Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
118 Cards in this Set
- Front
- Back
|
When neurons degenerate, what types of disorders can we get? |

(1) Dementia
(2) Movement disorders |
|
|
Neurodegenerative disorders are characterized by what?
|
Loss of neurons within the gray matter.
|
|
|
MCC of dementia?
|
Alzheimer's
|
|
|
What is Alzheimer's disease?
|

Degenerative disease of the cortex. APP-receptor is broken down by a beta-secretase creating a AB amyloid that is nondegradable. Alpha-secretase products are easily degradable. Deposition of amyloid results in this disease.
|
|
|
Clinical features of Alzheimer's?
|
All symptoms are based on dementia.
(1) Slow-onset memory loss (years to develop) (2) Progressive disorientation (3) Develop cognitive dysfunction (motor skills and language affected) (4) Behavioral and personality changes (prefrontal cortex) (5) Eventually they become mute and bedridden |
|
|
What is dementia?
|
Memory loss plus cognitive dysfunction without any loss of consciousness.
|
|
|
The slow-onset memory loss seen in Alzheimer's disease begins with ________ memory and ends with ___________.
|
recent; distant
|
|
|
True or false: Early in alzheimers disease we will see focal neurologic deficits.
|
False. We do not see this early in the disease.
|
|
|
Most cases of Alzheimer's disease are _________. Major risk factor for this?
|
sporadic
Age. |
|
|
What are the two forms of Alzheimers?
|
(1) Sporadic form
(2) Early form |
|
|
A special allele greatly increases the risk for sporadic Alzheimer's disease, what is it?
|
Epsilon 4 allele of apolipoprotein E (increased conversion to beta form)
|
|
|
What allele of apolipoprotein E would decrease the risk for Alzheimer's disease?
|
Epsilon 2 allele
(4 is higher than 2 and has an increased risk, 2 is lower and has a lower risk) |
|
|
The key genetic mutation that results in early-onset (familial cases) of Alzheimer's disease is?
|
Presenilin (Presenilin 1)
|
|
|
By the age of 40 a large number of patients with Downs will have developed _____________.
|
Alzheimer's (three copies of chromosome 21, and Amyloid Precursor Protein is located on this chromosome)
|
|
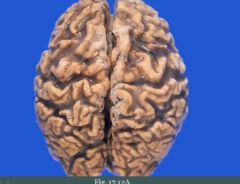
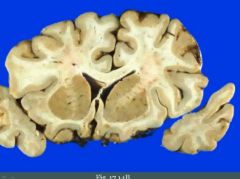
These are pathologic features of what?
|
Alzheimers. We see diffuse cerebral atrophy. Narrowing of gyri is seen and widening of sulci.
|
|
|
What is hydrocephalus ex vacuo?
|
Consequence of atrophy of the brain. It makes the ventricles dilate.
|
|
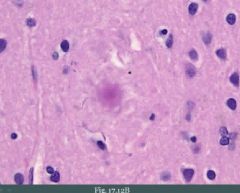
What is this and what is it composed of?
|
Pathologic hallmark of Alzheimer's. Neuritic plaque (traps neuritic processes). Contains Abeta-amyloid.
|
|
|
What is cerebral amyloid angiopathy? Possible consequences?
|
It's Abeta-amyloid depositing around blood vessels in the brain. Weakens wall of vessels which increases risk for hemorrhage.
|
|

What is this?
|
Pathologic hallmark of Alzheimer's. It is neurofibrillary tangles. Tau-protein becomes hyperphosphorylated. It can no longer assist in the organization of microtubules.
|
|
|
Diagnosis of Alzheimer's?
|
Presumptive diagnosis that is made clinically only after all other causes are exluded. It is confirmed with pathology at autopsy.
|
|
|
What is vascular dementia?
|
Multifocal infarction and injury that creates dementia. It's a consequence of moderate global cerebral ischemia.
|
|
|
Vascular dementia is due to?
|
(1) HTN
(2) Atherosclerosis (3) Vasculitis These decreased blood flow to the brain. |
|
|
What is the second most common cause of dementia?
|
Vascular dementia
|
|
|
What is Pick disease?
|
Degenerative disease of frontal and temporal cortex. It spares the parietal and occipital lobes.
