![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
63 Cards in this Set
- Front
- Back
|
What categories do you need to distinguish between when a patient presents with dizziness? |
- Pre-syncope - Disequilibrium - Vertigo |
|
|
What are the characteristics of "pre-syncope"? |
Feeling light-headed or faint, as opposed to actually passing out. Sometimes they feel worse when they stand up quickly. |
|
|
What are the characteristics of "disequilibrium"? |
A feeling of being off balance |
|
|
What are the characteristics of "vertigo"? |
A sensation of the room spinning |
|
|
What is usually the general cause of pre-syncope (feeling light-headed)? |
Inadequate cerebral perfusion |
|
|
What conditions are associated with pre-syncope? |
- MI - AFib - Tachycardia of thyroid storm - Bradyarrhythmias - Valvular heart disease - Acute blood loss (e.g., gastric ulcer bleed) |
|
|
What is the mechanism by which an MI would cause pre-syncopal symptoms? |
Inadequate cardiac output due to "pump failure" --> inadequate cerebral perfusion --> lightheadedness |
|
|
What is the mechanism by which AFib would cause pre-syncopal symptoms? |
Inadequate cardiac output due to decreased filling time --> inadequate cerebral perfusion --> lightheadedness |
|
|
How should AFib be managed? |
Rate control is achieved through pharmacologic or electric cardioversion or use of CCBs, Beta-Blockers, or Digoxin if cardioversion is contraindicated or ineffective |
|
|
What is the mechanism by which thyroid storm would cause pre-syncopal symptoms? |
Thyroid storm --> tachycardia --> inadequate cardiac output due to decreased filling time --> inadequate cerebral perfusion --> lightheadedness |
|
|
How can you treat tachycardia of thyroid storm? |
Treat the underlying hyperthyroidism and cardiac rate control with beta-blockers |
|
|
What is the mechanism by which bradyarrhythmias would cause pre-syncopal symptoms? |
Inadequate cardiac output due to decreased filling time --> inadequate cerebral perfusion --> lightheadedness |
|
|
How do you treat bradyarrhythmias? |
Often these are caused by medications; treatment is simply withdrawal of the medication
Symptomatic bradyarrhythmias frequently require a pacemaker |
|
|
What is the mechanism by which valvular heart disease would cause pre-syncopal symptoms? |
Inadequate cardiac output due to obstruction --> inadequate cerebral perfusion --> lightheadedness |
|
|
How should you manage valvular heart disease, e.g., aortic stenosis? |
Aortic stenosis is a common valvular lesion in the elderly that may be asymptomatic; however, once syncope develops, valve replacement may be indicated |
|
|
What is the mechanism by which acute blood loss would cause pre-syncopal symptoms? |
1. Inadequate cardiac output due to decreased preload due to volume depletion
2. Poor cerebral oxygenation due to inadequate hemoglobin concentration
--> inadequate cerebral perfusion --> lightheadedness |
|
|
How should you manage a patient with acute blood loss? |
Replace volume and raise hemoglobin concentration |
|
|
What type of dizziness would be caused by cerebellar degeneration (e.g., alcoholism)? How can you manage this? |
Disequilibrium - feeling off balance - Manage: treat underlying pathology; balance rehabilitation PT may benefit some |
|
|
What type of dizziness would be caused by amino glycoside toxicity? |
Vertigo / hearing loss, feels like the room is spinning |
|
|
What type of dizziness would be caused by peripheral neuropathy? |
Disequilibrium - feeling off balance due to loss of sensation and position sense |
|
|
What is the definition of orthostatic hypotension? |
- Drop in systolic BP of ≥20 mmHg OR - Drop in diastolic BP of ≥10 mmHg
- Occurs when changing position from supine to standing - Accompanied by feelings of dizziness or lightheadedness |
|
|
Mrs. Saleh is a 28-year-old woman with a recent upper respiratory infection who presents with acute onset constant, non-positional vertigo with associated nausea and vomiting. On exam she has normal orthostatic vital signs, normal hearing, a positive Romberg test, and left horizontal nystagmus that resolves with gaze fixation and does not change with direction of gaze.
