![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
152 Cards in this Set
- Front
- Back
|
White Blood Cell |
4.4-11.0 X 10^3/mm^3 |
|
|
Mean Red Cell Volume (MCV) *Ref. range and definition |
80.0-96.0 fL Average size of red blood cells MCV (fL)= (Hematocrit)/(RBC in millions) |
|
|
Mean Cell Hemoglobin concentration (MCHC) *Ref. range, def'n, and equation |
33.4-35.5 g/dL MCHC (or mean corpuscular) average amount of red cell volume occupied by Hgb. COLOR indicator (norma, hypo & hyper chromic) MCHC= (Hemoglobin)/(Hematocrit) *100 |
|
|
Red cell Distribution Width (RDW) *Ref. range, def'n, and equation |
11.5-15.0% Amount of red cell size variation "quantitates anisocytosis (%), meaning variation in size" |
|
|
Platelet Count (PLT) |
150-400 X 10^3/mm^3 |
|
|
Neutrophil % |
50-70 |
|
|
Bands % |
0-10% |
|
|
Lymphocyte % |
18-42% |
|
|
Monocyte % |
2-8%
|
|
|
Eosinophil % |
1-3%
|
|
|
Basophil % |
0-2%
|
|
|
Ave. volume of blood in an adult |
4-6L |
|
|
Differentiate between: Hematocrit- Hemoglobin- |
Hematocrit: % of whole blood volume occupied by RBCs Hemoglobin: Amount of Hgb in a given volume of RBCs (g/dL). The lower the Hgb, the smaller the RBC size |
|
|
MCV (fL): Microcytic= Normacytic= Macrocytic= |
Microcytic: <80 fL Normacytic: 80-100 fL Macrocytic: >100 fL |
|
|
EDTA: What is the mechanism of action? Tube type? Complications with using EDTA on some samples? |
Chelates calcium, so it can't clot. Lav. purple top tube with liquid or powdered EDTA Some people are "EDTA clumpers" either the platelets clump, or the cells do. This falsely increased WBC and decreases platelet count. |
|
|
Sodium Citrate: What is the mechanism of action? Tube type? Why does the tube need to be full? Correction value for WBC and PLTs? |
Binds calcium light blue top tube Ratio of citrate to blood needs to be 1:10 Correction value: multiply by 1.1 |
|
|
Heparin: Used for ______ _______ _______. Mechanism? When performing a CBC using a heparin blood sample which values should you report? *Verdict: good or bad for hematology? |
Used for osmotic fragility procedure. Mechanism- inactivates coagulation factors Report: WBC, RBC, and Hct. *causes clumping, not a good sample for CBC, doesn't stain well. |
|
|
True/False: blood with any amount of macroscopic or microscopic clotting is unsatisfactory. |
TRUE: clotting activates and consumes clotting factors and binds cells in the fibrin mesh making any hematology results erroneous. |
|
|
Define the following QA terms Accuracy: Precision: Reliability: Linearity Sensitivity: Specificity: |
Accuracy: closest to the correct/actual value Precision: reproducibility of results Reliability: precise and accurate over time Linearity: proportional within a range Sensitivity: ability to detect true positives Specificity: ability to detect true negatives |
|
|
As sensitivity increases, specificity ___________. |
As sensitivity increases, specificity decreases. |
|
|
Which blood collection tube is best for doing a peripheral blood smear? |
EDTA sample prepared within 2-3 hrs of collection. |
|
|
When is the preparation of a buffy coat indicated? |
When there is a decreased WBC |
|
|
What are the basic and acidic components of the Wright-Giemsa stain? |
BASIC : methylene blue (attracted to acidic structures such as RNA&DNA) Stains 'em blue. Blue=BASOPHILIC ACIDIC : Eosin, attracted to basic structure (Hgb in RBC) stains it red. |
|
|
