Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
90 Cards in this Set
- Front
- Back
|
Low back pain red flags
|
- Over age 50
- History of cancer - Weight loss - Pain at night or increased by rest - History of IV drug use - Presence of infection/fever |
|
|
Lupus (SLE)
|
Presents with back pain and butterfly rash
|
|
|
Psoriasis
|
Presents with back pain, scaly rash on flexor surfaces and nail pitting
|
|
|
Lyme disease
|
Presents with back pain and an expanding erythematous patch in an early febrile patient.
|
|
|
Reiter’s syndrome
|
Presents with back pain and conjunctivitis with urethritis.
|
|
|
Acute rheumatic fever
|
Presents with back pain preceding sore throat.
|
|
|
Ulcerative colitis or scleroderma
|
Presents with back pain, diarrhea and abdominal pain.
|
|
|
What is the most active joint in the body?
|
Temporal Mandibular Joint (TMJ)
|
|
|
What muscles, nerves and actions involve the TMJ?
|
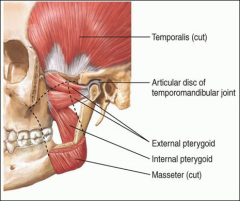
Opening the mouth - external pterygoids.
Closing the mouth - masseter, temporalis, internal pterygoids Innervated by CN V (trigeminal nerve) |
|
|
What muscles comprise the rotator cuff (scapulohumeral) group?
|
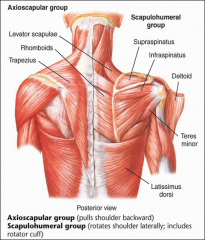
Supraspinatus
Infraspinatus Teres minor Subscapularis Action - rotates shoulder laterally |
|
|
What muscles consist of the axioscapular group?
|
Trapezius
Rhomboids Serratus anterior Levator scapulae Action - pulls shoulder back |
|
|
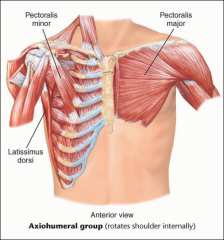
What muscles consist of the sciohumeral group?
|
Pectoralis major
Pectoralis minor Latissimus dorsi Action - rotates shoulder internally |
|
|
Flexion of the shoulder joint involves what muscles?
|
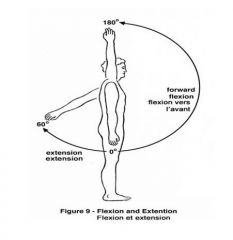
- anterior deltoid
- pectoralis major - biceps brachii - coracobrachialis |
|
|
Extension of the shoulder joint involves what muscles?
|
- latissimus dorsi
- teres major - posterior deltoid - triceps brachii |
|
|
ABduction of the shoulder joint involves what muscles?
|
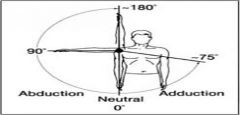
- supraspinatus (testable with open can test)
- middle deltoid - serratus anterior |
|
|
ADduction of the shoulder joint involves what muscles?
|
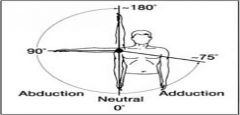
- pectoralis major
- coracobrachialis - latissimus dorsi - teres major - subscapularis Crossover sign test AC joint stability. |
|
|
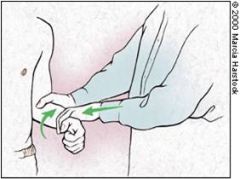
Internal rotation of the shoulder joint involves what muscles?
|
- subscapularis (test w/ lift off test)
- anterior deltoid - pectoralis major - teres major - latissimus dorsi Examine by having patient but hand behind back. |
|
|
External rotation of the shoulder joint involves what muscles?
|
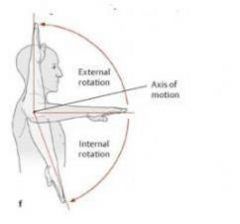
- infraspinatus (testable with isolation)
- teres minor - posterior deltoid Examine by having patient but hand behind head. |
|
|
What tests indicate shoulder impingement?
|
Neer's and Hawkin's sign
|
|
|
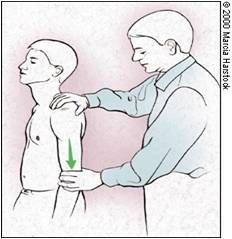
Neer’s sign
|
Press on scapula with one hand to prevent motion, raise the arm with the other hand.
Pain with movement = positive sign |
|
|
Hawkin’s sign
|
Flex shoulder/elbow to 90 degree with palm down. Place one hand on arm and one on forearm, rotate the arm internally.
