Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
101 Cards in this Set
- Front
- Back
|
Extrinsic causes of joint pain
|
Neurologic (nerve root compression, herpes), generalized (fibromylagia, polymyalgia, sickle cell), referred pain, and pain originating from surrounding organs
|
|
|
Intrinsic causes of joint pain
|
Articular (arthritis, neoplastic, traumatic), and non-articular such as bursa, tenons, ligaments, muscle
|
|
|
Signs suggesting an open fracture?
|
Continuous bleeding from puncture site or fat droplets in blood
|
|
|
The four X-ray rule of 2s
|
2 sides, 2 views, 2 joints (joint above and below), and 2 times (before and after reduction)
|
|
|
What is the difference between varus and valgus angulation?
|
Varus - apex away from midline; valgus - toward midline
|
|
|
What are the indications for open reduction? Use the mnemonic NO CAST
|
Non-union, Open fracture, Neurovascular Compromise, intra-Articular fracture, Salter-HArris 3,4,5, polyTrauma
|
|
|
Reasons for splinting?
|
Reduces pain and further damage to vessels, nerves, and skin; reduces inadvertently converting closed to open fracture, facilitates patient transport
|
|
|
What is heterotopic ossification?
|
Formation of bone in abnormal locations, such as muscle, secondary to pathology
|
|
|
What is avascular necrosis?
|
Ischemia to bone due to disrupted blood supply; commonly in bones covered by cartilage or with distal to proximal blood supply
|
|
|
Healing of a fracture at 0-3 weeks?
|
Hematoma, macrophages surround fracture site
|
|
|
Healing of a fracture at 3-6 weeks?
|
Osteoclasts remove sharp edges, callus forms within hematoma
|
|
|
Healing of a fracture at 6-12 weeks?
|
Bone forms within the callus, bridging fragments
|
|
|
Healing of a fracture at 6-12 months?
|
Cortical gap is bridged by bone
|
|
|
Healing of a fracture at 1-2 years?
|
Normal architecture is achieved through remodelling
|
|
|
How do you clinically evaluate healing of a fracture?
|
No longer tender to palpation or stressing on physical exam
|
|
|
How do you evaluate the healing of a fracture with x-rays? (what do you look for?)
|
Trabeculae cross fracture site, visible callus bridging site on at least 3 of 4 cortices
|
|
|
Early local fracture complications
|
Compartment syndrome, neurological injury, vascular injury, infection, implant failure, fracture blisters
|
|
|
Early systemic fracture complications
|
Sepsis, DVT, PE, ARDS secondary to fat embolism, hemorrhagic shock
|
|
|
Late local fracture complications
|
Mal/non-union, AVN, osteomyelitis, HO, post-traumatic osteoarthritis, joint stiffness, CRPS type I/RSD
|
|
|
Orthopedic emergencies? Use the mnemonic VON CHOP
|
Vascular compromise, Open fracture, Neurological compromise/cauda equina syndrome, Compartment syndrome, Hip dislocation, Osteomyelitis/septic arthritis, unstable Pelvic fracture
|
|
|
What is Buck's traction?
|
A system of weights, pulleys and ropes that are attached to the end of a patient's bed exerting a longitudinal force on the distal end of a fracture, improving its length, alignment, and rotation
|
|
|
Emergency measures in open fractures
|
Remove obvious foreign material --> irrigate with saline --> cover in sterile dressings --> immediate IV antibiotics --> tetanus or immunoglobulin as needed --> reduce and splint --> NPO and prepare for OR
|
|
|
Most common route of infection in septic joint?
|
Hematogenous
|
|
|
Most common causes of septic joint in adults?
