Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
258 Cards in this Set
- Front
- Back
|
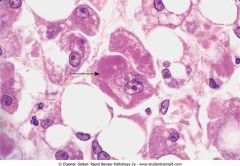
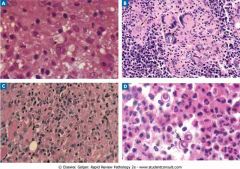
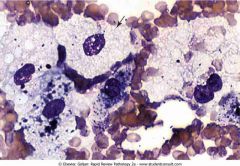
Mallory bodies.
Hyaline (eosinophilic) inclusions (arrow) are present in the cytosol of hepatocytes. Damaged ("ubiquinated") cytokeratin intermediate filaments in hepatoeytes in alcoholic liver disease. |
|
|
|
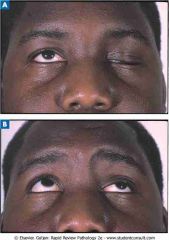
A and B, Right-sided Bell's palsy showing inability to fully close the eye and drooping of the corner of the mouth
|

|
|
|
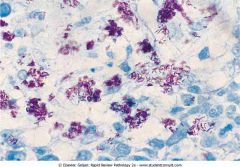
Acid-fast stain of a lung biopsy in a patient with reactivation tuberculosis due to Mycobacterium tuberculosis
|
|
|
|
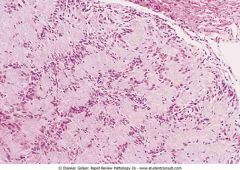
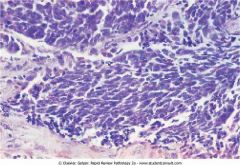
Acoustic neuroma showing spindle-shaped cells with alternating dark and light areas
|
|
|
|
Bronchopneumonia showing patchy areas of consolidation
|

|
|
|
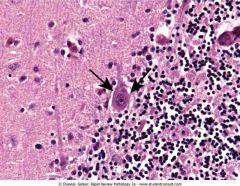
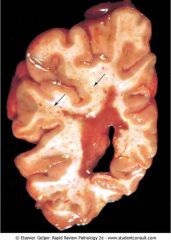
Cerebellum in a patient with rabies showing Purkinje cells with intracytoplasmic, eosinophilic inclusions (arrows) called Negri bodies
|
|
|
|
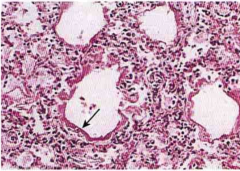
Common systemic fungal infections. The yeast form of Cryptococcus neoformans (A) produces a narrow-based bud (arrow). Coccidioides immitis (B) has spherules containing endospores (arrows). Multinucleated giant cells. Blastomyces dermatitis (D) is a yeast that forms broad-based buds.
|
|
|
|
Dependent pitting edema showing depressions in the skin around the ankle. Pitting edema is due to an increase in vascular hydrostatic pressure or a decrease in vascular oncotic pressure (hypoalbuminemia)
|

|
|
|
Dermatographism
|

|
|
|
Diffuse membranous glomerulopathy.
The H&E (hematoxylin and eosin)-stained biopsy shows glomerular basement membranes that are uniformly thickened. There is no proliferative component. |

|
|
|
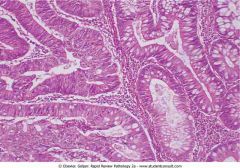
Diffuse type of gastric adenocarcinoma with signet-ring carcinoma cells (arrows)
|
|
|
|
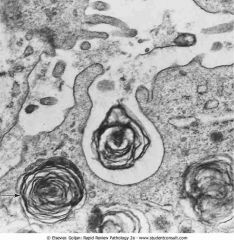
Electron micrograph of a type II pneumocyte showing lamellar body (arrow) containing surfactant
|
|
|
|
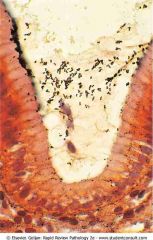
Embryonated eggs of Enterobius vermicularis
aka pinworm, a nematode (roundworm), intestinal parasite that causes enterobiasis |

|
|
|
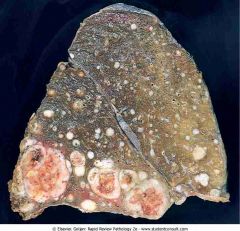
Metastatic renal cell carcinoma showing multiple nodular lesions scattered throughout the lung parenchyma
|
|
|
|
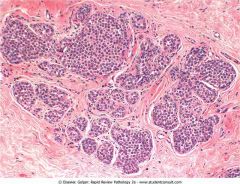
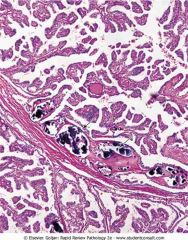
Fibroadenoma
|

|
|
|
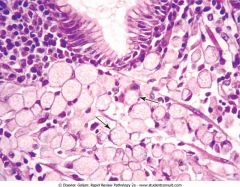
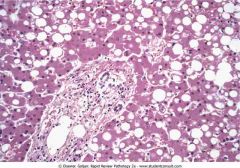
Fatty change of the liver.
Vacuoles containing triglyceride are noted in most of the hepatocytes. Nucleus is displaced to periphery. |
|
|
|
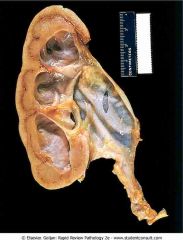
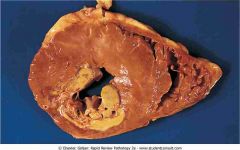
Hydronephrosis of the kidney. There is marked dilation of the renal pelvis and calyces with thinning of the overlying cortex and medulla due to compression atrophy
|
|
|
|
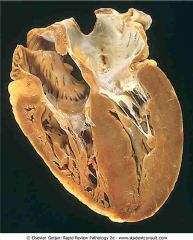
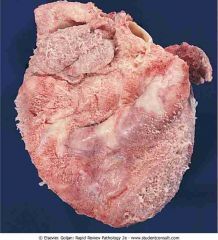
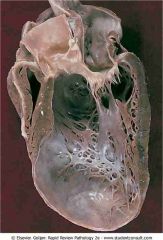
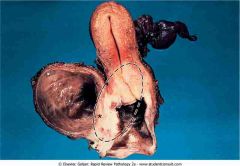
Left ventricular hypertrophy
|
|
|
|
Benign prostatic hyperplasia
|