Pain with movement = positive sign |
|
|
What tests evaluate the rotator cuff?
|
Empty can test - supraspinatus strength
Drop arm - supraspinatus strength Lift off - subscapularis Internal rotation - infraspinatus |
|
|
What tests evaluate the biceps tendon?
|
Yergason’s test - forearm supination
Speed’s test - forearm supination |
|
|
Yergason’s Test
|
Forearm supination
- Flex the elbow to 90 degree, and pronate hand - Provide resistance as patient supinates the hand Pain and clicking = positive biceps tendon injury |
|
|
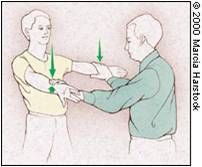
Speed’s Test
|

Forearm supination
- Flex shoulder to 90 degrees with supination at wrist - Examiner resists flexion Pain on movement = positive sign |
|
|
Crossover test
|
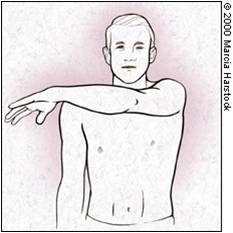
Adduct the arm across the chest
Pain/decreased ROM indicates: - Inflammation of the AC joint - AC joint instability |
|
|
Sulcus sign
|
- Relax arm at side and grasp forearm
- Apply downward force while observing joint Sulcus seen = positive - Indicates glenohumeral (GH) joint instability |
|
|
Apprehension test
|
- Abduct the shoulder to 90 degree
- Externally rotate arm Pain or patient apprehension = positive - Indicates anterior joint instability |
|
|
Calcific tendinitis
|
Degenerative process in the tendon associated with the deposition of calcium salts.
Usually involves supraspinatus tendon Acute, disabling attacks of shoulder pain may occur, usually in patients > age 30, more often in women. |
|
|
Biceps tendonitis
|
Inflammation of the long head of the biceps tendon and tendon sheath causes anterior shoulder pain resembling and often coexisting with rotator cuff tendinitis.
S/S - tenderness is maximal in the bicipital groove. Externally rotate and abduct the arm to separate this area from the subacromial tenderness of supraspinatus tendinitis. Positive Yergason's test |
|
|
Adhesive capsulitis
|
Fibrosis of the glenohumeral joint capsule (frozen shoulder)
S/S - diffuse, dull, aching pain in the shoulder PE - progressive restriction of active and passive range of motion, usually no localized tenderness Usually unilateral, occurs in ages 50-70 |
|
|
Anterior dislocation physical findings
|
- Postive apprehension sign
- Rounded lateral aspect of the shoulder appears flattened - Deformity with pain - Patient holds arm in neutral position |
|
|
Medial epicondylitis
|
Pitcher’s elbow
Follows repetitive wrist flexion, as in throwing Wrist flexion against resistance increases the pain |
|
|
Lateral epicondylitis
|
Tennis elbow
Follows repetitive extension of the wrist or pronation-supination of the forearm. When the patient tries to extend the wrist against resistance, pain increases. |
|
|
Olecranon Bursitis
|

Swelling and inflammation of the olecranon bursa
May result from trauma or may be associated with rheumatoid or gouty arthritis. Superficial to olecranon process |
|
|
Arthritis of the elbow
|

Synovial inflammation or fluid felt best in the grooves between the olecranon process and the epicondyles on either side.
Palpate for a boggy, soft, or fluctuant swelling and for tenderness. |
|
|
Rheumatoid arthritis/nodules
|
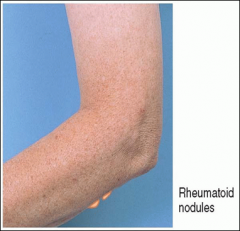
Subcutaneous nodules may develop at pressure points along the extensor surface of the ulna
Firm and nontender, not attached to the overlying skin May occur near olecranon bursa or more distally |
|
|
Thenar eminence
|
Three muscles that compose the thumb and provide flexion, extension and opposition
Atrophy may indicate median nerve compression (carpal tunnel syndrome) |
|
|
What signs of osteoarthritis may be observed in the fingers?
|
Heberden’s nodes at DIP
Bouchard’s nodes at PIP |
|
|
Tinel’s sign
|
Tapping lightly over the course the median nerve
Aching and numbness when tapped = positive - Indicates carpal tunnel syndrome |
|
|
Phalen’s sign
|
Hold the wrists in flexion for 60 seconds
Numbness and tingling in the median nerve distribution = positive - Indicates carpal tunnel syndrome |
|
|
Finkelstein’s test
|
Patient grips their thumb in the palm and ulnar deviates the wrist
Pain = positive Indicates de Quervain's tenosynovitis |
|
|
Acute RA
|
Tender, painful, stiff joints in rheumatoid arthritis, usually with symmetric involvement on both sides of the body.