How do you perform a WBC estimate? |
40X high dry objective Ave # of WBCs per field *2000=approx. total WBC/mm3 |
|
|
How do you perform a platelet estimate? |
100X oil objective Ave. # Plts* 20,000=platelets/mm3 NORMAL: 8-20 plts |
|
|
What can you add to your slide to avoid creating a smudge artifact? |
Albumin, it stabilizes the cell membrane |
|
|
What is going on inside a pyknotic degenerating cell? |
apoptosis, the nuclear material is losing its chromatin pattern |
|
|
Def'n of anemia |
a condition in which there is reduced oxygen delivery to the tissues |
|
|
causes of anemia |
increased RBC loss from RBC destruction or excessive blood loss decreased production of RBC (erythropoiesis) decreased RBC function |
|
|
Def'n hematopoiesis |
formation, development and specialization of blood cells |
|
|
What are the three phases (sites) of hematopoiesis in utero? |
1. mesoblastic (yolk sac) 2. hepatic (liver) 3. myeloid (medullary = bone marrow) |
|
|
At birth, where are blood cells primarily made? |
Bone marrow in the vertebrae, sternum, ribs, femur and tibia |
|
|
When you are older, where are blood cells primarily made? |
Bone marrow in the vertebrae |
|
|
The lymphoid progenitor cells gives rise to: |
NK cell, B and T lymphocytes |
|
|
A normal adult bone marrow displays ____% tissue and _____% fat. |
50% tissue 50% fat |
|
|
What is the largest lymphoid organ |
spleen |
|
|
What immunoglobulin is synthesized in the spleen? What is stored in the spleen? |
IgM platelets are stored in the spleen |
|
|
what is extra-medullary hematopoiesis? |
It is blood cell development that happens outside the bone marrow, when the spleen does this it is not normal |
|
|
What is splenomegaly |
enlargement of the spleen |
|
|
what treatment is advisd when there is an increased RBC destruction and or decreased plts? |
Splenectomy |
|
|
What are the liver tissue macrophages called |
Kupffer cells- they remove cellular debris |
|
|
Liver & hematopoietic roles: synthesizes: stores: conjugates: |
the liver synthesizes proteins and coag factors stores vitamins and minerals conjugates and transports bilirubin |
|
|
hemolytic anemia and RBC dysplasia is characterized by: |
increased conjugation of bilirubin increased storage of iron |
|
|
enzymatic deficiency that results in accummulation of intermediate products of heme production |
Porphyrias problem w/liver, you can't make enzymes |
|
|
enzymatic deficiency that results in the accumulation of lipids in macrophages |
lipid storage disease liver problem |
|
|
what is diff about lymph (compared to blood) |
lower protein and no RBCs |
|
|
what are the three main functions of lymph nodes |
1. filter particulate matter, debris and bacteria 2. process specific immunoglobulins 3. proliferation of lymphocytes |
|
|
what organ has the following two jobs? 1. promotes differentiation of progenitor lymphoid cells into T cells 2. holding site for T cells (and also B cells, eosinophils, neutrophils and myeloid cells) |
thymus |
|
|
what is the clinical manifestation of not having a thymus develop gestationally |
no T cell formation |
|
|
True/False: adults with thymus disturbance (like an accident) no longer make mature T cells |
False, adults maintain a pool of T cells for life |
|
|
2 types of stem cells: |
1. noncommitted or undifferentiated stem cell (pluripotent stem cell) 2. multi potential and committed progenitor cells (lineage specific precursor) |
|
|