|
|
|
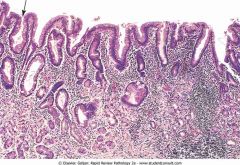
Intestinal metaplasia of the gastric mucosal epithelium in chronic gastritis
|
|
|
|
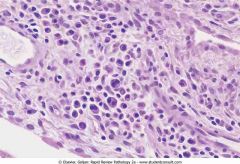
Squamous dysplasia of the cervix, a precursor of squamous cell carcinoma. There is a lack of orientation of the squamous cells throughout the upper two thirds of the epithelium, Many ofthe nuclei arc enlarged {arrows), are hyperchromatic, and have irregular nuclear margins.
|
|
|
|
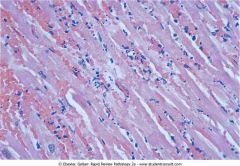
Acute myocardial infarction (MI) showing coagulation necrosis.
|
|
|
|
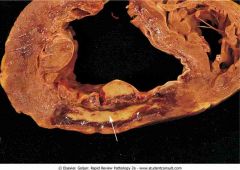
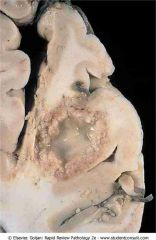
Acute myocardial infarction (MI) showing a pale infarction of the posterior wall of the left ventricle (bottom left)
|
|
|
|
Hemorrhagic infarction of the lung. There is a roughly wedge-shaped area of hemorrhage.
|

|
|
|
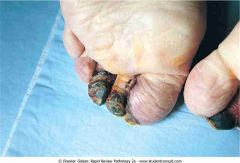
Dry gangrene of the toes
|
|
|
|
Cerebral infarction showing liquefactive necrosis
|

|
|
|
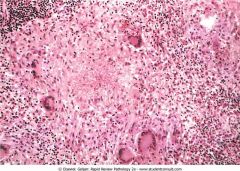
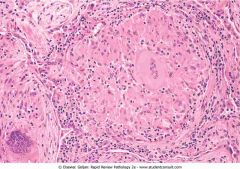
Caseous granuloma showing a central area of acellular, necrotic material surrounded by activated macrophages (epithelioid cells), lymphocytes, and multiple multinucleated Langhans-type giant cells
|
|
|
|
Enzymatic fat necrosis in acute pancreatitis
|

|
|
|
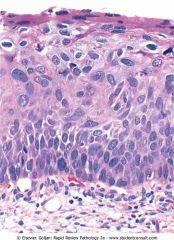
Apoptosis in the epidermis. The arrow shows a clear space in the epidermis containing an intensely eosinophilic staining cell with a small, dense nucleus.
|

|
|
|
Signs of acute inflammation. The patient has erysipelas of the face due to group A streptococcus. Signs of acute inflammation that are present in the photograph include redness (rubor) and swelling (tumor)
|

|
|
|
Acute inflammation. Histologic section of lung in bronchopneumonia showing sheets of neutrophils with multilobed nuclei.
|
|
|
|
Purulent (suppurative) inflammation. The photograph shows a skin abscess (furuncle) due to Staphylococcus aureus. Abscesses are pus-filled nodules located in the dermis.
|

|
|
|
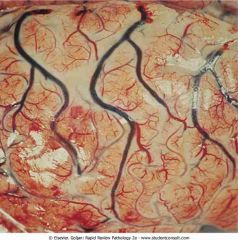
Fibrinous inflammation. The epicardial surface of the heart is covered by a shaggy layer of fibrin material
|

|
|
|
Pseudomembranous inflammation. There is necrosis and a yellow-colored exudate covering the mucosal surface of the colon due to a toxin produced by Clostridium difficile.
|

|
|
|
Chronic inflammation. This tissue shows an infiltrate of predominantly plasma cells (cells with eccentric nucleus and perinuclear clearing) and lymphocytes
|
|
|
|
Ehlers-Danlos syndrome
|

|
|
|
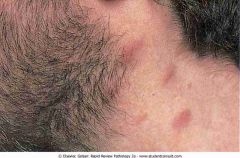
Keloid formation
|

|
|
|
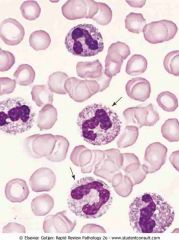
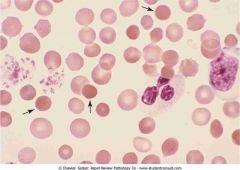
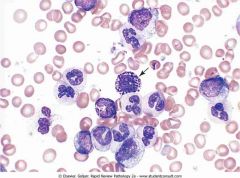
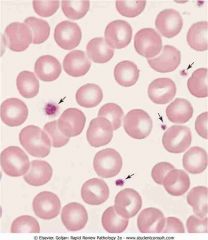
Absolute leukocytosis with left shift. Arrows point to band (stab) neutrophils, which exhibit prominence of the azurophilic granules (toxic granulation). Vacuoles in the cytoplasm represent phagolysosomes
|
|
|
|
Malar rash in systemic lupus erythematosus showing the butterfly-wing distribution
|

|
|
|
Systemic sclerosis. The tightening of the skin around the mouth is caused by excess collagen.
|

|
|
|
Kaposi's sarcoma in HIV. Skin lesions are raised, red, and nonpruritic
|
|
|
|
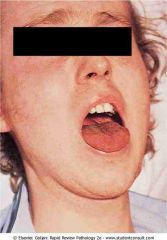
Patient with signs of volume the mucosal surface of the tongue is dry. Additional findings on examination were hypotension, tachycardia, and decreased skin turgor. (From Forbes C, depletion
|
|
|
|
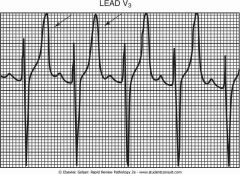
Electrocardiogram showing hyperkalemia. Arrows show peaked T waves, which are a sign of hyperkalemia.
|
|
|
|
Coronary artery thrombosis. In this specially stained cross-section of a coronary artery, collagen is blue and the thrombus is red
|

|
|
|
Pulmonary embolus. The main branches of the pulmonary artery are occluded with large-caliber thromboemboli (saddle emboli)
|

