Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
85 Cards in this Set
- Front
- Back
|
Ball and socket joint
|
Notable for its strength, stability, and wide range of motion.
Stability of the hip joint arises from: - Deep fit of head of the femur into acetabulum - Strong fibrous articular capsule - Muscles crossing the joint |
|
|
Bones/joints of the pelvis
|
femur
acetabulum ilium ischium symphysis pubis |
|
|
Anterior hip landmarks
|
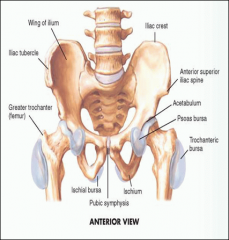
Iliac crest at level of L4
Iliac tubercle anterior superior iliac spine (ASIS) greater trochanter pubic symphysis |
|
|
Posterior hip landmarks
|
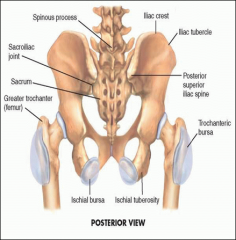
Posterior Superior Iliac Spine (line across to S2)
Greater trochanter Ischial tuberosity Sacroiliac joint |
|
|
Muscle groups in the hip
|
Flexor group (anterior) - Iliopsoas
Extensor group (posterior) - gluteus maximus Adductor group (medial) - swings thigh to body Abductor group (lateral) - gluteus medius and minimus, moves the thigh away from the body |
|
|
Additional hip structures
|
Bursae – psoas, trochanteric, and ischial
|
|
|
Hip exam: gait
|
Width of base – should be 2-4” from heel to heel
- Wide base in cerebellar disease or foot problems - Shift of the pelvis - Hip dislocation , arthritis, or abductor weakness can produce waddle - Flexion of the knee |
|
|
Gait stance/swing
|
Stance - foot is on the ground and bears weight
- 60% of the walking cycle Swing - foot moves forward and does not bear weight - 40% of the cycle |
|
|
Lumbar spine inspection
|
Loss of lumbar lordosis in paravertebral spasm
Excess lordosis in flexion deformity of the hip |
|
|
Leg length symmetry
|
Changes seen in abduction or adduction deformities and scoliosis
External rotation of the hip and shortening of leg suggest hip fracture |
|
|
Palpate inguinal structures
|
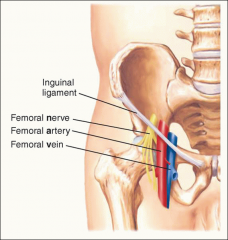
With the patient supine, ask the patient to place the heel of the leg being examined on the opposite knee.
Palpate along the inguinal ligament - Femoral nerve, artery, and vein (NAVEL) bisect the overlying inguinal ligament; lymph nodes lie medially. |
|
|
Inguinal abnormalities
|
Bulges along ligament
- May be inguinal hernia or aneurysm Enlarged lymph nodes - Suggest lower extremity infection |
|
|
How to palpate trochanteric and ischiogluteal bursae in hip
|
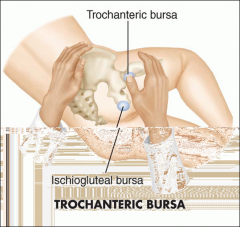
With the patient resting on one side and the hip flexed and internally rotated, palpate T. bursae
- Focal tenderness over the trochanter indicates trochanteric bursitis. |
|
|
Flexion of the hip
|
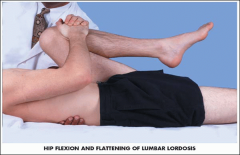
With the patient supine, place your hand under the patient's lumbar spine.
Bend each knee in turn up to the chest and pull it firmly against the abdomen. - Note that the hip can flex further when the knee is flexed. When the back touches your hand, indicating normal flattening of the lumbar lordosis—further flexion must arise from the hip joint itself - Note whether the opposite thigh remains fully extended, resting on the table. |
|
|
Extension of the hip
|

Lie face down, then bend your knee and lift it up.
With the patient lying face down, extend the thigh toward you in a posterior direction. Alternatively, carefully position the supine patient near the edge of the table and extend the leg posteriorly |
|
|
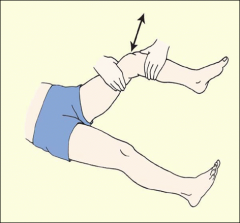
Abduction of the hip
|

