Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
48 Cards in this Set
- Front
- Back
|
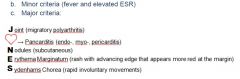
What types of valvular disorders may we get?
|
(1) Stenosis (narrows)
(2) Regurgitation (backflow) |
|
|
What is acute rheumatic fever?
|
Systemic complication of pharyngitis due to GAS.
|
|
|
Acute rheumatic fever affects which age group of patients and when does it present?
|
Affects children 2-3 weeks after strep throat
|
|
|
Acute rheumatic fever is caused by _____________.
|
molecular mimicry; bacterial M protein resembles human tissues
|
|
|
Diagnosis of ARF is based on what?
|
You need evidence of a prior GAS infection (ASO or anti-DNase B titer) and the above.
|
|

What might this be? What could it lead to?
|
Tiny vegetations on heart seen in ARF due to endocarditis. May lead to mitral regurgitation.
|
|
|
As far as myocarditis in ARF is concerned, what may we see on histology?
|
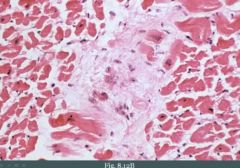
The image shows an aschoff body. It's a focus of chronic inflammation with giant cells and fibrinoid material (degenerated collagen) with a group of cells called the Anitschkow cells.
|
|

These cells are seen in a biopsy of the myocardium of a child with a previous strep throat. What are they called?
|

Anischkow cells, seen in Aschoff bodies. It's a hallmark cell.
Note the "caterpillar" nucleus. |
|
|
What is the MCC of death during the acute phase of acute rheumatic fever?
|
Myocarditis (may show as friction rub)
|
|
|
What is chronic rheumatic valve disease?
|
Repeated infections lead to persistent attacks on valves with scarring. Scarring results in stenosis. Almost always involves the mitral valve.
|
|
|
If ARF does involve a valve outside of mitral valve it will involve what?
|
aortic valve
|
|
|
Complication of chronic rheumatic valve disease?
|
Damage to the valves may lead to endocarditis.
|
|