|
|
|
Down syndrome. The facial profile (A) shows a short stature, small head with small nose and ears. The hand (B) shows a single palmar (simian) crease
|

|
|
|
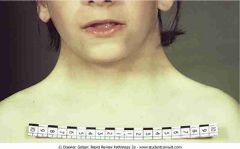
Turner's syndrome is characterized by a webbed neck
|
|
|
|
Klinefelter's syndrome
|

|
|
|
Prader-Willi syndrome
|

|
|
|
Angelman syndrome
|

|
|
|
Testicular feminization. The patient is genotypically male, but phenotypically female
|
|
|
|
Black widow spider
|

|
|
|
Brown recluse spider
|

|
|
|
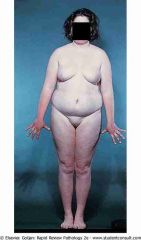
Kwashiorkor and marasmus.
Left, Child with kwashiorkor, showing dependent pitting edema involving the lower legs. Right, Child with marasmus, showing broomstick extremities with loss of muscle mass and subcutaneous fat. |

|
|
|
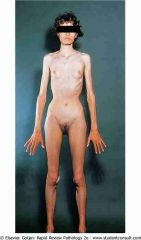
Anorexia nervosa
|
|
|
|
Gums showing the effects of scurvy
|

|
|
|
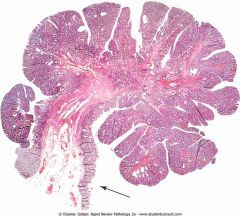
Tubular adenoma (adenomatous polyp) of the colon showing a fibrovascular stalk
|
|
|
|
Lipoma showing a well-circumscribed yellow tumor (A) containing benign adipose cells (B)
|

|
|
|
Cystic teratoma of the ovary,
|

|
|
|
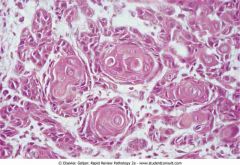
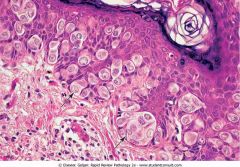
Squamous cell carcinoma.
The many well-differentiated foci of eosinophilic-staining neoplastic cells produce keratin in layers (keratin pearls). |
|
|
|
Adenocarcinoma. Irregular glands infiltrate the stroma
|
|
|
|
Osteogenic sarcoma of the distal femur. The light-colored mass of tumor in the metaphysis abuts the epiphyseal plate (arrow)
|

|
|
|
Metastasis to the liver. The liver contains multiple nodules that have a depressed central area (umbilicated)
|

|
|
|
Basal cell carcinoma (invasive tumor that does not metastasize)
|

|
|
|
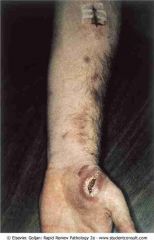
Malignant melanoma. The lesion on the patient's forearm is black, is multinodular, and has an irregular border with areas of pale-gray discoloration
|

|
|
|
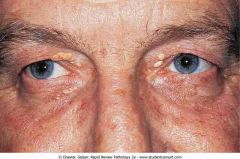
Xanthelasma.
Yellow, raised lesions on both eyelids. |
|
|
|
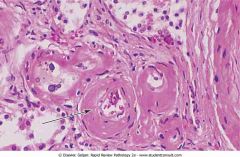
Hyaline arteriolosclerosis
|
|
|
|
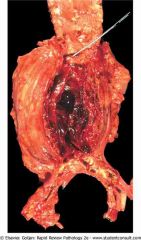
Abdominal aortic aneurysm
|
|
|
|
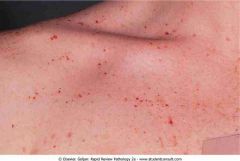
Henoch-Schönlein purpura
|

|
|
|
Acute myocardial infarction (day 7) in the posterior wall of the left ventricle
|
|
|
|
Fibrinous pericarditis.
Surface of the heart is covered by a shaggy, fibrinous exudate |
|
|
|
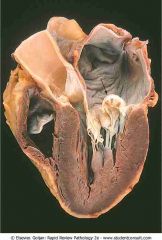
Left ventricular aneurysm.
Bulging aneurysm has a thin wall of scar tissue. |
|
|
|
Acute rheumatic fever.
Uniform, verrucoid-appearing sterile vegetations appear along the line of closure of the mitral valve |

|
|
|
Mitral valve prolapse.
Arrow shows prolapse of the posterior mitral leaflet into the left atrium |
|
|
|
Aortic stenosis
|