|
Staphylococcus aureus; consider coagulase-negative Staphylococcus in patients with prior joint replacement and Neisseria gonorrhea in sexually active adults
|
|
|
Risk factors for septic joint
|
Age >80, DM, RA, prosthetic joint, recent surgery, skin infects, IVDA, alcoholism
|
|
|
Clinical presentation of septic joint
|
Inability/refusal to bear weight, localized joint pain, erythema, warmth, swelling, pain on active and passive ROM, +/- fever
|
|
|
Investigations done in suspected septic joint
|
X-ray (r/o fracture), ESR, CRP, WBC, blood cultures; joint aspirate, and listen for heart murmur (to r/o endocarditis)
|
|
|
Treatment of septic joint
|
IV antibiotics, empiric therapy, adjust following joint aspirate C&S results; needle aspiration if small, urgent decompression and surgical drainage if large joint
|
|
|
Plain film findings in septic joint
|
0-3 days usually normal; 4-6 days joint space narrowing and destruction of cartilage
|
|
|
Plain film findings of osteomyelitis
|
Soft tissue swelling*, lytic bone destruction*, and periosteal reaction (formation of new bone); *generally not seen until 10-12 days after onset of infection
|
|
|
Most common organisms causing osteomyelitis
|
Staphylococcus aureus; consider Salmonella typhi in sickle cell and Gram negative in neonates and immunocompromised
|
|
|
Most common route of infection for osteomyelitis
|
Hematogenous or exogenous (open fractures, surgery, local infected tissue)
|
|
|
Common sites of osteomyelitis
|
Long bones (children) and vertebra (adults)
|
|
|
Joint aspirate findings in septic joint
|
>80,000 WBCs, protein >4.4, joint << blood Glucose, no crystals and positive Gram stain
|
|
|
Investigations in suspected osteomyelitis
|
Bone biopsy, blood culturem aspirate cultures, ESR; CRP, CBC (leukocytosis; x-ray, bone scan, MRI most sensitive and specific (use for diabetic foot or vertebral involvement)
|
|
|
Treatment of osteomyelitis
|
IV antibiotics, empiric therapy, adjust following blood and aspirate culture results; surgical decortication and drainage +/- local antibiotics if abscess or does not improve after 36 hours on IV antibiotics; worst case amputation
|
|
|
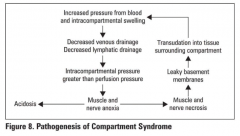
What is compartment syndrome?
|
Increased interstitial pressure in an anatomical compartment (forearm, calf) where muscle and tissue are bounded by fascia and bone with little room for expansion; interstitial pressure exceeds capillary perfusion pressure leading to muscle necrosis (4-6 hours) and eventually nerve necrosis
|
|
|
The etiology of compartment syndrome can be divided into intracompartmental and extracompartmental. What are the intracompartmental causes of compartment syndrome?
|
Fracture (tibial shaft, pediatric supracondylar fractures and forearm), crush injury, and ischemia-reperfusion injury
|
|
|
The etiology of compartment syndrome can be divided into intracompartmental and extracompartmental. What are the extracompartmental causes of compartment syndrome?
|
Constrictive dressing (circumferential cast, poor positioning during surgery), circumferential burn
|
|
|
Pathogenesis of compartment syndrome
|
|
|
|
The 5 P's of compartment syndrome
|
Pain, pallor (late finding), paresthesia, paralysis (late finding), and pulselessness (late finding)
|
|
|
Clinical presenation of compartment syndrome
|
Pain with active contraction of compartment and passive stretch, swollen and tense compartment, suspicious history
|
|
|
Most important sign of compartment syndrome? Symptom?
|
Increased pain with passive stretch; most important symptom is pain out of proportion to injury
|
|
|
Non-operative treatment of compartment syndrome?
|
Remove constrictive dressings (casts, splints), elevate limb at the level of the heart
|
|
|
Operative treatment of compartment syndrome
|
Urgen fasciotomy; 48-72 hours post-op - wound closure +/- necrotic tissue debridement
|
|
|
Investigations in compartment syndrome
|
Usually not necessary as it's a clinical diagnosis; measure compartment with catheter after clinical diagnosis is made
|
|
|
Complications of compartment syndrome
|
Rhabdomyolysis, renal failyre secondary to myoglobinuria, Volkmann's ischemic contracture
|
|
|
Etiology of cauda equina syndrome?
|
Compression or irritation of lumbosacral nerve roots below L2; decreased space in the vertebral canal below L2; common causes - herniated disk +/- spinal stenosis, vertebral fracture and tumor
|
|
|
Clinical features of cauda equina syndrome
|
Acute, motor (LMN signs), autonomic signs (urinary and fecal incontinence), sensory - low back pain radiating to legs, bilateral sensory loss or pain, saddle anesthesia, sexual dysfunction
|
|
|
Treatment of cauda equina syndrome
|
urgen investigation and decompression (<48 hours) to preserve bowel, bladder and sexual function and to prevent progression to paraplegia
|
|
|
Prognosis of cauda equina syndrome
|
Improved markedly with surgical decompression; recovery correlates with function at initial presentation: if unable to walk, unlikely to walk after surgery
|
|
|
What is thoracic outlet syndrome?
|
Impingement of subclavian vessels and brachial plexus nerve trunk
|
|
|
Etiologies of thoracic outlet syndrome
|
Congenital - cervical rib, trauma, degenerative - osteoporosis, arthritis
|
|
|
Clinical features of thoracic outlet?