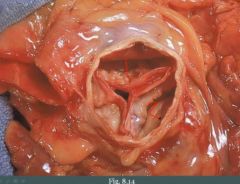
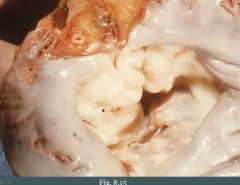
What is this?
|
"Fishmouth appearance" of aortic valve. Fusion of commissures is seen. Due to chronic rheumatic valve disease.
|
|
|
Normally the aortic valve is ______ cm^2 but in aortic stenosis it becomes less than _____ cm^2.
|
4;1
|
|
|
Aortic stenosis is a ____________ disorder.
|
"wear and tear"
It is usually due to fibrosis and calcification from "wear and tear". |
|
|
When does aortic stenosis typically present?
|
Late adulthood (>60)
|
|
|
What would hasten the disease onset of aortic stenosis?
|
Bicuspid aortic valve
|
|
What is this and what age would the patient present?
|
Aortic stenosis.
Late adulthood, > 60 yo |
|
|
How to distinguish aortic stenosis from wear and tear with aortic stenosis from chronic rheumatic valve disease?
|
(1) CRVD is going to have coexisting mitral stenosis
(2) CRVD is going to have fusion of the commissures |
|
|
Compensation by the heart to aortic stenosis leads to a _______________________.
|
prolonged asymptomatic stage
|
|
|
You auscultate a 70 year old man. He is known to have a mild anemia. You hear a "click" on auscultation during systole followed by a crescendo-decrescendo murmur. What could this be? Explain the findings.
|
(1) Stenosed valve may lead to microangiopathic hemolytic anemia. Poor RBCs are smashed into the degenerated calcified valve.
(2) Heart will eventually blow open the stenosed valve (click) creating a rush of blood (crescendo) followed by a decrescendo. |
|
|
Complications of aortic stenosis include [...]
|
(1) Concentric left ventricular hypertrophy
(2) Angina and syncope with exercise (limited ability to increase blood flow across the valve) (3) Microangiopathic hemolytic anemia |
|
|
Treatment of aortic stenosis?
|
You replace the valve. This is done after the onset of complications (normally).
|
|
|
What is aortic regurgitation?
|
Backflow of blood from the aorta into the left ventricle during diastole.
|
|
|
Aortic regurgitation arises due to _________________ or ____________.
|
aortic root dilation (e.g., syphilitic aneurysm); valve damage (e.g., IE)
|
|
|
Clinical features of aortig regurgitation?
|
(1) Early, "blowing" diastolic murmur
(2) Hyperdynamic circulation - Bounding pulses (strong pulse) - Pulsating nail bed - Head bobbing (3) LV dilation and eccentric (not concentric, or the entire ventricle) hypertrophy |
|
|
Why may the head of a patient with aortic regurgitation bob during regular heart beats?
|
Hyperdynamic circulation. Due to a high pulse pressure.
|
|
|
In aortic regurgitation the diastolic pressure ___________ and the systolic pressure ___________.
|
decreases; increases
|
|
|
Treatment of aortig regurgitation?
|
Valve replacement when LV dysfunction develops.
|
|
|
What is mitral valve prolapse?
|
Ballooning (oppsvulming) of mitral valve into left atrium during systole.
|
|
|
Mitral valve prolapse is due to what?
|
Myxoid degeneration in valve making it floppy. Etiology however is unknown.
|
|
|
A recent rigorous echocardiographic study indicated that MVP occurs in about _____% of the population and is more common among _________ (men/women), especially those with ______, ______ bodies.
|
2%; women; thin; lean
|
|
|
A person with mitral valve prolapse may have a comorbid conditions involving another organ. What is it?
|
Adult polycystic kidney disease
|
|
|
Mitral valve prolapse may be seen in these connective tissue diseases.
|
Marfan's or Ehler's danlos
|
|
|
You auscultate a patient with polycystic kidney disease. What might you expect to hear on auscultation?
|
A midsystolic "click", like opening a parachute. May have some regurgitation murmur.
|
|
|
Mitral valve prolapse is usually ____________, however in some cases it may lead to ________________.
|
asymptomatic; sudden death
|
|
|
Complications of mitral valve prolapse?
|
They are rare.
(1) Infectious endocarditis (dmg valve over time) (2) Arrhythmia (3) Severe mitral regurgitation |
|
|
Treatment of mitral valve prolapse?
|
Valve replacement
|
|
What is this? We're looking from the atrium.
|
Mitral valve prolapse.
|
|
|
Mitral regurgitation usually arises as a complication of ______.
|
MVP
|
|
|
Except for MVP, what other causes of mitral regurgitation are there?
|
(1) LV dilation
(2) Infective endocarditis (dmges valve leaflets) (3) ARF (4) Papillary muscle rupture after MI |
|
|
How does mitral regurgitation sound like on auscultation?
|
Holosystolic and "blowing"
|
|
|
A patient with known infective endocarditis has a holosystolic blowing type of murmur. You can barely hear it. How could you make it louder?
|
Tell the patient to squat or expire (increased preload to LV)
|
|
|
Mitral stenosis is usually due to what?
|
Chronic rheumatic valve disease
|
|
|
Acute rheumatic disease creates ____________ and chronic rheumatic disease creates___________.
|
regurgitation; stenosis
|
|
|
What would you hear on auscultation of a patient with mitral stenosis?
|
Opening snap followed by a diastolic rumble
|
|
|
A key complication of mitral stenosis.
|
Volume overload leads to dilation of LA:
(1) Pulmonary congestion with pulmonary HTN (2) Atrial fibrillation (abnormalities of conducting system due to dilation) |
|

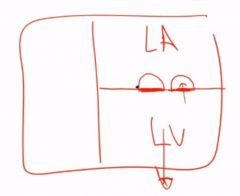
What is this associated with?
|
This is a mural thrombus in LA. Could be due to chronic mitral stenosis with LA dilation.
|