|
|
|
Acute bacterial endocarditis
|

|
|
|
Myocarditis.
Biopsy shows a lymphocytic infiltrate with dissolution of myocardial fibers |
|
|
|
Peripheral blood reticulocytes with supravital stain (new methylene blueView drug information). Red blood cells with thread-like material in the cytosol represent residual RNA filaments and protein (arrow)
|
|
|
|
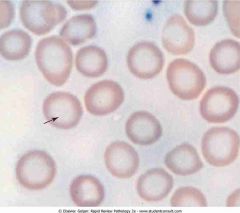
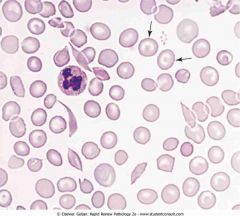
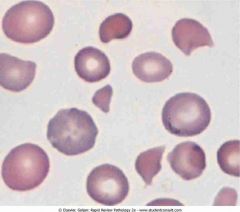
Peripheral blood smear in iron deficiency anemia. The enlarged central area of pallor in the red blood cell (arrow) indicates a decrease in hemoglobin synthesis.
|
|
|
|
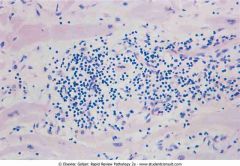
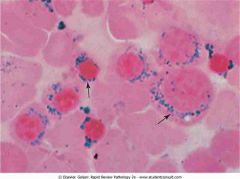
Ringed sideroblasts in a bone marrow aspirate. Dark blue iron granules around the nucleus of developing normoblasts (arrows) represent iron trapped within mitochondria and indicate a defect in mitochondria.
Causes of sideroblastic anemia can be categorized into three groups: congenital sideroblastic anemia, acquired clonal sideroblastic anemia, and acquired reversible sideroblastic anemia. All cases involve dysfunctional heme synthesis or processing. This leads to granular deposition of iron in the mitochondria that form a ring around the nucleus of the developing red blood cell. Congenital forms often present with normocytic or microcytic anemia while acquired forms of sideroblastic anemia are often normocytic or macrocytic. 1. Congenital sideroblastic anemia X-linked sideroblastic anemia: This is the most common congenital cause of sideroblastic anemia and involves a defect in ALAS2, which is involved in the first step of heme synthesis. Although X-linked, approximately one third of patients are women due to skewed X-inactivation. Autosomal recessive sideroblastic anemia involves mutations in the SLC25A38 gene. The function of this protein is not fully understood, but it is involved in mitochondrial transport of glycine. Glycine is a substrate for ALAS2 and necessary for heme synthesis. The autosomal recessive form is typically severe in presentation. 2. Genetic syndromes: Rarely, sideroblastic anemia may be part of a congenital syndrome and present with associated findings, such as ataxia, myopathy, and pancreatic insufficiency. Acquired clonal sideroblastic anemia Clonal sideroblastic anemias fall under the broader category of myelodysplastic syndromes (MDS). Three forms exist and include refractory anemia with ringed sideroblasts (RARS), refractory anemia with ringed sideroblasts and thrombocytosis (RARS-T), and refractory cytopenia with multilineage dysplasia and ringed sideroblasts (RCMD-RS). These anemias are associated with increased risk for leukemic evolution. 3. Acquired reversible sideroblastic anemia Causes include excessive alcohol use (the most common cause of sideroblastic anemia), pyridoxine deficiency, lead poisoning, and copper deficiency. Excess zinc can indirectly cause sideroblastic anemia by decreasing absorption and increasing excretion of copper. Antimicrobials that may lead to sideroblastic anemia include isoniazid, chloramphenicol, cycloserine, and linezolid. Also see Pappenheimer bodies. |
|
|
|
Peripheral blood with coarse basophilic stippling of RBCs in lead poisoning. Note the mature RBC containing numerous dots representing ribosomes (arrow)
|
|
|
|
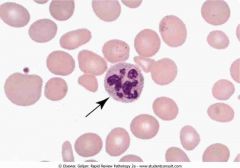
Peripheral blood in megaloblastic anemia showing the hypersegmented neutrophil (arrow) with nine lobes
|
|
|
|
Peripheral blood with spherocytes in hereditary spherocytosis. Numerous, round, dense red blood cells (RBCs) without central areas of pallor represent spherocytes (arrows). The mean corpuscular hemoglobi
|
|
|
|
Peripheral blood with sickle cells and target cells, showing the dense, boat-shaped sickle cells. Cells with a bull's-eye appearance are target cells (arrows), which have excess RBC membrane that bulges
|
|
|
|
Peripheral blood with sickle cells and Howell-Jolly bodies. The three dense boat-shaped sickle cells and the two cells containing a single dark, round inclusion (arrows) represent nuclear remnants.
|

|
|
|
Peripheral blood with schistocytes. The fragmented red blood cells (RBCs) with absence of central pallor, schistocytes, are produced when RBCs are mechanically injured by calcium deposits in an aortic valve
|
|
|
|
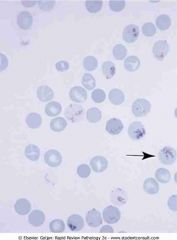
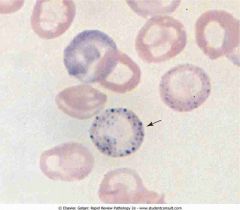
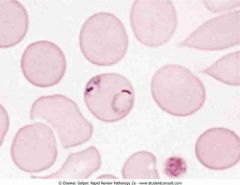
Plasmodium falciparum ring forms in red blood cells (RBCs). This RBC has two ring forms. Multiple infestation of an RBC is characteristic of P. falciparum malaria
|
|
|
|
Leukoerythroblastic reaction. Numerous bone marrow reticulocytes with a blue discoloration
|
|
|
|
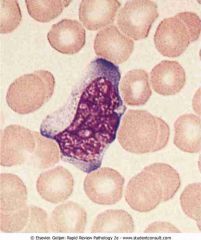
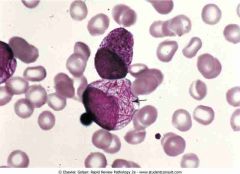
Peripheral blood with atypical lymphocyte. The cell shows prominent nucleoli and coarse nuclear chromatin. The cytoplasm is abundant and is indented by adjacent red blood cells
Distinctive cell associated with EBV or CMV is known as a "Downey cell." Reactive lymphocytes are usually associated with viral illnesses, however, they can also be present as a result of drug reactions (such as phenytoin), immunisations, radiation, hormonal causes (such as stress and Addison's disease) as well as some auto-immune disorders (such as rheumatoid arthritis). Some pathogen-related causes include: Epstein-Barr virus Cytomegalovirus Toxoplasma Treponema pallidum (Syphilis) Streptococcus agalactiae (Group B Streptococci), Hepatitis C Hantavirus |
|
|
|
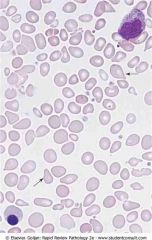
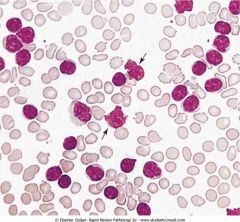
Peripheral blood in chronic myelogenous leukemia. Marked leukocytosis shows neutrophils at different stages of development (segmented and band neutrophils, metamyelocytes and myelocytes)
|
|
|
|
Peripheral blood with promyelocyte filled with Auer rods in acute promyelocytic leukemia
|
|
|
|
Peripheral blood in chronic lymphocytic leukemia
|
|
|
|
Gaucher disease
|
|
|
|
Niemann-Pick disease
|
|
|
|
Senile purpura
|

|
|
|
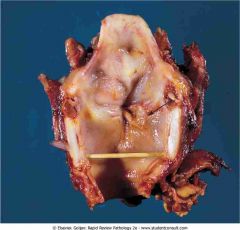
Laryngeal squamous cell carcinoma
|
|
|
|
Asbestos body
|