What are the top 3 differential diagnoses? |
- Vestibular neuritis - Benign paroxysmal positional vertigo (BPPV) - Vestibular migraine |
|
|
What cause of vertigo is commonly associated with a recent URI? |
Vestibular neuritis |
|
|
What are the characteristics of vestibular neuritis? |
Cause of vertigo: - Commonly associated with a recent URI - Nystagmus caused by a peripheral lesion such as this does not change direction with gaze |
|
|
What does benign paroxysmal positional vertigo (BPPV) cause symptom-wise? |
- Acute onset vertigo, episodic (rather than constant) - May be associated with nausea / vomiting - Intact hearing |
|
|
What causes the vertigo in benign paroxysmal positional vertigo (BPPV)? |
- Calcium carbonate debris in the semicircular canals - During positional changes the calcium debris moves - Symptoms usually resolve several seconds to minutes following positional changes |
|
|
What is the definition of a vestibular migraine? |
Migraine variant that can cause central vertigo; most patients will have a history of migraines but at the time of the vertigo (vestibular migraine), many do not have a headache |
|
|
How can you categorize the causes of vertigo? |
Central vs peripheral |
|
|
What is the location of pathology in cases of peripheral vertigo? |
Problems with the inner ear or vestibular system |
|
|
What is the location of pathology in cases of central vertigo? |
CNS tends to be more serious conditions than peripheral lesions |
|
|
What are the characteristics of nystagmus in peripheral vertigo? |
- Unidirectional (usually horizontal and rotational) and does not change direction - Inhibited by fixating on a point and intensifies when fixation is withdrawn - Frenzel glasses prevent fixation and bring out the nystagmus |
|
|
What are the characteristics of nystagmus in central vertigo? |
- Purely horizontal, vertical, or rotational - Does not lessen when the patient focuses gaze - Persists for a longer period |
|
|
What kind of lesion causes a nystagmus that is inhibited by fixating on a point but intensifies when fixation is withdrawn? |
Peripheral lesion |
|
|
What kind of lesion causes a nystagmus that does not lessen when the patient focuses their gaze? |
Central lesion |
|
|
What kind of glasses prevent fixation? How does this help you determine the location of the lesion causing nystagmus? |
Frenzel glasses - prevent fixation - brings out the nystagmus in peripheral lesions |
|
|
What symptoms would a patient with a cerebellar infarct have? |
- Ataxia - Dysmetria - Disequilibrium |
|
|
What is the disease that causes the triad of unilateral hearing loss, tinnitus, and vertigo? |
Meniere's disease |
|
|
What are the symptoms of Meniere's disease? |
- Unilateral hearing loss - Tinnitus - Vertigo |
|
|
Mrs. Saleh is a 28-year-old woman with a recent upper respiratory infection who presents with acute onset constant, non-positional vertigo with associated nausea and vomiting. On exam she has normal orthostatic vital signs, normal hearing, a positive Romberg test, and left horizontal nystagmus that resolves with gaze fixation and does not change with direction of gaze.
Why is a transient ischemic attack an unlikely cause of her symptoms? |
TIA can cause symptoms of vertigo but these should not be constant. In addition, the resolution of nystagmus with gaze fixation argues for a peripheral rather than central lesion. |
|
|
Mrs. Saleh is a 28-year-old woman with a recent upper respiratory infection who presents with acute onset constant, non-positional vertigo with associated nausea and vomiting. On exam she has normal orthostatic vital signs, normal hearing, a positive Romberg test, and left horizontal nystagmus that resolves with gaze fixation and does not change with direction of gaze.
Why does she most likely have a vestibular neuritis or acute labyrinthitis? |
- Constant symptoms of vertigo - Vertigo is unrelated to position - Signs of a peripheral lesion (nystagmus that stops with fixation) - Normal neurological exam (other than nystagmus/vertigo) - Symptoms occurred shortly after a viral URI |
|
|
What is the most common cause of vertigo in primary care? |
Benign Paroxysmal Positional Vertigo (BPPV) |
|
|
What is the second most common cause of vertigo in primary care? |
- Vestibular neuritis - Acute labyrinthitis |
|
|
What is the cause of vestibular neuritis? |
Viral (or, less commonly, bacterial) infection of the inner ear causes inflammation of the vestibular branch of the 8th cranial nerve --> vertigo (w/o hearing loss and/or tinnitus) |
|
|
What is the cause of acute labyrinthitis? |
Viral (or, less commonly, bacterial) infection of the inner ear causes inflammation of the both branches of the 8th cranial nerve --> tinnitus and/or hearing loss + vertigo |
|
|
How can you confirm the diagnosis of benign paroxysmal positional vertigo (BPPV)? |
Dix-Hallpike Maneuver |
|
|
What is the Dix-Hallpike Maneuver? |
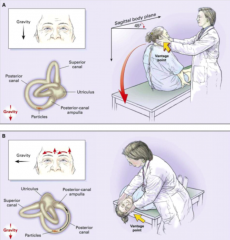
- Turn the patient's head to 45 degrees and quickly lay him down supine with his head just over the end of the exam table - Turn the head to the side which should reproduce the symptoms of dizziness and produce nystagmus - Observe for 20-30 seconds; if present, the nystagmus will have the fast component in the direction of the pathology - Sit the patient up and observe again for nystagmus |
|
|
Is there neuroimaging to confirm vestibular neuritis or BPPV? |
No - you diagnose them both based on clinical information
But if you are considered a potentially life-threatening CENTRAL cause of vertigo (e.g., cerebellar infarct or TIA) then you would do further testing - MRI is the best |
|
|
What physical exam maneuver can be used to differentiate between peripheral and central vertigo? |
Head Thrust Test (used to demonstrate a likely peripheral lesion) |
|
|
What do you do in the Head Thrust Test? |
- Ask them to keep looking at your nose - His eyes will stay fixed on your nose if you move his head suddenly to the side - If there is a peripheral lesion in the vestibular system, the vestibular ocular reflex will be disrupted and his eyes will move with the head and then saccade back to center (when the head is moved in the direction of the lesion) - A normal head thrust test in the presence of vertigo means the peripheral vestibular system is intact and the lesion is central |
|
|
Does the following patient need imaging?
