Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
13 Cards in this Set
- Front
- Back
Clinical Dystrophic EB
|

|
|
|
Inheritance
|
Dominant dystrophic epidermolysis bullosa (DDEB) autosomal dominant; COL7A 1 gene on 3p2l
Recessive dystrophic epidermolysis bullosa (RDEB) autosomal recessive; COL7A I gene on 3p2l |
|
|
Prenatal
|
DNA analysis
Chorionic villus sampling/ amniocentesis analysis of fetal cells |
|
|
Incidence
Age at Presentation |
Approximately 2.5 cases per million live births in the United States. (DDEB more common than RDEB); M=F
DDEB birth to early infancy RDEB birth |
|
|
Pathogenesis
|
Mutations in the COL7A 1 gene responsible for type VII collagen formation, the main structural protein in anchoring fibrils, disrupts the integrity of the dermal epidermal junction; structurally defective and reduced numbers of anchoring fibrils contribute to phenotype
|
|
|
Pathogenesis
|
RDEB Hallopeau Siemens subtype
more severe phenotype secondary to premature termination codon mutations causing lack of anchoring fibrils RDEB non Hallopeau Siemens subtype less severe phenotype secondary to missence or frameshift mutations in COL7AI producing defective anchoring fibrils DDEB less severe phenotype secondary to glycine substitutions that impact upon the triple helix assembly of type 7 collagen |
|
|
Clinical DDEB
|
DDEB
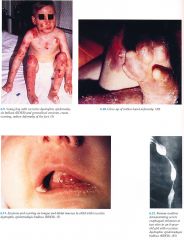
Skin Bullae can be localized to extremities or widespread; healing with/without milia, scar; mild oral disease; with/without albopapuloid lesions hypopigmented scar¬like papules increased on trunk Nails Dystrophic to absent |
|
|
Clinical RDEB Hallopeau Siemens Type
|
RDEB (Hallopeau Siemens) Skin Generalized bullae with erosions healing with atrophic scarring, hyper/hypopig¬entation, milia; squamous cell carcinoma may occur within scars
Nails Marked dystrophy with loss Musculoskeletal Digital fusions and "mitten" deformities of hands and feet secondary to repeated episodes of blistering and scarring; flexural contractures of knees, elbows, wrists; short stature secondary to malnutrition Mucous Membranes Oral/pharyngeal/laryngeal erosions with scarring, pain on eating, hoarse voice; esophageal erosions with strictures/stenosis; anal erosions with pain on defeca¬tion/fecal impaction; conjunctival]/comeal erosions with conjunctivitis/keratitis, scarring/visual loss (less common); genitourinary scarring Teeth Dysplastic, caries Hematologic Multifactorial anemia |
|
|
Clinical RDEB non-Hallopeau Siemens Type
|
RDEB non Hallopeau Siemens sskin changes localized to acral bony prominences and fragility improves in adulthood; may be indistinguishable from DDEB; all other RDEB findings can occur but less severe
|
|
|
DDx
|
Other forms of EB
Epidermolytic hyperkeratosis Congenital erythropoietic porphyria Staphylococcal scalded skin syndrome Congenital syphilis Neonatal HSVbullous impetigo |
|
|
Lab
|
Bacterial/viral cultures
Skin biopsy for light, electron microscopy; immunomapping; low threshold for skin biopsy to rule out squamous cell carcinoma DNA analysis |
|
|
Management
|
See EBS
Referral to symptom specific subspecialist Referral to nutrition ist vitamin, iron, protein supplementation, soft foods, mineral oil for chronic constipation Referral to surgeons repair mitten deformity, esophageal stenosis, excision of squamous cell carcinoma Referral to dentist soft toothbrush, pulsating water for hygiene Systemic corticosteroids, phenytoin, retinoids, with only anecdotal success |
|
|
describe stage D HF
|
End-stage disease who requires specialized treatment strategies such as mechanical circulatory support, continuous inotropic infusions, cardiac transplantation, or hospice care
|