|
|
|
Malignant mesothelioma
|

|
|
|
Sarcoid granuloma
|
|
|
|
Chest radiograph in emphysema
|

|
|
|
Primary lung cancer
|

|
|
|
Small cell carcinoma of the lung
|
|
|
|
Oral thrush
|

|
|
|
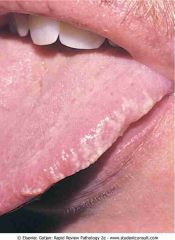
Hairy leukoplakia along the lateral.
|
|
|
|
Leukoplakia of the tongue
|

|
|
|
Barrett's esophagus
|

|
|
|
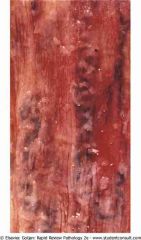
Esophageal varices
|
|
|
|
Gastric adenocarcinoma
|

|
|
|
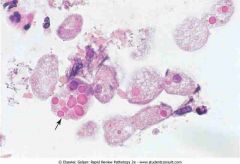
Entamoeba histolytica trophozoites
|
|
|
|
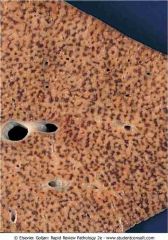
Celiac disease
|

|
|
|
Dermatitis herpetiformis
most common in patients of northern European ancestry, and is associated with the HLA-DQ2 haplotype along with celiac disease and gluten sensitivity |

|
|
|
Hemorrhagic infarction
|

|
|
|
Meckel diverticulum
|

|
|
|
Sigmoid diverticulosis
|

|
|
|
Ulcerative colitis.
|

|
|
|
. Crohn's disease
|

|
|
|
Tubular adenoma
|

|
|
|
Familial polyposis
APC gene, auto rec |

|
|
|
Acute appendicitis
|

|
|
|
. Centrilobular hemorrhagic necrosis
|
|
|
|
Alcoholic cirrhosis
|

|
|
|
Spider angioma (telangiectasia)
|

|
|
|
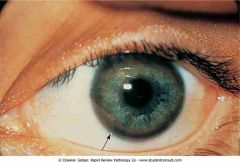
Kayser-Fleischer ring.
|
|
|
|
Hepatocellular carcinoma
|

|
|
|
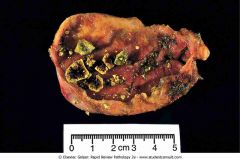
Yellow cholesterol stones
|
|
|
|
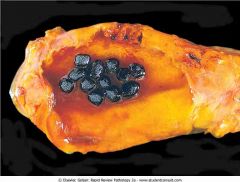
Black pigmented stones
|
|
|
|
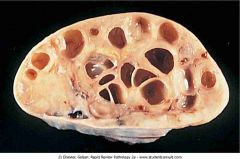
Adult polycystic kidney disease
|

|
|
|
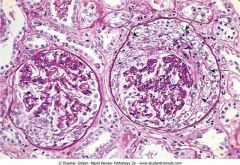
Normal glomerulus
|
|
|
|
Subepithelial immunocomplex
|

|
|
|
Red blood cell cast in the urine
|
|
|
|
Crescentic glomerulonephritis
|
|
|
|
Fatty cast under polarization
|

|
|
|
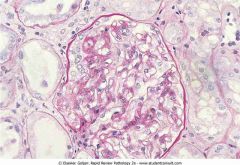
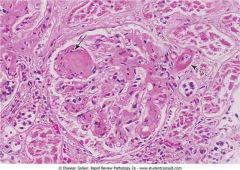
. Diabetic glomerulosclerosis
|
|
|
|
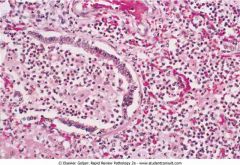
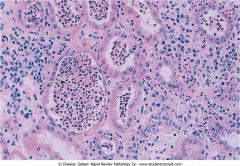
Acute pyelonephritis.
|
|
|
|
Waxy cast in the urine sediment
suggest the very low urine flow associated with severe, longstanding kidney disease such as renal failure. Additionally, due to urine stasis and their formation in diseased, dilated ducts, these casts are significantly larger than hyaline casts. While cylindrical, they also possess a higher refractive index and are more rigid, demonstrating sharp edges, fractures, and broken-off ends. Waxy casts also fall under the umbrella of “broad” casts, a more general term to describe the wider cast product of a dilated duct. It is seen in chronic renal failure. In nephritic syndrome many additional types of casts include broad and waxy casts if the condition is chronic (this is referred to as a telescopic urine with the presence of many casts) |

|
|
|
Benign nephrosclerosis
|

|
|
|
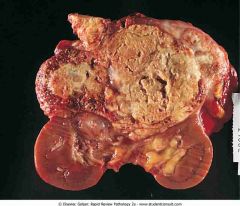
Renal cell carcinoma
|
|
|
|
Benign prostatic hyperplasia
|

|
|
|
Prostate cancer. Arrow
|

|
|
|
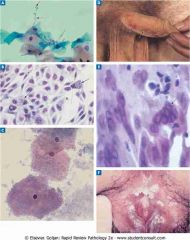
A, Candida.
B, Chlamydia trachomatis. C, Gardnerella vaginalis. D, Herpes type E, Herpes type 2. F, Human papillomavirus. |
|
|
|
G, Neisseria gonorrhoeae.
H, Treponema pallidum. I, Treponema pallidum. J, Trichomonas vaginalis. |

|
|
|
Extramammary Paget's disease
|
|
|
|
Squamous cell carcinoma of cervix
|
|
|
|
Polycystic ovarian syndrome
|
|
|
|
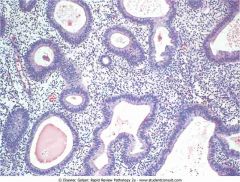
Simple hyperplasia of endometria
|
|
|
|
Endometrial carcinoma
|