|
Neurogenic (ulnar and median nerve motor and sensory), arterial (fatigue, weakness, coldness, ischemic pain, paresthesia), venous (edema, venous distention, collateral formation, cyanosis)
|
|
|
Treatment of thoracic outlet syndrome
|
Conservative - physiotherapy, posture and behaviour modification, surgical - removal of first or cervical rib
|
|
|
Mechanism of anterior hip dislocation
|
Posteriorly directed blow to knee with hip widely abducted
|
|
|
Management of hip dislocation
|
Examine for neurovascular injury --> reduce hip dislocation ASAP (<6h) to decrease risk of AVN of the femoral head -> hip reduction for 6 weeks post-reduction
|
|
|
Clinical features of anterior hip dislocation
|
Shortened, abducted, externally rotated limb
|
|
|
Treatment of anterior hip dislocation
|
Closed reduction under conscious sedation/GA, post-reduction CT to assess joint congruity
|
|
|
Mechanism of posterior hip dislocation
|
Severe force to knee with hip flexed and adducted; e.g., knee into dashboard in a motor vehicle collision (MVC)
|
|
|
Clinical features of posterior hip dislocation
|
Shortened, adducted and internally rotated limb
|
|
|
Treatment of a posteriorly dislocated hip
|
Closed reduction under conscious sedation/GA only if associated femoral neck fracture; ORIF if unstable, intra-articular fragments or posterior wall fracture; post-reduction CT to assess joint congruity and fractures; if reduction is unstable, put in traction for 4-6 weeks
|
|
|
Most common type of hip dislocation
|
Posterior
|
|
|
Mechanism of central hip dislocation
|
Traumatic injury where femoral head is pushed medially through acetabulum
|
|
|
Possible complications of all hip dislocations
|
Post-traumatic osteoarthritis, AVN, fracture of femoral head, neck, or shaft; sciatic nerve palsy in 25% (10% permanent), HO, thromboembolism - DVT/PE
|
|
|
What are the four joints in the shoulder?
|
Glenohumeral, acromioclavicular (AC), sternoclavicular (SC), and scapulothoracic
|
|
|
Factors causing shoulder instability
|
Shallow glenoid, loose capsule, ligamentous laxity
|
|
|
Shoulder passive ROM
|
Abduction - 180; adduction - 45; flexion - 180; extension - 45; internal rotation - level of T4; external rotation - 40-45
|
|
|
Describe the Rochester method to reduce dislocations
|
Patient lies supine with hip and knee flexed on injured side; surgeon stands on patient's injured side; surgeon passes one arm under patient's flexed knee, reaching to place that hand on patient's other knee; with other hand, surgeon grasps patient's ankle on injured side, applying traction, while assistant stabilizes pelvis; reduction via traction, internal rotation, then external rotation once femoral head clears acetabular rim
|
|
|
What is the most commonly dislocated joint in the body?
|
The glenohumeral joint, since stability is sacrificed for motion
|
|
|
Prognosis of shoulder dislocation
|
Recurrence rate depends on age of first dislocation: <20 - 65-95%; 20-40: 60-70%; >40: 2-4%
|
|
|
Specific complications of shoulder dislocation
|
Rotator cuff or capsular tear, shoulder stiffness; injury to axillary nerve/artery, brachial plexus; recurrent/unreducted dislocation (most common complication)
|
|
|
Mechanism of anterior shoulder dislocation
|
Abducted arm is externally rotated/hyperextended, or blow to posterior should; involuntary, usually traumatic; voluntary, atraumatic
|
|
|
Symptoms of anterior shoulder joint dislocation
|
Pain, arm slightly abducted and external rotated with inability to internally rotate
|
|
|
Findings on shoulder exam in anterior shoulder dislocation
|
"Squared off" shoulder, positive apprehension tests, positive relocation test, positive sulcus sign
|
|
|
What is considered a positive apprehension test?
|
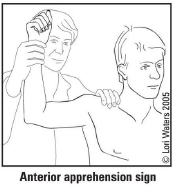
Patient looks apprehensive with gentle shoulder abduction and external rotation to 90 degrees since humeral head is pushed anteriorly and recreates feelings of anterior dislocation
|
|
|
What is considered a positive relocation test?
|
A posteriorly directed force applied during the apprehension test relieves apprehension since anterior sublluxation is prevented
|
|
|
What is considered a positive sulcus sign?
