Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
59 Cards in this Set
- Front
- Back
|
What is endocarditis?
|
Inflammation of endocardium, predominantly of the lining of the cardiac valves.
|
|
|
Endocarditis is usually due to __________________.
|
bacterial infection
|
|
|
Most common overall cause of endocarditis?
|
Streptococcus viridans
|
|
|
The virulence of S. viridans is _________ (high/low).
|
low, therefore it can only infect previously damaged valves
|
|
|
S. viridans infects ______________ (intact/previously damaged) valves.
|
previously damaged (low-virulence)
|
|
|
What is the result of a S. viridans infection of the valves, what happens to the valve?
|
Small vegetations that do not destroy valve (low virulence)
|
|
|
Infection with S. viridans of previously damaged cardiac valves is also called ___________________.
|
subacute endocarditis
|
|
|
Pathogenesis of endocarditis?
|
(1) Damaged endocardial surface (exposes tissue factor and collagen) develops thrombotic vegetations (PLTs and fibrin)
(2) Transient bacteremia leads to trapping of bacteria in vegetations. |
|
|
A person is undergoing a dental procedure. Why is this sometimes important when talking about IE?
|
Can force bacteria into blood (transient bacteremia) that can be trapped in the thrombotic vegetations created by the previously damaged heart valve.
|
|
|
What is the MCC of IE in IV-drug users?
|
S. aureus
|
|
|
The virulence of S. aureus is _________ (high/low) and it infects ____________ (healthy/previously dmged valves).
|
high; healthy
|
|
|
An heroin addict has endocarditis. What valve is usually involved?
|
Tricuspid (they travel by veins)
|
|
|
What is the result of S. aureus infective endocarditis?
|

Results in large vegetations that destroy the valve (acute endocarditis)
|
|
|
What organism causes endocarditis of prostatic valves?
|
S. epidermidis
|
|
|
A patient with colorectal cancer is known to have infectious endocarditis. What organism is most likely involved?
|
S. bovis
|
|
|
A patient presents with infectious endocarditis. The organism is S. bovis, what should you check for?
|
Colorectal carcinoma
|
|
|
An endocarditis blood culture comes back negative. What organisms could you suspect?
|
HACEK organisms
Haemophilus Actinobacillus Cardiobacterium Eikenella Kingella |
|
|
Clinical features of infective endocarditis?
|
(1) Fever
(2) Murmur (vegetations disrupt flow) - Can get septic embolization of vegetations (3) Janeway lesions (consequence of septic embolization) - Erythematous non-tender lesions on palms & soles (4) Osler nodes (painful lesions on fingers and toes) - Due to septic emboli (5) Splinter hemorrhages of the nail bed - Due to septic emboli |
|
|
Which one is a painful lesion, Janeway lesions or Osler nodes?
|
Osler nodes ("Ouch Ouch Osler")
|
|
|
Infectious endocarditis is associated with what hematologic disease?
|
Anemia of chronic disease
|
|
|
Laboratory findings in infectious endocarditis?
|
(1) Generally positive blood culture
(2) Anemia of chronic disease (high ferritin, TIBC low) |
|
|
What can be done to detect lesions on valves?
|
Transesophageal echocardiography (TEE)
|
|
|
What is nonbacterial thrombotic endocarditis?
|
Sterile vegetations that arise with hypercoagulable state or underlying adenocarcinoma. Vegetations arise on mitral valve along lines of closure and results in regurgitation.
|
|
|
This endocarditis is seen in systemic lupus erythematosus. Describe it.
|
Libman-Sacks endocarditis.
(1) Sterile vegetations associated with SLE (2) Vegetations present on surface and undersurface (both sides) of mitral valve (3) Result in mitral regurgitation. |
|
|
Libman-Sacks endocarditis is highly characteristic of having ______________.
|
Sterile vegetations on both sides of leaflets
|
|
|
What is a cardiomyopathy?
|
Myocardial diseases that lead to cardiac dysfunction
|
|
|
What is the MC form of cardiomyopathy?
|
Dilated cardiomyopathy
|
|
|
What parts of the heart are dilated in dilated cardiomyopathy?
|