|
|
|
Leiomyomas.
|

|
|
|
Ruptured ectopic tubal pregnancy
|

|
|
|
Complete hydatidiform mole
|

|
|
|
Ductal carcinoma in situ (DCIS)
|

|
|
|
Lobular carcinoma in situ
|
|
|
|
Infiltrating ductal carcinoma.
|

|
|
|
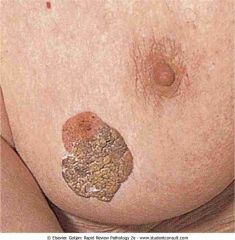
Paget's disease of the breast
|

|
|
|
Acromegaly showing the patient
|

|
|
|
Primary hypothyroidism
|

|
|
|
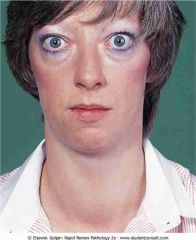
Graves' disease
|
|
|
|
Papillary carcinoma of thyroid.
|
|
|
|
Patient with Cushing syndrome
|

|
|
|
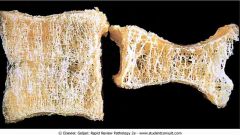
Osteoporosis of vertebral column
|
|
|
|
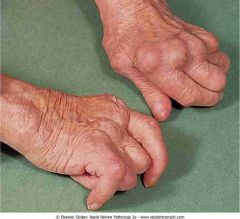
.Rheumatoid arthritis
|
|
|
|
Tophi (arrows)
|

|
|
|
Erythema chronicum migrans
|

|
|
|
Verruca vulgaris (common wart)
|

|
|
|
Molluscum contagiosum
|

|
|
|
Erythema infectiosum
|

|
|
|
Varicella infection of skin
|

|
|
|
Impetigo of the face
|

|
|
|
Patient with severe facial acne
|

|
|
|
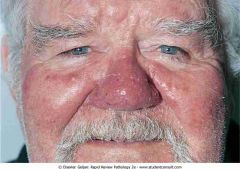
Acne rosacea
|
|
|
|
Tinea versicolor.
|

|
|
|
Lymphocutaneous sporotrichosis
|
|
|
|
Contact dermatitis.
|

|
|
|
Actinic (solar) keratosis
|

|
|
|
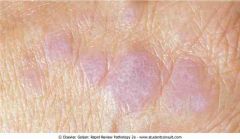
Lichen planus
Pruritic, purple, polygonal planar papules and plaques (6 P's) |
|
|
|
Psoriasis involving the elbow
|

|
|
|
Nail changes in psoriasis
|

|
|
|
Pityriasis rosea
|

|
|
|
Erythema multiform
allergic reaction or infection mediated by deposition of immune complex (mostly IgM) in the superficial microvasculature of the skin and oral mucous membrane that usually follows an infection or drug exposure. Infections: Bacterial (including Bacillus Calmette-Guérin (BCG) vaccination, haemolytic Streptococci, legionellosis, leprosy, Neisseria meningitidis, Mycobacterium, Pneumococcus, Salmonella species, Staphylococcus species, Mycoplasma pneumoniae), Chlamydial. Fungal Parasitic (Trichomonas species, Toxoplasma gondii), Viral (especially Herpes simplex) Drug reactions, most commonly to: Antibiotics (including, sulphonamides, penicillin), anticonvulsants (phenytoin, barbiturates), aspirin, antituberculoids, and allopurinol and many others. Physical factors - Radiotherapy, cold, sunlight Others - Collagen diseases, vasculitides, non-Hodgkin lymphoma, leukaemia, multiple myeloma, myeloid metaplasia, polycythemia |

|
|
|
Erythema nodosum
inflammation of the fat cells under the skin, resulting in tender red nodules or lumps that are usually seen on both shins A useful mnemonic for causes is SORE SHINS (Streptococci, OCP, Rickettsia, Eponymous (Bechet), Sulfonamides, Hansen's Disease (Leprosy), IBD, NHL, Sarcoidosis. HLA-B27 association. Idiopathic - In about 30-50% of cases, the cause of EN is unknown. Infection: Streptococcal infection which, in children, is by far the most common precipitant, Primary infection of Tuberculosis Mycoplasma pneumoniae Yersinia Hepatitis C Epstein-Barr virus Coccidioides immitis Cat scratch disease Autoimmune disorders, including, Inflammatory bowel disease, Behçet's disease, and Sarcoidosis Pregnancy Medications, including, Sulfonamides, Penicillins, Oral contraceptives, Bromides, Hepatitis B vaccination Cancer, including Non-Hodgkins lymphoma, carcinoid tumors, and pancreatic cancer |

|
|
|
Granuloma annulare
autoimmune reaction that causes over-productive leukocytosis females (80/20 ratio) The condition is usually seen in otherwise healthy people. Occasionally, it may be associated with diabetes or thyroid disease. It has also been associated with auto-immune diseases such as systemic lupus erythematosus, rheumatoid arthritis, and Addison's disease. |

|
|
|
Acanthosis nigricans
|

|
|
|
Solar lentigo
|

|
|
|
Seborrheic keratosis on the breast
|
|
|
|
Compound nevus
|

|
|
|
Lentigo maligna melanoma
|

|
|
|
Anencephaly
|

|
|
|
Neurofibromatosis
|

|
|
|
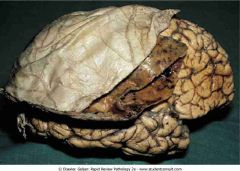
Epidural hematoma
|

|
|
|
Subdural hematoma
|
|
|
|
Atherosclerotic stroke.
|
|
|
|
Embolic stroke
|

|
|
|
Intracerebral hemorrhage
|

|
|
|
Bacterial meningitis
|
|
|
|
Cerebral abscess
|
|
|
|
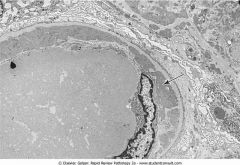
Fusion of the podocytes. Arrowheads show fusion of the podocytes, which should be separated by slit pores. This finding occurs in all glomerular diseases that present with the nephrotic syndrome (e.g., minimal change
|

|
|
|
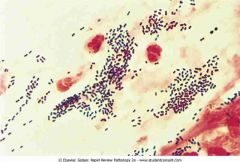
Gram stain of Streptococcus pneumoniae. The sputum stain shows numerous lancet-shaped diplococci
|
|
|
|
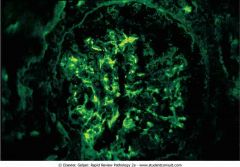
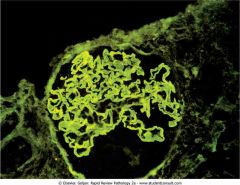
Granular immunofluorescence. Granular irregular deposits in the capillaries are caused by immunocomplex deposition (e.g., poststreptococcal glomerulonephritis
|
|
|
|
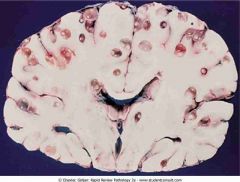
Brain of a newborn with kernicterus. Arrows depict yellow bilirubin pigment deposited in the basal ganglia
|

