![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
67 Cards in this Set
- Front
- Back
|
What are the characteristics of Hepatic Steatosis? |
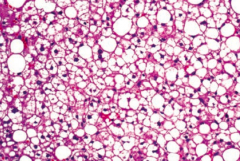
- First stage in alcoholic liver disease |
|
|
What are the characteristics of Alcoholic Hepatitis?
|
- Second stage in alcoholic liver disease
- Requires sustained, long-term consumption of alcohol - Swollen and necrotic hepatocytes with neutrophilic infiltration - Mallory bodies (intracytoplasmic eosinophilic inclusions) are present - AST > ALT (ratio usually >1.5) |
|
|
What are the characteristics of Alcoholic Cirrhosis?
|
- Final stage of alcoholic liver disease
- Irreversible changes - Micronodular, irregularly shrunken liver with "hobnail" appearance - Sclerosis around central vein (zone III) - Has manifestations of chronic liver disease (eg, jaundice, hypoalbuminemia) |
|
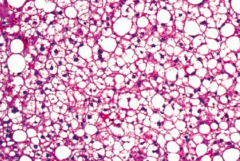
When might you see macrovesicular fatty change in the liver?
|
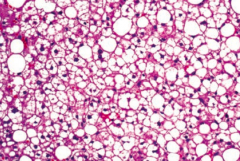
Macrovesicular fatty change is a sign of hepatic steatosis (stage 1 of alcoholic liver disease); reversible with alcohol cessation
|
|
|
When might you see swollen and necrotic hepatocytes with neutrophilic infiltration and Mallory bodies? |
Alcoholic Heptitis (stage 2 of alcoholic liver disease)
- Mallory Bodies: intracytoplasmic eosinophilic inclusions |
|
|
When might you see a micronodular with a "hobnail" appearance? |
Alcoholic cirrhosis (stage 3 of alcoholic liver disease); irreversible and final form
|
|
|
Where is there sclerosis in the liver with alcoholic cirrhosis?
|
Around the central vein (zone III)
|
|
|
What causes non-alcoholic fatty liver disease? What changes happen?
|
Metabolic syndrome (insulin resistance) → fatty infiltration of hepatocytes → cellular "ballooning" and eventual necrosis
ALT > AST (lipids) (independent of alcohol use) |
|
|
What can non-alcoholic fatty liver disease lead to?
|
May cause cirrhosis and hepatocellular carcinoma
|
|
|
What causes hepatic encephalopathy?
|
Cirrhosis → portosystemic shunts → ↓ NH3 metabolism → neuropsychiatric dysfunction
|
|
|
How severe is hepatic encephalopathy?
|
Spectrum from disorientation / asterixis (mild) to difficult arousal or coma (severe)
|
|
|
What an trigger hepatic encephalopathy?
|
- ↑ NH3 production: dietary protein, GI bleed, constipation, infection
- ↓ NH3 removal: renal failure, diuretics, post-TIPS |
|
|
What can lead to ↑ NH3 production? Implications?
|
- Dietary protein
- GI bleed - Constipation - Infection - Can be a trigger for hepatic encephalopathy |
|
|
What can lead to ↓ NH3 removal? Implications?
|
- Renal failure
- Diuretics - Post-TIPS (Transjugular Intrahepatic Portosystemic Shunt) |
|
|
How do you treat patients with hepatic encephalopathy?
|
- Lactulose (removes NH3 by converting to NH4+)
- Low protein diet - Rifaximin (kills intestinal bacteria) |
|
|
What is the most common 1° malignant tumor of the liver in adults?
|
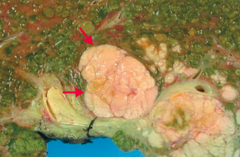
Hepatocellular Carcinoma (HCC)
|
|
|
What is Hepatocellular Carcinoma (HCC) associated with?
|
- Hepatitis B & C
- Wilson disease - Hemochromatosis - α1-antitrypsin deficiency - Alcoholic cirrhosis - Aflatoxin from Aspergillus (carcinogen) |
|
|
What can Hepatocellular Carcinoma (HCC) lead to?
|
Budd-Chiari Syndrome
- Caused by occlusion of the hepatic veins that drain the liver - Presents with the classical triad of abdominal pain, ascites and hepatomegaly |
|
|
What are the findings in patients with Hepatocellular Carcinoma?
|
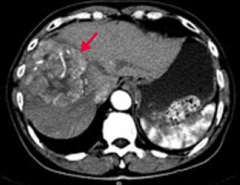
- Jaundice
- Tender hepatomegaly - Ascites - Anorexia - May lead to Budd-Chiari Syndrome |
|
|
How do you diagnose Hepatocellular Carcinoma (HCC)?
|
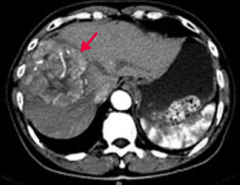
- ↑ α-Fetoprotein
- Ultrasound - Contrast CT (enhancing heterogenous mass) |
|
|
How does Hepatocellular Carcinoma (HCC) spread?
|
Hematogenously
|
|
|
What are the liver tumors?
|
- Hepatocellular Carcinoma (most common)
- Cavernous Hemangioma - Hepatic Adenoma - Angiosarcoma |
|
|
What is the common, benign liver tumor that typically occurs at age 30-50 years?
|
Cavernous Hemangioma
|
|
|
What is the rare, benign liver tumor, often related to oral contraceptive or anabolic steroid use?