Stabilize the pelvis by pressing down on the opposite anterior superior iliac spine with one hand.
With the other hand, grasp the ankle and abduct the extended leg until you feel the iliac spine move. This movement marks the limit of hip abduction. |
|
|
Adduction of the hip
|

With the patient supine, stabilize the pelvis, hold one ankle, and move the leg medially across the body and over the opposite extremity.
|
|
|
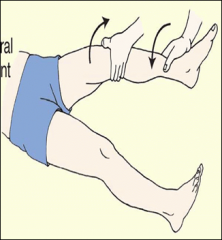
Internal and external rotation of the hip
|
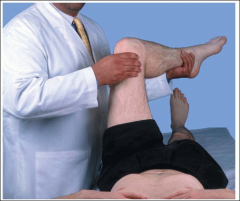
Flex the leg to 90° at hip and knee, stabilize the thigh with one hand, grasp the ankle with the other, and swing the lower leg.
Medially for external rotation at the hip and laterally for internal rotation. It is the motion of the head of the femur in the acetabulum that identifies these movements. |
|
|
Hip fractures
|
More common in the elderly
Present with hip, knee, or back pain Leg is externally rotated and appears shorter |
|
|
Hip fracture types
|
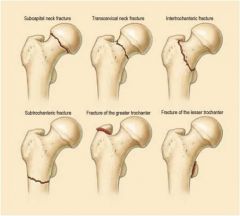
Femoral neck
Intertrochanteric Subcapital Subtrochanteric Greater and lesser trochanteric fractures |
|
|
Legg Calve Perthes
|
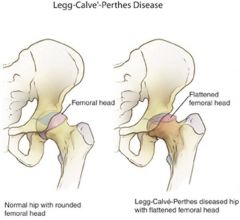
A childhood disorder of the hip due to alteration in blood flow to the femoral head resulting in avascular necrosis.
Symptoms - Hip or knee pain - Limping or antalgic gait - Reduced range of motion of the hip |
|
|
Slipped Capital Femoral Epiphysis
|

Fracture through the growth plate and slippage of the epiphysis
Often in overweight children Symptom/signs: thigh, groin, or knee pain. Decreased internal rotation and abduction. As hip is flexed it rolls into external rotation and abduction |
|
|
Knee
|
Largest joint in the body
Articulating bones - femur, tibia, patella Stability dependent on ligaments |
|
|
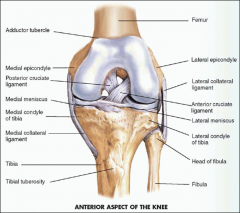
Bony landmarks of the knee
|
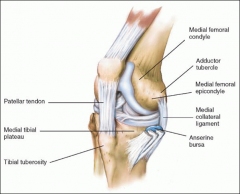
Medial - adductor tubercle, medial epicondyle, and medial condyle of tibia
Anterior - patella, patellar tendon, tibial tuberosity Lateral - lateral epicondyle, lateral condyle of tibia |
|
|
Condylar tibiofemoral joints
|
Formed by the convex curves of the medial and lateral condyles of the femur as they articulate with the concave condyles of the tibia.
|
|
|
Patellofemoral joint
|
Slides on the groove of the anterior aspect of the distal femur, called the trochlear groove, during flexion and extension of the knee.
|
|
|
Muscle groups of the knee
|
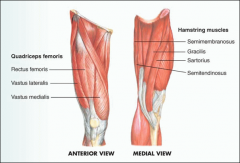
Quadriceps femoris - extends the leg
Hamstring muscles - flex the knee |
|
|
Meniscus
|
Medial and lateral
- Crescent shaped fibrocartilagionous discs cushion the action of the femur on the tibia |
|
|
Knee ligaments
|
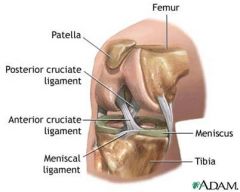
Medial Collateral
Lateral Collateral Anterior Cruciate Posterior Cruciate |
|
|
Synovial cavity of the knee
|
Concavities anteriorly, medially, and laterally
Synovium is not normally detectable, these areas may become swollen and tender when joint is inflamed |
|
|
Suprapatellar pouch
|
Synovial cavity lying 6cm above the upper boarder of the patella, lying upward and deep to the quadriceps muscles.
|
|
|
Bursa
|
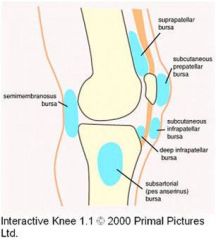
Prepatellar
Anserine Semimembranosus |
|
|
Knee exam: Gait
|
Look for smooth, rhythmic flow as the patient enters the room.
Knee should be extended at heel strike and flexed at all other phases of swing and stance. |
|
|
Knee inspection
|
Alignment and contours of the knees
Atrophy of the quadriceps muscles - Bowlegs (genu varum) - Knock-knees (genu valgum) Loss of the normal hollows around patella, sign of swelling in knee joint and suprapatellar pouch Note any swelling, scars or lesions around knee. |
|
|
Prepatellar bursitis
|