PIP, MCP, and wrist joints are the most frequently affected. Note the fusiform or spindle-shaped swelling of the PIP joints in acute disease. |
|
|
Ganglion cyst
|
Round, usually nontender swellings along tendon sheaths or joint capsules, frequently at the dorsum of the wrist.
|
|
|
Chronic tophaceous gout
|
Joint involvement is usually not as symmetric as in rheumatoid arthritis.
Acute inflammation may be present. Knobby swellings around the joints ulcerate and discharge white chalklike urates. |
|
|
Trigger finger (type of contracture)
|
Caused by a painless nodule in a flexor tendon in the palm, near the metacarpal head. The nodule is too big to enter easily into the tendon sheath during extension of the fingers from a flexed position.
With extra effort or assistance, the finger extends and flexes with a palpable and audible snap as the nodule pops into the tendon sheath. |
|
|
Neurofibromatosis
|

- Café-au-lait spots (discolored patches of skin)
- Skin tags - Fibrous tumors |
|
|
Spina bifida occulta (least severe)
|
- Birthmarks
- Port-wine stains - Hairy patches - Lipomas often overlie bony defects (possibly unknown to patient) |
|
|
Osteoporosis
|
A progressive bone disease characterized by declining bone mass. Risk factors include:
- Postmenopausal Caucasian women - Age >50 - Weight < 70kg - History of fractures - Family history in 1st degree relative of fractures - Higher intake of alcohol - Delayed menarche or early menopause - Smoker - Low vitamin D - Use of corticosteroids for >2 months |
|
|
Osteoporosis/osteopenia diagnosis
|
Bone density accounts for 70% of bone strength
Measured by Dexascan - Normal T score: -1.0 and above - Osteopenia: between -2.5 and -1.0 - Osteoporosis: less than -2.5 |
|
|
Cauda equina syndrome
|
Low back pain and neurologic dysfunction with urinary retention and overflow incontinence resulting from lesion or tumor of the L1-S5.
Bowel or urinary retention or incontinence. |
|
|
Signs/symptoms of inflammation and arthritis
|
- Swelling
- Warmth - Tenderness - Redness |
|
|
What type of joint is the TMJ?
|
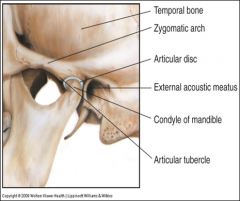
Condylar synovial joint, a fibrocartilaginous disc that cushions the action.
|
|
|
TMJ inspection
|
Look for joint symmetry, alignment, bony deformities, swelling and/or color changes.
|
|
|
TMJ Palpation
|
Palpate joint:
Place tips of index fingers just in front of tragus of each ear and ask patient to open his or her mouth. Fingertips should drop into the joint spaces as the mouth opens. Palpate muscles: Masseters - externally at the angle of the mandible Temporal muscles - externally during clenching and relaxation of the jaw |
|
|
TMJ range of motion (ROM)
|
Grind and hinge motions
- Open/close - normal is 3 fingers can be inserted - Protrusion/retraction (jutting jaw forward) --- bottom teeth can be placed in front of upper - Lateral or side-side motion |
|
|
TMJ Syndrome
|
Typical features are unilateral chronic pain with chewing, jaw clenching, or teeth grinding, often associated with stress, may also present as headache.
|
|
|
TMJ syndrome exam/diagnosis
|
Exam - swelling, tenderness, and decreased range of motion in inflammation
Differential diagnosis - temporal arteritis, trigeminal neuralgia Trauma - dislocation of the TMJ may be seen, palpable crepitus or clicking in poor occlusion, meniscus injury, or synovial swelling from trauma |
|
|
Shoudler girdle
|
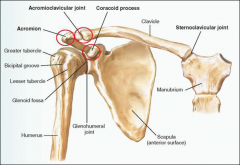
Shoulder derives its mobility from a complex interconnected structure of joints, large bones and principal muscle groups.
|
|
|
What are the major joints of the shoulder?