when a monocyte enters a tissue what is it then called? |
macrophage |
|
|
which cells are capable of self renewal |
stem cells, duh. |
|
|
CFU: CFU-L CFU-GEMM |
colony forming units CFU-L: lymphoid CFU-GEMM: granulocyte, erthrocyte, monocyte, megakaryocyte (committed to anything BUT a lymph) |
|
|
which hematopoietic cytokine promotes mast cell (tissue basophil) proliferation? |
Kit ligand (KL) or Stem Cell factor (SCF) |
|
|
which hematopoietic cytokine is particularly effective at very low concentrations? |
interleukins (IL) |
|
|
how is apoptosis initiated |
cells don't receive cytokines necessary to PREVENT cell death |
|
|
what is the first part of the cell to degrade during apoptosis |
nucleus chromatin condensation "pyknotic" |
|
|
EPO is __________, which induces __________ synthesis and stimulates CFU-E to produce RBCs. |
erythropoietin induces hemoglobin synthesis depends on your kidneys ability to detect hypoxia EPO also inhibits RBC apoptosis |
|
|
which cells produced EPO |
renal tubular epithelial cells |
|
|
how are nucleated RBCs formed?? |
nRBCs are formed from the early release of RBCs from the bone marrow after promotion from EPO... they essentially get kicked out before they were ready every single one is clinically significant |
|
|
TPO is ________________, which is a key factor in __________ production. Where is TPO made? |
TPO is thrombopoietin, important for platelet production. Produced by the liver and kidney |
|
|
What is the name of the cell type that is right before (lineage) platelet production? |
megakaryocyte |
|
|
What is the process of hematopoiesis when hypoxia is detected? |
hypoxia (due to decreased RBC, decreased O2 in blood or increased tissue O2 needs) detected, kidneys release erythropoietin, EPO stimulates red bone marrow, RBC numbers increase. |
|
|
If you need more platelets, __________ will prevent the megakaryocytes from dying. |
TPO |
|
|
What is the name of the differential cell counter we use? |
Clay Adams |
|
|
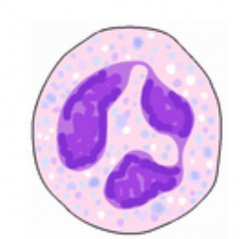
What is the most numerous and most common WBC? What is it primarily used for? |
neutrophil -> phagocytic cell used for defense against bacteria increased in #s during bacterial infection, depleted in viral infection |
|
|
PMN, "poly", "seg": Size: N/C ratio: # lobes: color of cytoplasm: |
10-16um n/c ratio: 1:1 2-5 distinct nuclear lobes pink cytoplasm with deep blue-purple chromatin no nucleoli (RNA, proteins) |
|
|
What is the name of a slightly immature poly? |
Band cell singular lobe, no segment or filament connections |
|
|
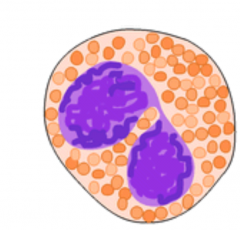
Which cell type serves to mediate immediate hypersensitivity reactions and destroy helminth larvae and other parasites? |
Eosinophils. |
|
|
pmn |
|
|
eosinophil |
|
|
what are nucleoli? |
The largest structure in the nucleus of eukaryotic cells, where it primarily serves as the site of ribosome synthesis and assembly. |
|
|
which type of granulocyte generates histamine and other mediator of the inflammatory response? |
basophil |
|
|
which cell has a lot of the same features as a poly, except that it has coarse purple-black non-uniform specific granules? |
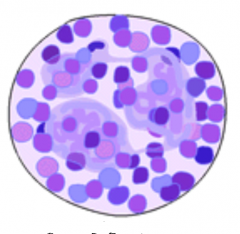
basophils |
|
|
which cell is the bodies' primary defense adjacent viral infection but are necessary as mediators for virtually EVERY immune response? |
LYMPHOCYTES B-lymphs- synthesis and excretion of Ab T-lymphs Cant differentiate on a Wright-stained specimen |