Swelling over the patella
Housemaid's knee, caused by excessive kneeling |
|
|
Infrapatellar bursitis
|
Swelling over the tibial tubercle
|
|
|
Palpate
|
Ask the patient to sit on the edge of the exam table to make bony landmarks more visible.
- Tibiofemoral joint - Medial meniscus (slight internal rotation) - Lateral meniscus (slight flexion) - Medial compartment - medial to patellar tendon (flexed at 90 degree) - Lateral compartment- - lateral to patellar tendon - Patellofemoral compartment - Suprapatellar pouch and bursa - Gastrocnemius and soleus |
|
|
Medial compartment of knee
|
1. Medial femoral condyle
2. Adductor tubercle 3. Medial tibial plateau 4. Medial collateral ligament (MCL) |
|
|
Lateral compartment of knee
|
1. Lateral femoral condyle
2. Lateral tibial plateau 3. Lateral collateral ligament (LCL) (ask to cross legs) |
|
|
Patellofemoral compartment of knee
|
Patella and patella tendon to tibial tuberosity
- extend knee for intact tendon |
|
|
Patellar grind test
|

With the patient supine and the knee extended, compress the patella against the underlying femur.
Ask the patient to tighten the quadriceps as the patella moves distally in the trochlear groove. Check for a smooth sliding motion - Grinding or pain is abnormal Pain may indicate: - chondromalcia patella - arthritis - patellofemoral syndrome |
|
|
Suprapatellar pouch and bursa palpation
|
Palpate any thickening or swelling in the suprapatellar pouch
- Start 10 cm above superior border of patella, well above pouch, and feel soft tissues between thumb and fingers. - Move your hand distally in progressive steps, trying to identify pouch. - Continue palpation along the sides of patella. - Note any tenderness or warmth greater than in the surrounding tissues. Thickening, bogginess, or warmth suggests: - synovitis or effusion Palpate prepatellar, anserine and popliteal bursae. |
|
|
Anserine bursitis (medial)
|
Caused by running, valgus knee deformity, fibromyalgia, osteoarthritsis.
|
|
|
Popliteal cysts (baker's cyst)
|
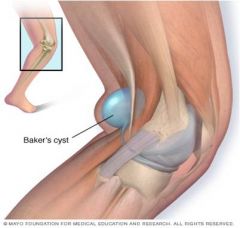
Caused by distension of the gastrocnemius semimembranous bursa.
|
|
|
Bulge sign (minor effusions)
|

With knee extended, place the left hand above knee and apply pressure on suprapatellar pouch, displacing or “milking” fluid downward.
Stroke downward on the medial aspect, apply pressure to force fluid into the lateral area. Tap the knee just behind the lateral margin of the patella with right hand. Positive - fluid wave or bulge on the medial side, consistent with effusion. |
|
|
Balloon sign (major effusions)
|