|
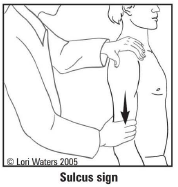
Presence of subacromial indentation with distal traction on humerus indicates inferior shoulder instability
|
|
|
Investigations in suspected anterior shoulder dislocation
|
X-rays: AP, trans-scapular, and axillary views
|
|
|
Radiographic findings in anterior shoulder dislocation
|
Axillary view: humeral head is anterior; trans-scapular/scapular Y view: humeral head is anterior to the centre of the "Mercedez-Benz sign"
|
|
|
What is a Hill-Sachs lesion?
|
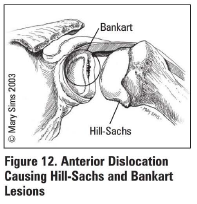
Compression fracture of posterior humeral head due to forceful impaction of an anteriorly dislocated humeral head against the glenoid rim
|
|
|
Treatment of anterior shoulder dislocation
|
Closed reduction with IV sedation and muscle relaxation; obtain post-reduction x-rays; check post-reduction NVS; sling for 3 weeks (avoid abduction and external rotation), followed by shoulder rehabilitation (dynamic stabilizer strengthening)
|
|
|
Mechanism of posterior shoulder dislocation (5%)
|
Adducted, internally rotated, flexed arm; FOOSH; 3 E's (epileptic seizure, EtOH, electrocution); blow to anterior shoulder
|
|
|
Clinical features of a posterior shoulder dislocation
|
Arm is held in adduction and internal rotation; external rotation is blocked; anterior shoulder flattening, prominent coracoid, palpable mass posterior to shoulder; posterior apprehension ("jerk") test
|
|
|
What is posterior apprehension test?
|
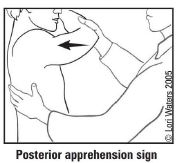
With patient supine, flex elbow 90 degrees and adduct, internally rotate the arm while applying a posterior force to the shoulder; patient will "jerk" back with the sensation of subluxation
|
|
|
Investigations in suspected posterior shoulder dislocation
|
X-rays: AP, trans-scapular, axillary
|
|
|
AP x-ray findings on posterior shoulder dislocation
|
Partial vacancy of glenoid fossa and >6mm space between anterior glenoid rim and humeral head (positive rim sign), humeral head may resemble a lightbulb due to internal rotation (lightbulb sign)
|
|
|
Axillary x-ray findings on posterior shoulder dislocation
|
Humeral head is posterior
|
|
|
Trans-scapular view findings on x-ray in posterior shoulder dislocation
|
Humeral head is posterior to centre of "Mercedez-Benz sign"
|
|
|
Other x-ray findings in posterior shoulder location
|
Reverse Hill-Sachs lesion (75% of cases): divot in anterior humeral head; reverse bony Bankar lesion: avulsion of the posterior glenoid labrum from the bony glenoid
|
|
|
Treatment of posterior shoulder dislocation
|
Closed reduction, obtain post-reduction x-rays, check post-reduction neurovascular status, sling in abduction and external rotation for 3 weeks, followed by shoulder rehablitation
|
|
|
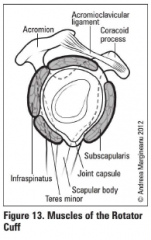
Muscles of the rotator cuff
|
SITS: Supraspinatus, Infraspinatus, Teres minor, Subscapularis
|
|
|
How do you screen out rotator cuff tears?
|
No night pain (SN 87.7%); No painful arc (SN 97.5%); No impingement signs (SN 97.2%); no weakness
|
|
|
Describe the traction-countertraction method of reducing a shoulder dislocation
|
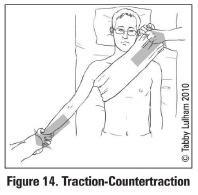
Assistant stabilizes torso with a folded sheet wrapped across the chest while the surgeon applies gentle steady traction
|
|
|
Describe the Stimson method of reducing a shoulder dislocation
|
While patient lies prone with arm hanging over table edge, hand a 5lb (2.3kg) weight on wrist for 15-20 minutes
|
|
|
Describe the Hippocratic method of reducing shoulder dislocations
|
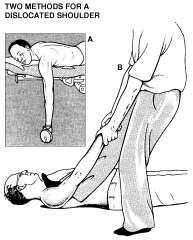
Place heel into patient's axilla and apply traction to arm; perhaps the safest method of shoulder reduction
|
|
|
Nerve root of biceps reflex
|
C5/C6
|
|
|
Nerve root of the brachioradialis reflex
|
C6
|
|
|
Nerve root of the triceps reflex
|
C7/C8
|
|
|
Nerve root of the patellar reflex
|
L2-L4
|
|
|
Nerve root of the ankle jerk reflex
|
S1/S2
|