("It picks the frontal and temporal cortex") |
|
|
What is seen microscopically in Pick disease?
|
Round aggregates of tau protein in neurons of cortex.
|
|
|
Clinical features of Picks?
|
(1) Frontal cortex --> Behavioral symptoms
(2) Temporal cortex --> Language symptoms These arise early. Progresses to dementia. |
|
|
What is Parkinsons disease?
|
Degenerative loss of dopaminergic neurons in the substantia nigra pars compacta (basal ganglia)
|
|
|
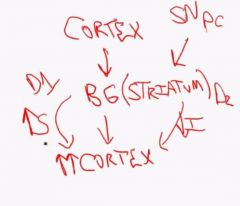
Draw a simple flowchart of the interactions between cortex and basal ganglia.
|
|
|
|
The key processing center in the basal ganglia is called the __________.
|
striatum
|
|
|
Parkinson disorder is a _______________ (rare/common) disorder related to _________.
|
common; aging
|
|
|
What is the etiology of Parkinsons disease?
|
Unknown.
|
|
|
Rare cases of Parkinsons are related to ________.
|
MPTP (contaminant in illicit drugs)
|
|
|
Clinical features of Parkinsons disease?
|
(1) Tremor (pill rolling tremor)
(2) Rigidity (cogwheel rigidity of extremities) (3) Akinesia/bradykinesia (slow voluntary movements, can't move muscles of face leads to a expressionless mask-like face) (4) Postural instability, shuffling gait ("Trapped in your body") |
|

What is this and is this normal?
|
Loss of pigmented neurons in the substantia nigra.
|
|
|
In parkinsons disease, what would you see in the substantia nigra?
|
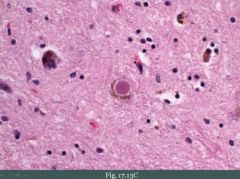
Round eosinophilic inclusions that are called Lewy bodies. It is composed of alpha-synuclein.
|
|
|
What is the hallmark of Parkinsons disease histologically?
|
Lewy bodies.
|
|
|
What is a common feature of late Parkinsons disease?
|
Dementia.
|
|
|
A man with symptoms of Parkinsons has early-onset dementia. What could this be?
|
Parkinsons has late onset dementia. This is Lewy body dementia which is characterized by dementia, hallucinations, and parkinsonian features with CORTICAL Lewy bodies.
|
|
|
What is Huntingtons disease?
|
Degeneration of GABAergic neurons in the caudate nucleus of the basal ganglia. This nucleus provides an inhibitory stimuli to the cortex.
|
|
|
Role of caudate nucleus?
|
Has an "inhibitory hold" on the cortex, preventing you from having random firing of neurons with flailing uncoordinated movements.
|
|
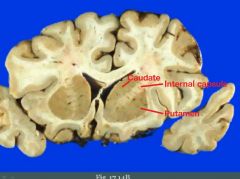
Mark the caudate nucleus, putamen and internal capsule.
|
|
|

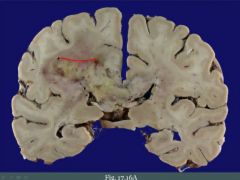
What is this?
|
Hydrocephalus ex vacuo. Patient had Huntington's disease (absence of caudate nucleus)
|
|
|
Huntingtons disorder is an ______ (AR/AD) disorder. It is due to what?
|
AD.
It is due to an expanded trinucleotide repeat (CAG) in the huntingtin gene. |
|
|
Huntingtons disease display earlier onset disease in subsequent generations which is called ____________. A further expansion of trinucleotides occur where and when?
|
anticipation
Further expansion occurs during spermatogenesis. |
|
|
Clinical features of Huntington's disease?
|
(1) Chorea (brief irregular movement like dancing) or athetosis (slow involuntary snake like movements)
(2) Progresses to dementia and depression (3) Suicide is common cause of death |
|
|
What is normal pressure hydrocephalus? The result?
|
Increased CSF results in dilated ventricles. This stretches the corona radiata (goes around ventricles) and can cause dementia in adults.
|
|
|
In normal pressure hydrocephalus, the increased CSF can stretch the corona radiata producing what clinical features?
|
(1) Urinary incontinence
(2) Gait instability (3) Dementia ("Wet, wacky and wobbly") |
|
|
What is the etiology of normal pressure hydrocephalus?
|
Usually idiopathic.
|
|
|
You do a lumbar puncture of a patient with symptoms of dementia. A short period after this is completed, symptoms appear to improve in the patient. What is going on?
|
Normal pressure hydrocephalus where there is increased CSF. LP ameliorates symptoms.
|
|
|
Treatment of normal pressure hydrocephalus?
|
Shunt CSF from ventricles into the peritoneum.
|
|
|
Why is there an increased CSF in normal pressure hydrocephalus?
|
For some reason there is a decreased resorption of CSF via the arachnoid granulations into the venous sinuses.
|
|
|
What is a spongiform encephalopathy?
