (15%), hematuria (microscopic and macroscopic) (30%), and hypertension (55%) secondary to compression of adjacent parenchyma or to altered blood flow within the vascular tree can occur. *The hypertension is renin mediated, secondary to relative parenchymal ischemia |
|
|
How is a renal artery aneurysm diagnosed?
|
*The diagnosis may be suspected when a pulsatile mass is palpated in the region of the renal hilum or when a bruit is heard on abdominal auscultation.
*A wreathlike calcification in the area of the renal artery or its branches (30%) is highly suggestive, but this finding is often missed on a plain abdominal radiograph. *Color Doppler imaging will demonstrate decreased flow, but selective renal angiography, digital subtraction angiography, or, more recently, color Doppler ultrasound or magnetic resonance angiography is needed to confirm the diagnosis |
|
|
When is intervention for a renal artery aneurysm suggested?
|
*the hypertension cannot be easily controlled; (2) incomplete ringlike calcification is present; (3) the aneurysm is larger than 2.5 cm; (4) the patient is female and of child-bearing age, because rupture during pregnancy is a likely possibility; (5) the aneurysm increases in size on serial angiograms; or (6) an arteriovenous fistula is present
|
|
|
What are the two types of renal AV fistulas?
|
*Congenital
*Acquired - such as that from renal biopsy, percutaneous renal surgery, infection, trauma |
|
|
When do congenital AV fistulas usually present?
|
*lthough they are considered congenital (because similar arteriovenous malformations can be found elsewhere in the body), they rarely present clinically before the third or fourth decade. Women are affected three times as often as men, and the right kidney is involved slightly more often than the left
|
|
|
What are symptoms of a congenital AV fistula?
|
*hemodynamic derangement often produces a loud bruit (in 75% of cases). Diminished perfusion of renal parenchyma distal to the fistulous site leads to relative ischemia and renin-mediated hypertension (40% to 50%)
*The increased venous return and high cardiac output with concomitant diminution in peripheral resistance may result in left ventricular hypertrophy and eventually in high-output cardiac failure (50%) *arteriovenous fistula usually is located close to the collecting system. As a result, macroscopic and microscopic hematuria occurs in more than 75% of affected individuals |
|
|
What is the best way to diagnose an AV fistula?
|
*Three-dimensional Doppler ultrasound and MR angiography are more accurate and noninvasive tests (Mohaupt et al, 1999; Ishikawa et al, 2004), but selective renal arteriography or digital subtraction angiography is the most definitive method for diagnosing the lesion
|
|
|
What are complications of calyceal diverticula that can cause complications over time?
|
*progressively distend with trapped urine.
*Infection, milk of calcium (crystallization of calcium salts without actual stone formation), or true stone formation are complications of stasis or obstruction that can produce symptom. *Hematuria, pain, and urinary tract infection may be seen in the presence of stones |
|
|
How would you diagnose a calyceal diverticulum?
|
*CT urogram
*Excretory urogram or retrograde urogram |
|
|
How might milk of calcium look on imaging?
|
*Milk of calcium appears on excretory urography as a crescent-shaped density that changes as the patient assumes different positions.
|
|
|
What are indications for surgery in a patient with a calyceal diverticulum?
|
*Persistent pain, resistant urinary tract infections, hematuria, and milk of calcium or true calculus formation are indications for surgery
|
|
|
How do you know a patient with megacalycosis is not obstructed?
|
*The renal pelvis is not dilated, nor is its wall thickened, and the UPJ is normally funneled without evidence of obstruction
*The cortical tissue around the abnormal calyx is normal in thickness and shows no signs of scarring or chronic inflammation *Diuretic renography reveals a normal pattern for uptake and washout of the isotope, whether or not the Whitaker test generates high pressure in the collecting system (Gomes Tellado et al, 1997). Therefore, an obstructive picture cannot be proven. Long-term follow-up of patients with this anomaly does not reveal any progression of the anatomic derangement or functional impairment of the kidney |
|
|
What is a unipappilary kidney?
|
*he cause is thought to be a failure of progressive branching after the first three to five generations (which create the pelvis) of the ureteral bud
*solitary calyx drains a ridgelike papilla. Nephrons attach to fewer collecting tubules, which then drain directly into the pelvis. |
|
|
What is infundibulopelvic stenosis?
|
*Infundibulopelvic stenosis most likely forms a link between cystic dysplasia of the kidney and the grossly hydronephrotic organ
*Infundibulopelvic stenosis is usually bilateral and is commonly associated with vesicoureteral reflux, suggesting an abnormality of the entire ureteral bud. |
|
|
Are upper tract urothelial tumors commonly asymptomatic?
|
*No, they are almost never found at autopsy and usually present during a patient's lifetime symptomatically.
|
|
|
Who are generally older, patients with bladder cancer or patients with upper tract TCC?
|
*Upper tract TCC, but not by a large margin
|
|
|
What are risk factors for upper tract TCC after bladder cancer and where does it occur? What is a major risk factor for upper tract TCC after bladder Ca?
|
The incidence of upper tract recurrence has been shown to be higher in patients with carcinoma in situ than in patients with superficial
transitional cell carcinoma and in patients treated with cystectomy for carcinoma in situ rather than for invasive cancer ( Solsona et al, 1997 ). On pathologic evaluation, recurrence is most likely to be superficial (Ta, T1, Tis) and to occur in the distal ureter only (47%) |
|

1.)What does the above image show?
|
Megacalycosis is a rare congenital abnormality in which all the renal calyces are enlarged, without any evidence of obstruction [1, 2].
The renal calyces as well as being dilated are frequently increased in number. Megacalycosis usually occurs unilaterally, as an isolated anomaly, being more frequent on the left side. The renal papillae are hypoplastic and, instead of protruding into the calyceal cavity, they surround the hypotonic calyces. The differential diagnosis should be established with congenital hydronephrosis, polycalycosis, and hydrocalycosis resulting from infundibular stenosis. |