|
|
which cell often has a smudged nuclear chromatin? |
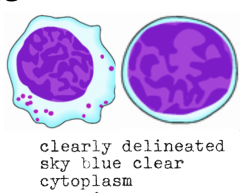
lymphocytes |
|
|
whats the name of an activated T lymph |

reactive lymphocyte features: wandering or ballerina skirt cytoplasm, bluer periphery, coarse nuclear cytoplasm or smudged. |
|
|
T/F: nRBCs are included in the 100 cell diff |
False. |
|
|
If you count more than 5 nrbcs you must correct the automated WBC. whats the equation? |
100*uncorrected WBC/100+nRBC |
|
|
RBC morphology is always done on what objective |
100X |
|
|
in infants birth to 12 mos of age, what is the primary type of WBC? What is it in adults? |
Lyphocyte- up to 61%, their immune systems are still developing. In adults, the most abundant are PMNs. |
|
|
calculation for absolute value of cell type |
Abs value= relative value % * WBC/mm3 |
|

Names: Size: N/C ratio: |
Rubriblast (Pronormoblast) 14-19um, N/C ratio- 4:1 Red-purple finely stippled,granular chromatin, finelace-like |
|

Names Size N/C ratio |
Prorubricyte (Basophilic normoblast) 12-15um, N/C ratio - 3:1 Increased granularity ofnuclear chromatin (moredistinct parachromatin) |
|

Name Size N/C ratio |
Rubricyte (Polychromatic normoblast(polychromatophilic)) 10-15um, N/C ratio - 2:1 Smaller nucleus with increasedcondensation of chromatin,very coarse chromatinpattern(distinct parachromatin) |
|

Names Size N/C ratio |
Metarubricyte (Orthochromic normoblast) 8-12um, N/C ratio - 1:1 Smaller nucleus with pyknoticdegeneration, condensedchromatin, no discernibleparachromatin (nucleus is solid) Lavender/pink cytoplasm |
|

Names Size N/C ratio |
Reticulocyte 7-10um, no nucleus Clear lavender - pink cytoplasm(polychromatophilic). Lackscentral pallor |
|

Names size |
Erythrocyte 6-8um Clear pink cytoplasm, centralpallor 1/3 of cell diameter |
|
|
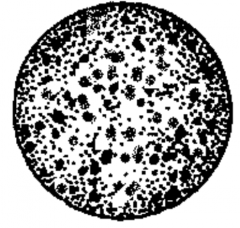
WBC Variant: The stimulation of granulocytic cells results infewer mitotic divisions. Prevents normaldilution of nonspecific granules. Leads to ___________ in _____ and _______ cells. |
Toxic granulation in PMNs and bands (granulocytes) |
|
|
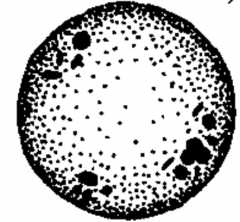
Pale blue translucent bodies in the cytoplasm of granulocytes and monocytes: |
Dohle bodies |
|
|
What are Dohle bodies made of? |
Remnant RNA (often seen along with toxic granulation/vacuoles and shift to the left. |
|
|
How many lobes is considered hypersegmented (in neutrophils)? |
Segmented neutrophils with six or more nuclear lobes. Cells are often larger than normal. Congenital or megaloblastic change. |
|
|
What is the opposite of hyper segmentation? |
Pelger-Huet anomaly, ALL PMNs will have <3 lobes. Typically benign, just note it in the diff. |
|
|
What does pince-nez and Stodtmeister cell refer to? |
Pince-nez are two lobed PMNs Stodtmeister cells are one lobed PMNs |
|
|
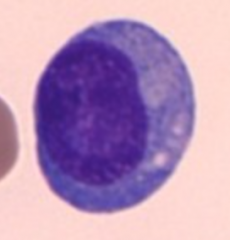
Name for an activated B lymph |
Plasmacytoid lymph |
|
|
Plasmacytoid lymph, with ecentric nucleus that is being pushed to one side by the golgi (which is not visible) |
|
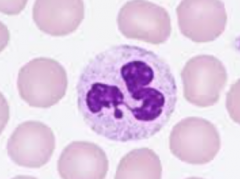
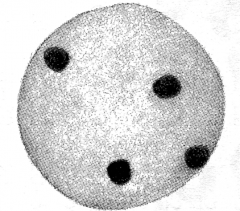
What is this? |
Neutrophil with a Barr body Which is an extra X-chromosome |
|
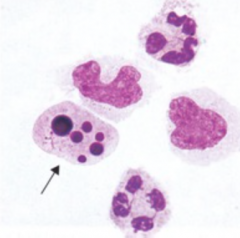
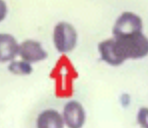
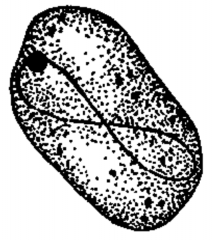
ID the arrow |
This cell is undergoing apoptosis.. Pyknotic degeneration (necrobiotic) |