|
Hepatic Adenoma
|
|
|
What is the malignant liver tumor of endothelial origin associated with exposure to arsenic and vinyl chloride?
|
Angiosarcoma
|
|
|
What are the characteristics of Cavernous Hemangioma?
|
- Common, benign liver tumor
- Typically occurs at age 30-50 years - Biopsy contraindicated because of a risk of hemorrhage |
|
|
What are the characteristics of Hepatic Adenoma?
|
- Rare, benign liver tumor
- Often related to oral contraceptive or anabolic steroid use - May regress spontaneously or rupture (abdominal pain and shock) |
|
|
What are the characteristics of Angiosarcoma?
|
- Malignant tumor of endothelial organ
- Associated with exposure to arsenic and vinyl chloride |
|
|
What causes the liver to have a "nutmeg" appearance?
|
- Backup of blood into liver
- Commonly caused by R-sided heart failure and Budd-Chiari Syndrome - Appears mottled by a nutmeg |
|
|
What can nutmeg liver progress to?
|
If the condition persists, centrilobular congestion and necrosis can result in cardiac cirrhosis
|
|
|
What causes Budd-Chiari Syndrome?
|
Occlusion of IVC or hepatic vein with centrilobular congestion and necrosis
|
|
|
What does Budd-Chiari Syndrome lead to?
|
- Congestive liver disease → hepatomegaly, ascites, abdominal pain, and eventual live failure
- May develop varices - May have visible abdominal and back veins |
|
|
What is Budd-Chiari Syndrome associated with?
|
- Hypercoagulable states
- Polycythemia vera - Pregnancy - Hepatocellular Carcinoma (HCC) - Absence of JVD |
|
|
How does α1-antitrypsin deficiency cause liver damage?
|
Misfolded gene product protein aggregates in hepatocellular ER → cirrhosis
|
|
|
What is the histologic finding of α1-antitrypsin deficiency in the liver?
|
Cirrhosis with PAS (+) globules (made of aggregations of misfolded gene product)
|
|
|
How do you inherit α1-antitrypsin deficiency?
|
Codominant trait
|
|
|
How does α1-antitrypsin deficiency affect other organs besides the liver?
|
In lungs, ↓ α1-antitrypsin → uninhibited elastase in alveoli → ↓ elastic tissue → panacinar emphysema
|
|
|
What causes jaundice?
|
- Bilirubin deposition in the skin and/or sclera causing yellowing
- Occurs at high bilirubin levels (>2.5 mg/dL) in the blood 2° to ↑ production or defective metabolism |
|
|
How high does bilirubin need to be to cause jaundice?
|
>2.5 mg/dL in blood
|
|
|
What are the types of hyperbilirubinemia?
|
- Unconjugated (indirect) hyperbilirubinemia
- Conjugated (direct) hyperbilirubinemia - Mixed (direct and indirect) hyperbilirubinemia |
|
|
What is the level of urine urobilinogen in unconjugated (indirect) hyperbilirubinemia? What diseases have this finding? |
- Increased urine urobilinogen
- Diseases: hemolytic, physiologic (newborns), Crigler-Najjar, Gilbert syndrome |
|
|
What is the level of urine urobilinogen in conjugated (direct) hyperbilirubinemia? What diseases have this finding? |
- Decreased urine urobilinogen
Diseases: - Biliary tract obstruction: gallstones, pancreatic liver cancer, liver fluke - Biliary tract disease: 1° sclerosing cholangitis and 1° biliary cirrhosis - Excretion defect: Dubin-Johnson syndrome, Rotor syndrome |
|
|
What is the level of urine urobilinogen in mixed (direct and indirect) hyperbilirubinemia? What diseases have this finding?
|
- Normal or ↑
- Diseases: hepatitis or cirrhosis |
|
|
What type of hyperbilirubinemia is seen in patients with hemolysis?
|
Unconjugated (indirect) hyperbilirubinemia
- ↑ urine urobilinogen |
|
|
What type of hyperbilirubinemia is seen in newborns?
|
Physiologic (don't have enzymes to convert to conjugated form)
- Unconjugated (indirect) hyperbilirubinemia - ↑ urine urobilinogen |
|
|
What type of hyperbilirubinemia is seen in patients with Crigler-Najjar syndrome?
|
Unconjugated (indirect) hyperbilirubinemia
- ↑ urine urobilinogen |
|
|
What type of hyperbilirubinemia is seen in patients with Gilbert syndrome?
|
Unconjugated (indirect) hyperbilirubinemia
- ↑ urine urobilinogen |
|
|
What type of hyperbilirubinemia is seen in patients with a biliary tract obstruction? What can cause this?
|
Causes of biliary tract obstruction:
- Gallstones - Pancreatic liver cancer - Liver fluke Conjugated (direct) hyperbilirubinemia - ↓ urine urobilinogen |
|