A 68-year old woman with a history of HTN and sudden acute onset constant vertigo. She has right nystagmus that changes direction with gaze and does not appear when she focuses. |
Yes - there are multiple reasons to be concerned about a central lesion and a possible infarct. Her age puts her at risk as does her HTN. Her exam shows nystagmus that changes direction and does not inhibit with focus. Both of these are consistent with a central lesion. She needs an urgent MRI. |
|
|
Does the following patient need imaging?
A 45-year old man with recurrent episodes of brief intense vertigo every time he turns his head rapidly. He has no other neurologic signs of symptoms. He has a positive Dix-Hallpike maneuver. |
No - this patient has a classic history of benign paroxysmal positional vertigo (BPPV). In addition, the positive Dix-Hallpike maneuver confirms the diagnosis. Neuroimaging is not required. |
|
|
Does the following patient need imaging?
A 66-year old man with recurrent episodes of vertigo associated with tinnitus and hearing loss. His head thrust is positive. |
No - the triad of recurrent episodes of vertigo, tinnitus, and hearing loss is characteristic of Meniere's disease which is a peripheral lesion. A positive head thrust test reassures that the lesion is peripheral. |
|
|
Does the following patient need imaging?
A 28-year old otherwise well woman with new onset constant vertigo with no other neurological symptoms. On exam, she has unidirectional nystagmus that disappears when her gaze is fixed. |
No - unidirectional nystagmus that disappears with fixation and recurs with loss of fixation implies a peripheral lesion. In the absence of other neurological signs and symptoms in an otherwise well young woman, neuroimaging is not needed since the likelihood of a central lesion is minimal. |
|
|
Does the following patient need imaging?
A 40-year old woman with history of migraine and new onset headache with constant, non-positional vertigo. Her head thrust test displays a normal response. |
Yes - a normal head thrust test in the face of constant and new vertigo combined with a history of migraines indicates a possible central lesion. Neuroimaging is needed. |
|
|
Mrs. Saleh has left-beating nystagmus that disappears when she fixes on a foal point and recurs when she loses the focal point. Head thrust test is positive.
What is the likely diagnosis? What needs to be done for a patient with this diagnosis? |
Vestibular neuritis - she does not need further testing at this time. Symptoms will likely improve over the next couple of days to a week. |
|
|
What treatments can be given for a patient with peripheral vertigo? |
- Diuretics - Epley maneuvers - Vestibular rehab exercises - Vestibular suppressant meds |
|
|
What medication can be used to treat Meniere's disease? |
Diuretics and low salt diet --> reasoning that diuretics will decrease the endolymphatic pressure and abate symptoms (but a Cochrane review in 2006 found no trials of high enough quality to recommend for or against diuretics) |
|
|
What is the mainstay of treatment for benign paroxysmal positional maneuver? |
Epley maneuver or canalith repositioning |
|
|
What is the etiology of vertigo in BPPV? |
Calcium debris in the semicircular canals |
|
|
What is the purpose of the Epley maneuver for patients with BPPV? |

Relieves symptoms by returning the deposits back to the vestibule
For right-sided symptoms: - Patient sits on table with head turned 45 degrees to right - Clinician supports the head, patient quickly lies back with head hanging over table - Once nystagmus stops clinician turns head 90 degrees to left and position is held for 30 seconds - Patient rolls onto left side, with his face at a 45 degree angle to floor, hold position for 30 seconds - Patient returns to sitting with legs off left edge of table, hold position for 30 seconds - Resume normal head position |
|
|
What are medications that can suppress the vestibular system? Uses? |
Effective short-term treatments of vertigo: - Anti-cholinergic vestibular suppressants: Meclizine, Dimenhydrinate
Non-selective phenothiazine anti-emetics: Metoclopramide, Promethazine |
|
|
What are the names of the anti-cholinergic vestibular suppressants? |
- Meclizine - Dimenhydrinate |
|
|
What are the names of the non-selective phenothiazine anti-emetics that can be effective in patients with nausea/vomiting associated with vertigo? |
- Metoclopramide (Reglan) - Promethazine |