Place thumb and index finger of right hand on each side of the patella
- With left hand, compress the suprapatellar pouch against the femur. Feel for fluid entering (or ballooning into) the spaces next to the patella under your right thumb and index finger. |
|
|
Balloting the patella (major effusions)
|
Compress the suprapatellar pouch and “ballotte” or push the patella sharply against the femur. Watch for fluid returning to the suprapatellar pouch.
|
|
|
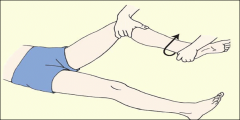
Thompson test
|
Place patient prone with knee and ankle flexed at 90°, or alternatively, ask patient to kneel on a chair.
Squeeze calf and watch for plantar flexion at ankle. Absence of plantar flexion = positive test - Indicates Achilles rupture |
|
|
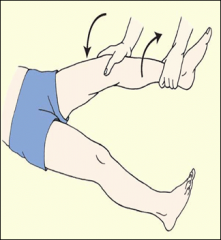
Knee flexion
|
Hamstring group
- biceps femoris, semitendinosus, and semimembranosus Bend or flex your knee or squat down to the floor |
|
|
Knee extension
|
Quadriceps
- rectus femoris, vastus medialis, lateralis, and intermedius Straighten your leg or after you squat down to the floor, stand up. |
|
|
Knee internal rotation
|
Sartorius, gracilis, semitendinosus, semimembranosus
While sitting, swing your lower leg toward the midline. |
|
|
Knee external rotation
|
Biceps femoris
While sitting, swing your lower leg away from the midline. |
|
|
McMurray test (medial and lateral meniscus)
|
With patient supine, grasp heel and flex knee.
Cup other hand over knee joint with fingers and thumb along medial and lateral joint line. From the heel, rotate lower leg internally and externally. Then push on lateral side to apply a valgus stress on medial joint. At the same time, rotate the leg externally and slowly extend it. Positive - click or pop along medial joint With valgus stress, external rotation, and leg extension, suggests tear of the posterior portion of the medial meniscus. With nternal rotation, varus stress, and extension, suggests tear of lateral meniscus. |
|
|
Abduction or valgus stress test
|
With patient supine and knee slightly flexed, move the thigh about 30° laterally to side of table. Place one hand against lateral knee to stabilize femur and other hand around medial ankle.
Push medially against knee and pull laterally at ankle to open knee joint on medial side - Valgus stress Pain or gap in medial joint line points to ligamentous laxity and a partial tear of the medial collateral ligament (MCL). |
|
|
Adduction or varus stress test
|
With patient supine and knee slightly flexed, move the thigh about 30° laterally to side of table. Place one hand against the medial surface of the knee and the other around the lateral ankle.
Pull laterally against the knee and push medially at the ankle to open the knee joint on the lateral side. - Varus stress Pain or a gap in the lateral joint line points to ligamentous laxity and a partial tear of the lateral collateral ligament (LCL). |
|
|
Anterior drawer test
|
With patient supine, hips flexed and knees flexed to 90° and feet flat on the table, cup your hands around the knee with the thumbs on the medial and lateral joint line and the fingers on the medial and lateral insertions of the hamstrings.
Draw the tibia forward and observe if it slides forward (like a drawer) from under the femur. Compare the degree of forward movement with that of the opposite knee. Positive - forward jerk showing the contours of the upper tibia is a positive anterior drawer sign. ACL tear 11.5 times more likely |
|
|
Lachman test
|
Place the knee in 15° of flexion and external rotation. Grasp distal femur with one hand and upper tibia with the other. With the thumb of the tibial hand on the joint line, simultaneously move the tibia forward and the femur back.
Estimate the degree of forward excursion Positive - significant forward excursion ACL tear 17.0 times more likely |
|
|
Posterior drawer test
|
With patient supine, hips flexed and knees flexed to 90° and feet flat on the table. Push the tibia posteriorly and observe the degree of backward movement in the femur.
Positive - movement of tibia posteriorly on femur significantly expressing the femoral condyles. Isolated PCL tears are rare |
|
|
Ankle bones
|
Tibia
Fibula Talus - Tibia and fibula act as a mortis for the talus |
|
|
Ankle joints
|
- Tibiotalar joint
- Subtalar (talocalcaneal) joint - Metatarsophalangeal joints - Proximal and distal interphalangeal joints of toes |
|
|
Ankle bony landmarks
|
Medial malleolus
Lateral malleolus Calcaneus |
|
|
Ankle muscle groups
|
Plantar flexors
- Gastrocnemius, posterior tibialis, and the toe flexors (tendons run behind malleoli) Dorsiflexors - Anterior tibial muscle and the toe extensors (on anterior or dorsum of the foot) |
|
|
Ankle ligaments
|
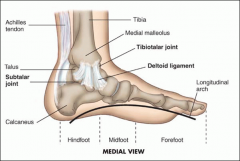
Medially
- Deltoid ligament medial malleolus to talus and proximal tarsal bones Laterally - Anterior talofibular ligament --- most at risk with inversion injury) - Calcaneofibular ligament - Posterior talofibular ligament |
|
|
Ankle/foot inspection
|
All surfaces of the ankles and feet, noting any deformities, nodules, swelling, calluses, or corns
|
|
|
Ankle/foot palpation
|
With thumbs, palpate anterior ankle joint.
- Note for bogginess, edema, or tenderness. Achilles tendon for nodules and tenderness Heel – posterior/inferior calcaneus and plantar fascia Medial and lateral malleolus Metatarsophalangeal joints Heads of the 5 metatarsals and grooves in between |
|
|
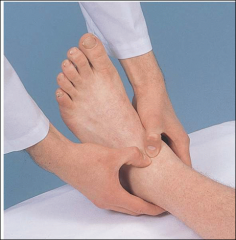
Heel palpation
|
Bone spurs - may present on calcaneus
Plantar fasciitis - focal pain on palpation of the fascia, seen in prolonged standing or hell-strike exercise - inserts on medial calcaneal tubercle |
|
|
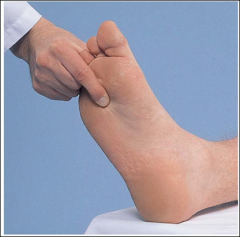
Palpating the metatarsophalangeal joints
|