|
Glenohumeral
Sternoclavicular (SC joint) Acromioclavicular (AC joint) |
|
|
Empty can test
|
Supraspinatus strength
- Flex the arm to 60 degree and internally rotate with thumbs pointing down --- like turning a can upside down and emptying it - Resistance pressure downward Weakness = positive, indicates possible rotator cuff (RTC) tear |
|
|
Drop arm sign
|
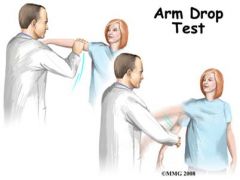
Supraspinatus strength
- Abduct the shoulder to 90 degrees, then slowly lower, move arm up, pt moves arm down Patient cannot lower smoothly = positive, indicates possible RTC tear |
|
|
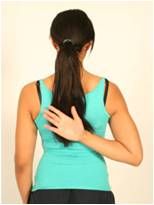
Apley scratch test
|

Overall shoulder rotation
- Ask patient to touch the opposite scapula using two motions - scratching upper and lower back |
|
|
Rotator cuff tendonitis
|
Cause - repeated shoulder motion, as in throwing or swimming.
S/S - can cause edema and hemorrhage followed by inflammation, most commonly involving the supraspinatus tendon. Acute, recurrent, or chronic pain may result, often aggravated by activity. Patients report sharp catches of pain, grating, and weakness when lifting the arm overhead. Physical findings - when the supraspinatus tendon is involved, tenderness is maximal just below the tip of the acromion. Risk factors - patients are typically athletically active. |
|
|
Rotator cuff tear
|
Cause - when arm is raised in forward flexion, rotator cuff may impinge against undersurface of acromion and coracoacromial ligament. Injury from a fall or repeated impingement may weaken the rotator cuff, causing a partial or complete tear, usually after age 40.
S/S - weakness, atrophy of the supraspinatus and infraspinatus muscles, pain, and tenderness may ensue. Physical findings - in a complete tear of the supraspinatus tendon (illustrated), active abduction and forward flexion at the glenohumeral joint are severely impaired, producing a characteristic shrugging of the shoulder and a positive “drop arm” test. |
|
|
Acromioclavicular arthritis
|
Uncommon, usually arising from direct injury to the shoulder girdle with resulting degenerative changes.
S/S - tenderness localized over acromioclavicular joint, glenohumeral joint motion is not painful, but movement of the scapula, as in shoulder shrugging, is painful |
|
|
Anterior dislocation
|
Shoulder instability from anterior dislocation of the humerus usually results from a fall or forceful throwing motion, then becomes recurrent.
Dislocations may also be inferior, posterior (relatively rare), and multidirectional. |
|
|
What muscles are involved in elbow flexion?
|
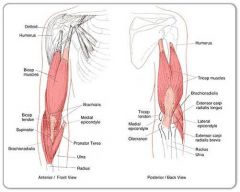
Biceps brachii
Brachialis Brachioradialis |
|
|
What muscles are involved in elbow extension?
|
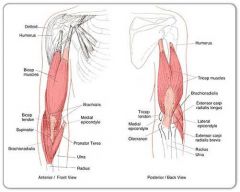
Triceps brachii
Anconeus |
|
|
What muscles are involved in elbow supination?
|
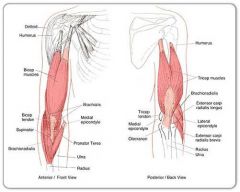
Biceps brachii
Supinator |
|
|
What muscles are involved in elbow pronation?
|
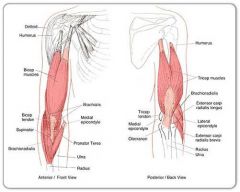
Pronator teres
Pronator quadratus |
|
|
Nursemaid's elbow
|
Radial head subluxation at elbow, annular ligament becomes trapped
Caused by pulling on a extended pronated arm (as in pulling up on a unruly child’s arm) |
|
|
Dupuytren's contractures
|
Thickening of the palmar fascia
Flexion contracture at 3rd, 4th and 5th fingers Skin in this area puckers, and a thickened fibrotic cord develops between palm and finger. Flexion contracture of the fingers may gradually ensue. |
|
|
de Quervain's tenosynovitis
|
Inflammation of the abductor pollicis longus and extensor pollicis brevis tendon and sheath.
Positive Finkelstein's test |
|
|
Hand grip strength
|
Grip examiners 2nd and 3rd fingers
Tests intrinsic muscles of the hand Causes - arthritis, CTS, epicondylitis, cervical radiculopathy |
|
|
How to test finger range of motion
|

Flexion - make a fist
Extension - extend or open the fist Abduction/Adduction - spread fingers apart and back together Thumb ROM - flexion, extension, abduction, adduction, opposition |
|
|
Acute tenosynovitis
|
Infection of the flexor tendon sheaths may follow local injury.