All four chambers
|
|
|
What is the physiologic problem in dilated cardiomyopathy?
|
It's gonna result in a systolic dysfunction leading to biventricular CHF.
|
|
|
Complications of dilated cardiomyopathy?
|
(1) Mitral & tricuspid regurgitation
(2) Arrhythmia Both are due to stretching. |
|
|
Most commonly the cause of dilated cardiomyopathy is __________.
|
idiopathic
|
|
|
What causes are there of dilated cardiomyopathy?
|
(1) Idiopathic
(2) Genetic mutations (AD is MC, cytoskeletal prot. are affected) (3) Myocarditis (Coxsackievirus B) (4) Alcohol abuse (5) Drugs (doxorubicin, daunorubicin) (6) Pregnancy (late third trimester or within 6 months postpartum) |
|
|
Treatment of dilated cardiomyopathy?
|
Transplant
|
|
|
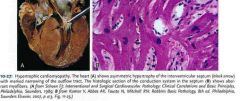
What is hypertrophic cardiomyopathy?
|
Massive hypertrophy of the left ventricle
|
|
|
Hypertrophyic cardiomyopathy is due to what?
|
AD genetic mutations in sarcomere proteins (e.g., myosin heavy chain gene)
|
|
|
What is the MCC of sudden death in young individuals?
|
Hypertrophic cardiomyopathy
|
|
|
How are patients with hypertrophic cardiomyopathy going to present?
|
(1) Decreased cardiac output (heart can't fill)
(2) Sudden death due to ventricular arrhythmias; common cause of sudden death in young athletes (3) Syncope with exercise |
|
|
Why do we see syncope with exercise in people with hypertrophic cardiomyopathy?
|
Because of the preferential involvement of the interventricular septum close to the aortic valve (relative block, like aortic stenosis).
|
|
|
On biopsy of a person with hypertrophic cardiomyopathy you would see what?
|

Myocytes should normally be lined up nicely in parallel. However, on this biopsy they are in a disarray (going in every single direction). This is what we see in this heart disease.
|
|
|
What is restrictive cardiomyopathy?
|
Decreased compliance of ventricular endomyocardium. It restricts filling during diastole.
|
|
|
Causes of restrictive cardiomyopathy? (7)
|
(1) Amyloidosis
(2) Sarcoidosis (3) Hemachromatosis (4) Endocardial fibroelastosis (children) (5) Loeffler syndrome (6) After open-heart surgery (7) Systemic sclerosis |
|
|
What is Loeffler syndrome?
|
There is peripheral eosinophilia with increase in toxic products (esp. MBP) --> Endomyocardial necrosis --> Scarring --> Thrombi covers area and gets organized
|
|
|
Endocardial fibroelastosis is seen in the first ______ years of life.
|
2
|
|
|
Patients with restrictive cardiomyopathy will present with?
|
CHF (blood backs up)
|
|
|
A classic finding in EKG in restrictive cardiomyopathy?
|
Low-voltage EKG with diminished QRS amplitudes.
|
|
|
What is a cardiac myxoma?
|
Cardiac tumor. Benign mesenchymal proliferation with a gelatinous appearance.
|
|
|
What would a cardiac myxoma show on histology?
|
Abundant ground substance on histology.
|
|
|
What is the MC primary cardiac tumor in adults?
|
Cardiac myxoma
|
|
|
How and where does a cardiac myxoma grow?
|
Pedunculated mass in the left atrium.
|
|
|
Cardiac myxomas can cause what?
|
Syncope due to obstruction of mitral valve.
|
|
|
What is a rhabdomyoma?
|
Benign hamartoma of skeletal muscle.
|
|
|
What is the most common primary cardiac tumor in children?
|
Rhabdomyoma
|
|
|
What heart tumor is associated with tuberous sclerosis?
|
Rhabdomyoma
|
|
|
In tuberous sclerosis we see multisystem _____________.
|
hamartomas
|
|
|
Tuberous sclerosis is an _______ (AR/AD) disease.
|
AD
|
|
|
Rhabdomyomas usually arise in what part of the heart?
|
Ventricle
|
|
|
What is more common, metastasis or primary tumors of the heart?
|
Metastasis
|
|
|
Common metastasis to the heart include?
|
(1) Breast carcinoma
(2) Lung carcinoma (3) Melanoma (4) Lymphoma |
|
|
A melanoma metastasizes to the heart. Where would it typically go?
|
Pericardium. It results in a pericardial effusion.
|