|
|
What kind of protein spans the lipid bilayer (transmembranous)? example in RBC: |
INTEGRAL Proteins ex: sialic acid - rbc neg chg |
|
|
What kind of protein may interact with lipids at the membrane surface, but don't penetrate the bilayer? example in RBC: |
Peripheral proteins ex: spectrin - cytoskeleton (which modulates shape and deformability) |
|
|
RBC Metabolic Pathway that utilizes Pyruvate kinase (PK) in anaerobic glycolysis. |
Embden-Meyerhof pathway EM path. Net gain of 2 ATP.... glucose metabolism |
|
|
RBC Metabolic Pathway that utilizes Glucose-6-phosphatedehydrogenase (G6PD) as the major enzyme in aerobic glycolysis. |
Hexose Monophosphate Pathway. OXIDATIVE. Combats oxidative injury to RBC. |
|
|
RBC Metabolic Pathway that utilizes 2,3-biphosphoglycerate( 2,3-BPG ) as the enzyme for regulating oxygen delivery to tissues... |
Rapoport-Luebering Pathway |
|
|
RBC Metabolic Pathway that utilizes Methemoglobin reductase as the enzyme.. |
Methemoglobin Reductase pathway. Maintains hemoglobinin its functionally reduced state ( Fe +2 ) |
|
|
Methemoglobinemia (Fe+3) results in ___________. This condition is often caused by.... |
Cyanosis because the Met-Hgb can't carry O2, caused by Hereditary Enzyme Defic., toxic substance exposure (oxidizes Hgb) OR Hgb M Disease. |
|
|
Another name for protoporphyrin IX is ________. |
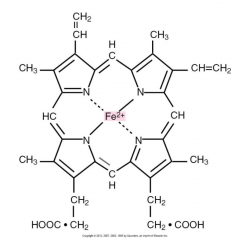
Pyrole ring. Heme - ring of carbon, hydrogen and nitrogenatoms called protoporphyrin IX (or pyrole ring)with an atom of ferrous (Fe+2) iron inserted. |
|
|
Each hemoglobin molecule has _____(#) hemes. |
Each hemoglobin molecule has 4 hemes. |
|
|
Eachhemoglobin moleculehas _______(#) pairs ofpolypeptide chains.Each chain is made upof 141-146 amino acids. |
Eachhemoglobin moleculehas two pairs ofpolypeptide chains.Each chain is made upof 141-146 amino acids. Alpha and beta pairs. |
|
|
How soon after birth does the ratio of Hgb F and Hgb A slowly reverse to the adult ratio> |
6 most of age |
|
|
What are the three intrauterine Hgb? |
Gower 1, Gower 2, and Portland |
|
|
What molecule is critical for regulating oxygen delivery to tissues? |
2,3-BPG Controls Hgb affinity for oxygen |
|
|
What happens when 2,3-BPG binds to oxygenated-hemoglobin? |
The hemoglobin unloads its oxygen and is now "deoxygemoglobin" |
|
|
What happens to the salt bridges in Hgb when it becomes oxygenated? |
Salt bridges are broken, beta chains pull together and 2,3-BPG is expelled. |
|
|
What percentage of oxygen in the Hgb is released to the tissues? |
25%. In lungs - pO2 is ~ 100 mm Hg andHgb is almost 100%saturated with O2 (A) As rbc travels totissues the pO2 dropsto ~ 40mm Hg andthe Hgb saturationdrops to ~ 75%. |
|
|
p50 value is the pO2 at which Hgb is50% saturated withO2 under standard in vitro conditionsof temperature and pH• Reference range: |
P50 = 26-30 mm Hg |
|
|
What is a shift to the right? What it is mediated by? |
This is a compensatory mechanism (ex. in response to hypoxia). Increases the p50 value = more efficient RBC. Mediated by increased 2,3-BPG - which decreasesHgb affinity for O2 and increases O2 deliveredto tissues |
|
|
What is a shift to the left? |
This is when the RBC are less efficient at delivering oxygen to tissues, and the p50 value decreases. Results in increasedO2 affinity anddecreased O2released to tissues |
|
|
In a shift to the right, how do the following change?