|
Degenerative disease due to prion proteins. We see white spongy spaces in the brain parenchyma.
|
|
|
All of us have prion protein in our brains and it is normally in what configuration?
|
PrP^C (alpha)
|
|
|
What prion protein do we see in spongiform encephalopathies?
|
PrP^SC (beta pleated sheet). Creates more of the pathologic protein from alpha to beta.
|
|
|
What ways can lead to formation of a beta pleated sheet conformation of PrP?
|
(1) Sporadic
- Alpha sporadically converts. (2) Inherited - Inherit a bad gene. (3) Transmitted - When you're exposed to the beta-pleated protein |
|
|
MC form of spongiform encephalopathy?
|
Creutfeldt-Jakob disease.
|
|
|
Creutzfeldt-Jakob disease is usually _____________ (sporadic/inherited).
|
sporadic, it rarely arises due to exposure to prion infected human tissue
|
|
|
How could you be exposed to beta pleated sheet configurations of PrP?
|
E.g. corneal transplants or HGH preparations from a patient with CJD
|
|
|
Hallmark of CJD?
|
Rapidly progressive dementia (weeks to months)
|
|
|
Clinical features of CJD?
|
(1) Rapidly progressive dementia
(2) Ataxia (3) Startle myoclonus |
|
|
What is seen on EEG of patients with CJD?
|
Spike-wave complexes are seen on EEG.
|
|
|
CJD results in death, usually within _______ year(s).
|
1 year
|
|
|
What is vCJD?
|
Variant of CJD. Related to exposure to bovine spongiform encephalopathy ('mad cow'). It occurs in younger patients.
|
|
|
What is familial fatal insomnia?
|
Spongiform encephalopathy. Inherited prion disease characterized by insomnia and exaggerated startle response.
|
|
|
CNS tumors can be _________ or __________.
|
metastatic; primary
|
|
|
How do metastatic tumors of the CNS often present?
|
Metastatic tumors present as multiple, well-circumscribed lesions most often at the gray-white junction.
|
|
|
Three MC cancers that like to go to the brain?
|
Lung, breast and kidney. Prostate as well.
|
|
|
Primary tumors of the CNS are classified according to what?
|
(1) Cell type
|
|
|
Malignant tumors are locally ___________ however they rarely __________.
|
destructive; metastasize outside the CNS
|
|
|
Five key cell types in the brain?
|
(1) Astroglial cells
(2) Oligodendrocytes (3) Ependymal cells (4) Neurons (5) Meningothelial cells |
|
|
______________ is the most abundant glial cell.
|
Astrocytes
|
|
|
The tumor that classically arises from astrocytes in kids is called a?
|
Pilocytic astrocytoma (benign)
|
|
|
MC tumor of astrocytes in adults?
|
GBM (malignant)
|
|
|
This is the MC CNS tumors in adults.
|
GBM
|
|
|
Oligodendriocytes form a tumor called ______________ in adults.
|
Oligodendroglioma
|
|
|
Ependymal cells can form a _____________ (tumor) which is classically seen in ___________ (children/adults).
|
ependymoma; children
|
|
|
Why don't we (normally) see tumors of neurons in adults?
|
In children, they divide to a greater extent.
|
|
|
A tumor of neurons in children is called a ________________.
|
Medulloblastoma (which is a tumor derived from neuroectoderm)
|
|
|
Meningothelial cells can form a _____________ which is usually seen in _______________.
|
meningioma; adult females
|
|
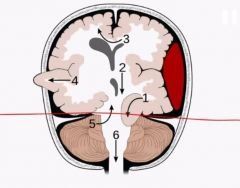
The red line represents? Tumors in adults occur where in the relation to the red line?
|
Tentorium
They usually occur above the tentorium and in children it is usually below |
|
|
Glioblastoma multiforme is a ____________ (benign/malignant) ___________ (low/high) grade tumor of ________.
|
malignant; high; astrocytes
|
|
What is this?
|
GBM. Can cross the midline (corpus callosum)
("Butterfly glioma") |
|
|
Histologic characteristics of GBM?
|
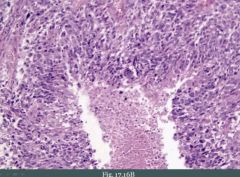
Note necrosis in the middle and cells "lining" up around it which is called pseudopallisading. Endothelial cell proliferation is also seen (glomeruloid-bodies).
|
|
|
What filament is present within glial cells?
|
GFAP (intermediate filament)
|
|
|
Meningioma is a ___________ (benign/malign) tumor of _________ cells.
|
benign; arachnoid
|
|
|
This is the MC benign CNS tumor in adults.
|
Meningioma
|
|
|
Meningiomas express __________ receptors.
|
estrogen
|
|
|
Imaging of a meningioma reveals what? What may it present as clinically?
|
Round mass attached to the dura (with reactive bone formation above it). May present with seizures from pushing on the cortex.
|
|
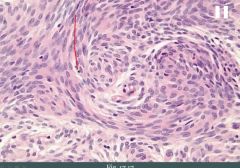
This histologic image could represent what tumor?
|
Meningioma, note the whorled appearance of cells.