|
|
|
Herpes zoster
|

|
|
|
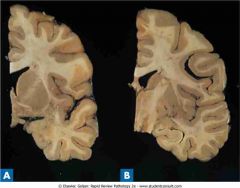
Huntington disease. Coronal section (A) shows a dilated lateral ventricle and atrophy of the caudate, putamen, and globus pallidus when compared with a normal coronal section (B)
|
|
|
|
If the crystal is blue when parallel to the slow ray, the crystal demonstrates positive birefringence.
|

|
|
|
Normal peripheral blood smear showing RBCs. The RBCs are uniform in size, and the central areas of pallor are slightly less than half the total diameter of an RBC. The four dark objects (arrows) outside
|
|
|
|
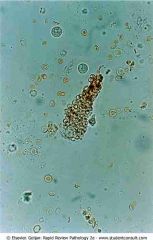
Giardia lamblia with two nuclei
|
|
|
|
Man with ankylosing spondylitis
|

|
|
|
Keratoacanthoma
|

|
|
|
classic Reed-Sternberg (RS) cell. The large, multilobed cell with prominent nucleoli is surrounded by a halo of clear nucleoplasm. Classic RS cells are more easily found in mixed-cellularity Hodgkin's lymphoma
|
|
|
|
Linear immunofluorescence. The uninterrupted smooth immunofluorescence along the glomerular basement membrane is caused by deposition of IgG antibodies directed against the membrane (e.g., Goodpasture syndrome)
|
|
|
|
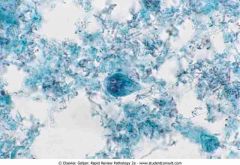
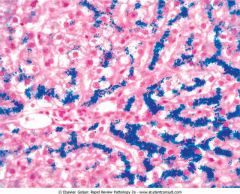
Liver biopsy stained with Prussian blue in a patient with hereditary hemochromatosis
|
|
|
|
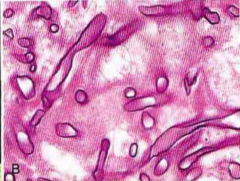
Lung biopsy stained with Gomori methenamine-silver showing septated hyphae and fruiting body (inset) of Aspergillus fumigatus
|

|
|
|
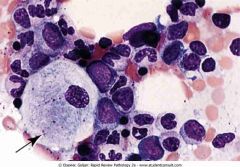
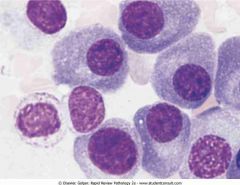
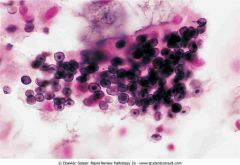
.Malignant plasma cells in multiple myeloma. The majority of malignant plasma cells show a gray-blue cytoplasm, peripherally located nuclei, and perinuclear clearing
|
|
|
|
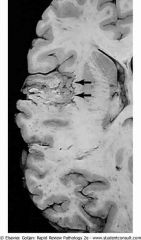
Multiple sclerosis showing multiple areas of demyelinated white matter (arrows pointing to brown plaques)
|
|
|
|
Analgesic nephropathy showing multiple brownish necrotic papillae (arrows)
|

|
|
|
Neonatal respiratory distress syndrome
|
|
|
|
Neurocysticercosis showing multiple cysts between the gray and white matter
|
|
|
|
Optic disk with papilledema showing loss of the disk margin and hard exudates (white streaks
|

|
|
|
Osteoarthritis. Bony protuberances (Heberden's nodes)
|

|
|
|
Patient with myasthenia gravis showing ptosis of the left eye (A) followed by opening of the eye (B) after intravenous injection of Tensilon.
|
|
|
|
Petechiae in idiopathic thrombocytopenic purpura showing pinpoint hemorrhages, a sign of platelet dysfunction
|
|
|
|
Pneumocystis jiroveci pneumonia. This silver-impregnated cytologic smear
|
|
|
|
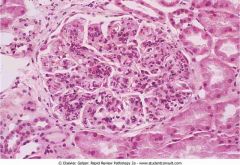
Poststreptococcal diffuse proliferative glomerulonephritis
|
|
|
|
Potassium hydroxide preparation of skin scrapings showing hyphae and yeasts
|

|
|
|
Prostate cancer metastatic to the vertebral column. Multiple white foci of metastatic prostate cancer produce an osteoblastic response in the bone.
|

|
|
|
Radiograph of a skull showing multiple punched out lytic lesions in multiple myeloma
|

|
|
|
Radiograph showing small bowel obstruction.
|

|
|
|
Saddle embolus occluding the main branches of the pulmonary artery
|

|
|
|
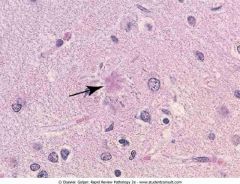
Senile plaque (arrow) shows an eosinophilic center with peripherally located distended neuronal processes (neurites).
|
|
|
|
Silver stain showing Helicobacter pylori organisms.
|
|
|
|
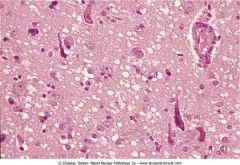
Spongiform encephalopathy in Creutzfeldt-Jakob disease showing classic bubbles and holes of the neuropil cell bodies
|
|
|
|
Subendothelial immunocomplex deposits viewed with electron microscopy.
|
|
|
|
Substantia nigra in a patient with Parkinson disease (A) and a normal individual (B)
|

|
|
|
Tinea capitis due to Trichophyton tonsurans
|

|
|
|
Tinea corporis showing annular lesions with erythematous margins and clear centers
|