Compress the forefoot
- tenderness is an early sign of RA |
|
|
Metatarsalgia
|
Pain between metatarsals and grooves in between.
- Found in trauma, arthritis, or vascular compromise |
|
|
Ankle flexion
|
Plantar flexion
- gastrocnemius, soleus, plantaris, tibialis posterior Point your foot toward the floor. |
|
|
Ankle extension
|
Dorsiflexion
- tibialis anterior, extensor digitorum longus, and extensor hallucis longus Point your foot toward the ceiling. |
|
|
Ankle inversion
|
Tibialis posterior and anterior
Bend your heel inward. |
|
|
Ankle eversion
|
Peroneus longus and brevis
Bend your heel outward. |
|
|
Ankle ROM
|
Dorsiflex and plantar flex the foot at the ankle
|
|
|
Subtalar joint ROM
|
Stabilize the ankle with one hand and invert/evert foot.
|
|
|
ROM of the foot
|

Transverse tarsal joint
- stabilize the heel and invert/evert the forefoot Metatarsophalangeal joint - flex the toes in relation to the feet |
|
|
Measuring leg lengths
|
If abnormalities suspected, measure the distance between the anterior superior iliac spine and the medial malleolus.
|
|
|
Acute gouty arthritis
|

Podagra
- metatarsophalangeal joint of the great toe may be the first joint invovled. Very painful, erythematous, hot, and tender - Can be mistaken for septic arthritis. - Look at risk factors for gout - Disease of kings-lots of alcohol and red meat |
|
|
Flat feet (pes plantus)
|

Longitudinal arch flattens so the sole approaches or touches the floor.
- Tenderness may be present from the medial malleolus down along the medial-plantar surface of the foot. - Swelling develops anterior to the medial malleolus |
|
|
Hallux valgus (bunion)
|
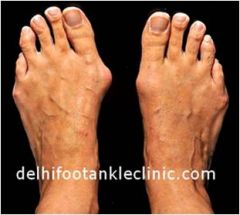
Great toe is abnormally abducted in relationship to the first metatarsal, which itself is deviated medially.
Head of metatarsal may enlarge and from a bursae. Pain and edema, with deformity |
|
|
Morton's neuroma
|
Entrapment of medial and lateral plantar nerves
Symptoms Hyperesthesia, numbness, aching, and burning from the metatarsal heads into 3rd and 4th toes Tenderness over plantar surface 3rd and 4th metatarsal heads |
|
|
Hammer toe
|
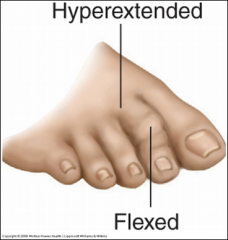
Hyperextension at the MTP joint with flexion at the PIP (usually 2nd toe)
|
|
|
Corn
|
Painful conical thickening of skin from recurrent pressure (usually 5th toe).
Cauliflower look when you scrape corns |
|
|
Plantar wart
|

Wart on the sole of the foot.
Painful due to pressure on underlying structures. |
|
|
Neuropathic ulcer
|

Diminished sensation or absent, as in DM neuropathy, neuropathic ulcers develop at pressure points
|
|
|
Achilles rupture
|
Sudden severe pain “like a gunshot”
Ecchymosis from the calf into the hell Flat-footed gait with absence of “toe-off” More common in middle aged men |