pH BPG levels Temp p50 value |
pH decreases BPG, temp and p50 all increase |
|
|
In a shift to the left, how do the following change? pH BPG levels p50 value |
pH increases BPG, temp and p50 value all decrease |
|
|
What is oxidized iron? If you lack Met-Hgb reductase, what does this lead to? |
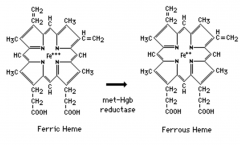
Iron in the ferric (+3) state Hgb molecule changes and O2affinity of other heme groups increases resultingin Shift to the Left. |
|
|
Hgb modified by irreversible oxidation by certaindrugs or chemicals such as sulfonamides. |
Sulfhemoglobin Ineffective for O2 transport– (100 x less affinity for oxygen) |
|
|
The binding of carbon monoxide to heme iron results in what modified hemoglobin?? This Hgb has _____x more affinity for CO than 02 |
Carboxyhemoglobin Hgb has 200x more affinity for CO than 02 The blood is bright, cherry red |
|
|
__________ __________ is the Normal Catabolism of Senescent RBCs |
Extravascular Hemolysis |
|
|
Abnormal amount ofvariation in rbc size |
anisocytosis |
|
|
Name the associated morphology: Rbc <7um or MCV < 80 fL. This is an indicator of what kind of problem? |
Microcytosis, often accompanied by hypochromasia. Indicator of Hgb production problem. |
|
|
Name the associated morphology: Rbc >8um or MCV >100 fL. This is an indicator of what kind of problem? |
Macrocytosis, indicates a DNA synthesis problem. Fewer mitotic divisions in mitosis. |
|
|
Hypochromasia is due to what? Hypo chromatic cells are also often _____, with an MCHC < ________. |
RBCs that lack the normal amount of Hgb. (iron deficiency, thalassemia) Often microcytic. Often the MCHC <32. |
|
|
What does the supra vital stain do? |
It is useful for viewing and counting reticulocytes. |
|
|
polychromasia.... diffuse pale blue/gray or lavender (due to remnant RNA) and it picks up more methylene blue stain. often macrocytic and lack central pallor |
|
|
variation in RBC shape is called: |
Poikilocytosis (POIK) |
|
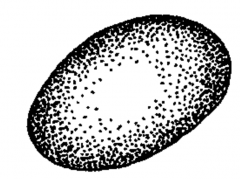
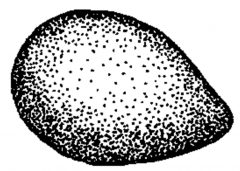
Name: Caused by: |
ovalocytes or elliptocytes (cigar or egghead shaped) Rounded ends. DUE TO: hereditary, IDA, megaloblastic anemias, thalassemias, myelodyplastic syndromes... |
|
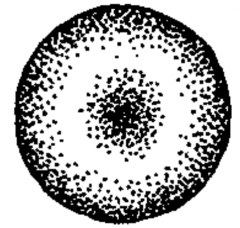
Name: Caused by: |
Target cells (codocytes) increased membrane lipid resulting in increased surface area or decreased Hgb. Also: liver disease, anemias, IDA, any Hgb abnormalities |
|

Name: This is due to the presence of what? |
Sickle cells (Drepanocytes) pointed ends "oat shaped" Due to presence of abnormal Hgb S in decreased O2, tension cells will take a crescent or sickle form. |
|
Crystal Cells form due to.... |
Due to the condensation of abnormal Hgb C ... often into "washington monument" shaped formations |
|
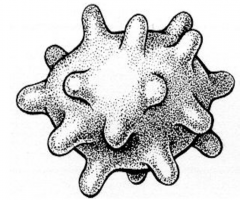