This tumor can also result in abundant psammoma bodies. |
|
|
Schwannomas involve ________ or _________ nerves.
|
cranial; spinal
|
|
|
Schwannomas especially involve what cranial nerve?
|
CN VIII at cerebellopontine angle.
|
|
|
Schwannomas are positive for what marker?
|
S100
|
|
|
Bilateral schwannomas are seen in?
|
Neurofibromatosis type 2
|
|
|
Oligodendrogliomas are ____________ (benign/malignant) tumor of ________________.
|
malignant; oligodendrocytes
|
|
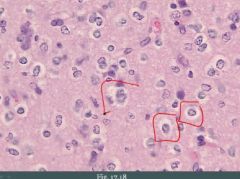
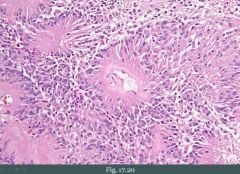
The histologic picture is classic for what tumor?
|
Note all the fried eggs. Classic for oligodendroglioma.
|
|
|
Oligodendrogliomas form a __________ mass in the _______ matter. It usually involves what lobe?
|
calcified; white
usually involves frontal lobe |
|
|
Oligodendrogliomas present with ______________.
|
seizures
|
|
|
This is the MC CNS tumor in children.
|
Pilocytic astrocytoma
|
|
|
Pilocytic astrocytomas usually arise in the ____________.
|
cerebellum
|
|

What could this be?
|
Note the dark cystic lesion with a nodule growing on its wall. This is classic for pilocytic astrocytoma.
("Pilocystic astrocytoma") |
|
|
Histology of pilocytic astrocytoma would show what?
|
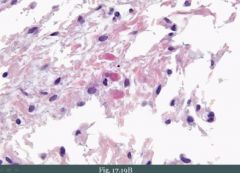
Astrocytes with thick eosinophilic processes (Rosenthal fibers)
|
|
|
Pilocytic astrocytoma would be __________ (GFAP/S100) positive.
|
GFAP
|
|
|
What is a medulloblastoma?
|
Malignant tumor derived from granular cells of cerebellum (neuroectodermal tissue)
|
|
|
Histology of medulloblastoma reveals [...]
|
Small, round blue cells with Homer-Wright rosettes that may be present.
|
|
|
Prognosis of medulloblastoma?
|
Poor. It grows rapidly and spreads via the CSF. It can go to the spinal cord.
|
|
|
What is a drop metastasis?
|
Medulloblastoma that metastasizes to the spinal cord ("drops down")
|
|
|
What is an ependymoma? Usually seen in?
|
Malignant tumor of the ependymal cells.
It is usually seen in children. |
|
|
Ependymomas usually arise in?
|
4th ventricle
|
|
|
How do ependymomas present?
|
May present with hydrocephalus.
|
|
Key histologic findings in ependymomas?
|
Pseudorosettes (blue cells) lining up against blood vessel
|
|
|
Craniopharyngioma is a cranial tumor that arises from?
|
Epithelial remnants of Rathke's pouch.
(Cranio - in the cranium, pharyng - arises from pharynx) |
|
|
In embryogenesis, an __________ protrusion of the __________ results in formation of the anterior pituitary while a __________ protrusion of the ______________ results in formation of the posterior pituitary.
|
upward; floor of the mouth; downward; base of the brain
|
|
|
The upwards protrusion of the floor of the mouth during embryogenesis is called?
|
Rathke's pouch
|
|
|
Craniopharyngioma presents as a what?
|
Supratentorial mass in a child or young adult.
|
|
|
Craniopharyngiomas can compress the ___________ resulting in what?
|
optic chiasm; bitemporal hemianopsia
|
|
|
Bitemporal hemianopsia in a child. What should you think especially about?
|
Craniopharyngioma.
|
|
|
How does a craniopharyngioma look like on imaging?
|
Often calcified
(It arises from floor of the mouth and could contain tooth-like tissue) |
|
|
Craniopharyngioma is ___________ (benign/malignant).
|
benign but tend to recur after resection
|