|
What type of hyperbilirubinemia is seen in patients with a biliary tract disease? What can cause this?
|
Causes of biliary tract disease:
- 1° sclerosing cholangitis - 1° biliary cirrhosis Conjugated (direct) hyperbilirubinemia - ↓ urine urobilinogen |
|
|
What type of hyperbilirubinemia is seen in patients with an excretion defect? What can cause this?
|
- Dubin-Johnson Syndrome
- Rotor Syndrome Conjugated (direct) hyperbilirubinemia - ↓ urine urobilinogen |
|
|
What type of hyperbilirubinemia is seen in patients with hepatitis and cirrhosis?
|
Mixed (direct and indirect) hyperbilirubinemia
- Normal or ↑ urine urobilinogen |
|
|
What is the most common cause of jaundice in a neonate?
|
Physiologic Neonatal Jaundice
- At birth, immature UDP-glucuronosyltrasnferase --> unconjugated hyperbilirubinemia --> jaundice / kernicterus |
|
|
How do you treat a neonate with physiologic jaundice?
|
Phototherapy (converts unconjugated bilirubin to water-soluble form
|
|
|
Which hereditary hyperbilirubinemia is associated with mildly DECREASED UDP-glucuronosyltransferase conjugation activity? What does this lead to?
|
Gilbert Syndrome
- Decreased bilirubin uptake by hepatocytes - Asymptomatic or mild jaundice (no clinical consequences) - Elevated unconjugated bilirubin without overt hemolysis - Bilirubin increases with fasting and stress |
|
|
Which hereditary hyperbilirubinemia is associated with ABSENT UDP-glucuronosyltransferase conjugation activity? What does this lead to?
|
Crigler-Najjar Syndrome (type I)
- Presents early in life, patients die within a few years - Causes jaundice, kernicterus (bilirubin depostion in brain), and ↑ unconjugated bilirubin |
|
|
Which hereditary hyperbilirubinemia is associated with a black liver? Why?
|
Dubin-Johnson Syndrome
- Conjugated hyperbilirubinemia is due to defective liver excretion - Benign |
|
|
Which hereditary hyperbilirubinemia causes a mild conjugated hyperbilirubinemia but without turning th eliver black?
|
Rotor Syndrome
|
|
|
Which syndrome causes bilirubin to increase with fasting or stress? Consequences?
|
Gilbert Syndrome
- Mildly ↓ UDP-glucuronosyltransferase conjugation activity - Leads to ↓ bilirubin uptake by hepatocytes - Can be asymptomatic or cause mild jaundice - Elevated unconjugated bilirubin without overt hemolysis |
|
|
What is wrong in Gilbert Syndrome? Symptoms? Other characteristics?
|
- Very common, no clinical consequences
- Mildly ↓ UDP-glucuronosyltransferase conjugation activity - Leads to ↓ bilirubin uptake by hepatocytes - Can be asymptomatic or cause mild jaundice - Elevated unconjugated bilirubin without overt hemolysis - Bilirubin ↑ with fasting and stress |
|
|
What is wrong in Crigler-Najjar Syndrome, type 1? Symptoms? Other characteristics?
|
- Absent UDP-glucuronosyltransferase
- Presents early in life, patients die within a few years - Findings: jaundice, kernicterus (bilirubin deposition in brain), ↑ unconjugated bilirubin - Treat with plasmapheresis and phototherapy |
|
|
What is wrong in Crigler-Najjar Syndrome, type 2? Symptoms? Other characteristics?
|
- Type 2 is less severe
- Responds to phenobarbital which ↑ liver enzyme synthesis |
|
|
What is wrong in Dubin-Johnson Syndrome? Symptoms? Other characteristics?
|
- Conjugated hyperbilirubinemia
- Due to defective liver excretion - Grossly black liver - Benign |
|
|
What is wrong in Rotor Syndrome? Symptoms? Other characteristics?
|
- Similar to Dubin-Johnson Syndrome (problem with liver excretion of bilirubin)
- Mild conjugated hyperbilirubinemia - Even milder, and doesn't cause black liver |
|
|
What does hemoglobin get converted to during its destruction? Where?
|

Bilirubin - takes place in hepatic sinussoid
|
|

Which hereditary syndromes cause a problem with bilirubin uptake and conjugation (1)? Leads to?
|

Gilbert Syndrome
- Leads to unconjugated bilirubinemia |
|

Which hereditary syndromes cause a problem with bilirubin conjugation (2)? Leads to?
|

Crigler-Najjar Syndrome
- Leads to unconjugated bilirubinemia |
|

Which hereditary syndromes cause a problem with conjugated bilirubin excretion (3) and (4)? Leads to?
|

Dubin-Johnson Syndrome
- Leads to conjugated hyperbilirubinemia Rotor Syndrome - Leads to MILD conjugated hyperbilirubinemia |