|
|
|
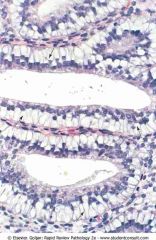
subnuclear vacuoles (arrows) containing mucin push the nuclei of the endometrial cells toward the apex of the cell
|
|
|
|
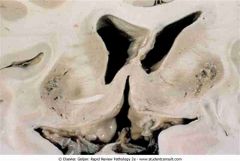
Wernicke's encephalopathy showing hemorrhage and discoloration of mamillary bodies and the wall of the third ventricle
|
|
|
|
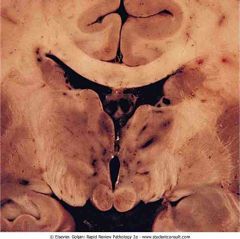
Wilson's disease showing cavitary necrosis of the putamen on both sides of the brain
|
|
|
|
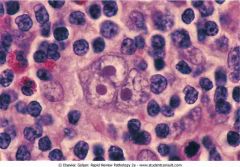
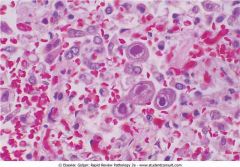
Cytomegalovirus.
The enlarged nuclei of many of the type I pneumocytes contain large inclusions (basophilic staining with hematoxylin and eosin slain) surrounded by a dear halo. "Owl's eye" inclusions in monocytes. |
|
|
|
Type A Cowdry body --> HSV and CMV
|

|
|
|
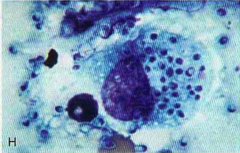
Histoplasma capsulatum.
Alveolar macrophage contains intracellular yeast forms. |
|
|
|
Tonsillitis due to Corynebacterium diphtheriae.
Note the gray, pseudomembrane covering the tonsils |

|
|
|
Gram stain of Streptococcus pneumoniae.
The sputum stain shows numerous lancet-shaped diplococci with the tapered ends pointing to each olher, A few neutrophils conlain phagocytosed bacteria. |

|
|
|
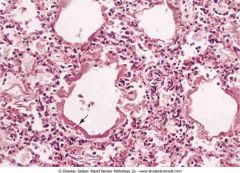
Neonatal respiralory distress syndrome.
Some of the dilated respiralory bronchioles and alveolar ducts are lined with a fibrin-rich membrane (hyaline membrane) (arrow). The subjacent alveoli are collapsed. |
|
|
|
Electron micrograph of a type II pneumocyle showing a lamellar body {arrow) containing surfactant.
|

|
|
|
Cryptococcus.
India ink preparation showing large capsules surrounding budding yeast cells. |

|
|
|
Toxoplasmosis.
Note the cyst (arrow) filled with bradyzoites. |

|
|
|
Ncurocysticercosis.
Note the multiple cysts localcd between the gray and white mater. |

|
|
|
Mucor species (zygo-mycosis).
Note the broad, aseptate hyphae that have wide-angled branching. |
|
|
|
A, Multiple sclerosis, gross appearance. The brain shows multiple areas of demyelinated white mater (arrows pointing to gray-brown plaques).
B, Multiple sclerosis, gross appearance Note the periventricular location for the demyelinating plaques. C, Bilateral internuclear ophthalmoplegia in multiple sclerosis. When the palient is asked to look right, the right eye moves to the right and exhibits jerk nystagmus, while the left eye remains stationary. When the patient is asked to look left, the left eye moves to the left and shows jerk nystagmus, while the right eye remains stationary. These findings are due to bilateral demyelinalion of the medial longitudinal fasciculus. |

|
|
|
Pneumocystisjiroveci pneumonia.
This silver-impregnated cytologic smear prepared from bronchial washings in an HIV- positive patient contains numerous P. jiroveci cysts. Some cysts look like crushed ping-pong balls. |

|
|
|
E, Dermatomyositis. Note the characleristic purple papules overlying the knuckles and proximal and distal interphalan- geal joints.
F, Dermatomyositis. Note the characleristic swelling and red-mauve discoloration below the eyes. |

|
|
|
B, Raynaud's phenomenon: Raynaud's phenomenon in systemic sclerosis is due 10 a digital vasculitis. The usual color changes are white (this patient) to blue lo red. It is one ofthe first signs of systemic sclerosis.
|

|
|
|
C, Systemic sclerosis. The skin is erylhematous and tighlly bound. The fingertips are tapered (called sclerodactyly) and have digital infarcts {arrows) due to fibrosis oflhe digital vessels.
D, Systemic sclerosis. Note the thinned lips and characterislic radial furrowing around the mouth giving a pursed-lip appearance. This is due to increased deposilion of collagen in the subcutaneous lissue. There are also dilatations of small vessels (telangiectasia) on the face. |

|
|
|
Acute myocardial infarction (Ml) showing coagulation necrosis. This section of myocardial lissue is from a 3-day-old acute Ml. The outlines of the myocardial fibers are Intact: however, they lack nuclei and cross-striations. A neutrophilic infiltrate is present between some of the dead fibers.
|

|
|
|
Acute Ml showing a pale infarction ofthe poste- rior wall ofthe left ventricle (bottom left),
|

|
|
|
Hemorrhagic infarclion of lung. There is a roughly wedge-shaped area of hem- orrhage extending to the pleural surface. The arrow shows an embolus in one of the pulmonary artery tributaries.
|

|
|
|
E, Barrett's esophagus showing an extensive area of glandular metaplasia with numerous goblet cells. A small section of squamous epithelium remains on the right.
|

|
|
|
F, Section of bronchus from a smoker showing focal squamous metaplasia (longarrow). Normal ciliated, pseudostratified colum- nar epithelium is presenl on the right (short arrow).
|

|
|
|
D, Fusion ofthe podocytes.
Arrow shows fusion of the podocytes. This finding occurs in all glomerular diseases that present with the nephrotic syndrome (e.g., minimal change disease). |

|
|
|
Diffuse proliferative glomerulonephritis due to systemic lupus erythematosus.
Subendothelial immunocomplex deposits viewed with electron microscopy. The band of electron-dense material extends around the glomerular basement membrane and hugs lhe interface oflhe membrane ivitli the capillary lumen. The arrow poinls to immune deposits direcily beneath the nucleus of the endothelial cell. A thin rim of normal basement membrane (lighl gray) separates the deposits from the epithelial side ofthe membrane. |

|