Names? Due to... |
BURR cells (echinocytes) small, blunt evenly spaced projections. Due to the change in the tonicity of intravascular fluid. Also: Uremia, liver disease, burns, anemias, MAHA |
|
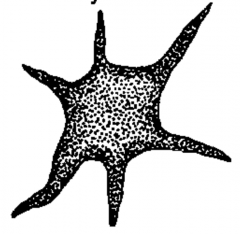
Name: Due to: |
Acanthocytes, long irregular, spiny uneven projections. Due to Abnormal membrane lipids, liver disease, abetalipoproteinemia |
|

Name: |
Schistocytes - fragmented RBCs Due to DIC, TTP, HUS, Hemolysis, MAHA, AproL (M3) |
|
Name: Due to: |
Tear drop (Dacryocytes) Due to formation from inclusion containing RBCs, myelofibrosis |
|
Name: Due to: |
Spherocytes Due to defect in or loss of cell membrane Usually microcytic, MCHC may be >36 (b/c they are so small, it gives a really high MCHC) |
|
Name: Due to: |
Stomatocytes. Central pallor is slit or mouth shaped. Due to artifact, hereditary (Na/K pumps OR Rh def. syndrome) or liver disease |
|
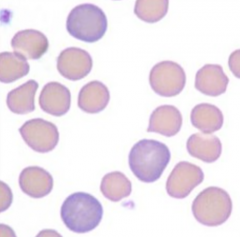
What is this called, how can you reduce this? Disease associations... |
Rouleax- increased plasma proteins or Igs. Reduce this by using the saline replacement technique. Multiple myeloma, Waldenstrom's macroglobulinemia. |
|
Name: What is it made of? Due to: |
Howell-Jolly Body. Busy bone marrow, NUCLEAR REMNANT. Due to: hemolytic & megaloblastic anemias, thalassemias, splenectomy |
|
Name: What are they made of? Due to... |
Basophilic stippling of remnant precipitated RNA, reticulocyte (Slightly immature). Due to: bodies attempt to compensate for blood loss/hemolysis Course stippling attributed to lead poisoning. |
|
Name: Made of... Due to... |
Pappenheimer bodies. Clustured near periphery, made of granules of iron, ineffective utilization or excess iron. Due to: sideroblastic anemias, hemochromatosis, hemoglobinopathies, thalassemias |
|
Name: Made of... Due to... |
Cabot ring No DNA, just the remnant nuclear membrane. |
|
Name: Made of... Due to... |
Heinz bodies. These are not visible with Wright stain. Requires supra vital stain The bodies are precipitated, denatured Hgb due to oxidative injury. Due to G6PD deficiency! (think Hexose Monophosphate Pathway) |
|
|
State the hemoglobins normally found in an adult, the approximate percentage, and globin chain composition of each. |
Hgb A: alpha 2, beta 2 (>95%) Hgb A2: alpha 2, delta 2 (~2%) Hgb F: alpha 2, gamma 2 (1-2%) |
|
|
State the predominant hemoglobin in newborns and give its globin chain composition. |
Hgb F: alpha 2, gamma 2 (60-90%) |
|
|
Methemoglobin is.... |
Iron in the ferric state (Fe+3) can’t bind O2 Seen in presence of oxidants such as nitrites, decreased activity of methemoglobin reductase, or inherited HbM disease (abnormal globin structure) |
|
|
which RBC inclusion is only visible when stained with a supra vital stain? |
Heinz bodies |
|
|
1. State the length of normal rbc survival incirculation. |
120 d |