Finger is held in slight flexion; finger extension is very painful. If the infection progresses, it may extend from the tendon sheath into the adjacent fascial spaces within the palm. Early diagnosis and treatment are important. |
|
|
What area of the back is especially vulnerable to injury?
|
L5-S1 due to sharp posterior angle
|
|
|
How common is low back pain?
|
2/3 of adults have LBP at least once
85% have idiopathic back pain |
|
|
Spine inspection
|
- Observe posture
- Assess patient for movements and gait - Observe landmarks - Inspect spinal curves |
|
|
Thoracic kyphosis
|
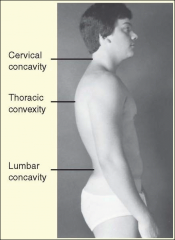
Increased thoracic kyphosis occurs with:
- Aging - Osteoporosis - In children, it is a correctable structural deformity and should be pursued. |
|
|
Spinal landmarks
|
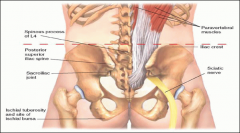
Spinous processes (C7/T1)
Paravertebral muscles Iliac crests - Unequal heights (pelvic tilt) suggests leg length, scoliosis, or abnormality of hips Posterior superior iliac spine (skin dimples) - Line drawn across iliac crests usually marks L4 Shoulder symmetry - Unequal shoulder heights in scoliosis, winging of the scapula, trapezius weakness |
|
|
Spine palpation
|
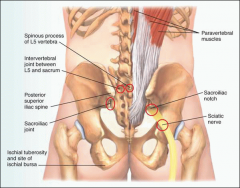
Spinous processes (with thumb) – noting any “step off’s” (slips) of spondylolisthesis (displaced discs) – forward slippage of one vertebrae can compress spinal cord
Cervical facet joints (relaxed neck) Sacroiliac joint – tenderness of SI joint indicates ankylosing spondylitis Paravertebral muscles – not spasm and pain Sciatic nerve – with hip flexed and patient lying on opposite side (L4-S3 nerve roots), tenderness suggests herniated disc Tenderness of spinous processes indicates fracture, infection, arthritis, or dislocation. |
|
|
How to palpate the sciatic nerve
|
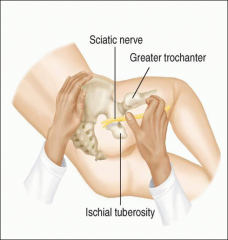
Patient lies on side and flexes hip to opposite side.
The nerve lies midway between the greater trochanter and the ischial tuberosity as it leaves the pelvis through the sciatic notch. Tenderness suggests herniated disc near L4-S3 nerve roots. |
|
|
Neck ROM
|
Flexion and extension (chin down/up)
- Between the skull and C1, the atlas - Flexion - SCM, scalene, prevertebral muscles - Extension-splenius capitus, cervicis, intrinsic muscles Rotation at C1-C2, axis (chin to each shoulder) - Sternocleidomastoid, small intrinsic neck muscles Lateral bending at C2-C7 (ear to each shoulder) - Scalenes and small intrinsic neck muscles |
|
|
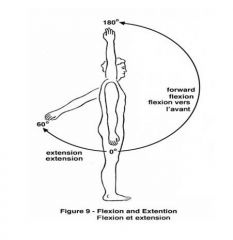
Spinal flexion
|
Psoas major, psoas minor, quadratus lumborum; abdominal muscles attaching to the anterior vertebrae, such as the internal and external obliques and rectus abdominis
Bend forward and try to touch your toes As flexion proceeds, the lumbar concavity (curve in lumbar area) should flatten out. |
|
|
Spinal extension
|
Deep intrinsic muscles of the back, such as the erector spinae and transversospinalis groups.
Bend back as far as possible Support the patient by placing your hand on the posterior superior iliac spine, with your fingers pointing toward the midline. |
|
|
Spinal rotation
|
Abdominal muscles, intrinsic muscles of the back
Rotate from side to side Stabilize the patient's pelvis by placing one hand on the patient's hip and the other on the opposite shoulder then rotate the trunk by pulling the shoulder and then the hip posteriorly and repeat these maneuvers for the opposite side. |
|
|
Spinal lateral bending
|
Abdominal muscles, intrinsic muscles of the back
Bend to the side from the waist Stabilize the patient's pelvis by placing your hand on the patient's hip and repeat for the opposite side. |
|
|
Scoliosis
|

Lateral and rotatory curvature of the spine to bring the head back to midline.
Often becomes evident during adolescence, before symptoms appear. Deformity of the thorax on forward bending. |