![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
98 Cards in this Set
- Front
- Back
|
Top Prescribed Drug : Age abused: |
Hydrocodon/APAP = Vicodin Oycodon/APAP= Percocet Young- mid adult 25-40 |
|
|
AAPCC-TESS
|
AmericanAssociation of Poison Control Centers-Toxic Exposure Surveillance System
Children less than 6 compose 50% of cases |
|
|
Elderly tend to have toxicities because of |
Polypharmacy/confuse product and instruction |
|
|
Toxicokinetics- how drugs get into our body and what happens when its in our body. Toxicokinetics of TCAD and AChergics |
Slow absorption due to slow GI motility
|
|
|
Toxidrome: Anticholinergic |
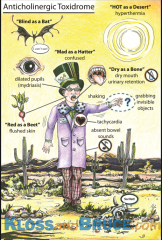
delirium
hyperthermia red as a beet, mad as a hatter, dry as a bone , blind as a bat, hot as a hare ileus mydriasis tachycardia urinaryretention warmdry skin |
|
|
Toxidrome: Cholinergic |
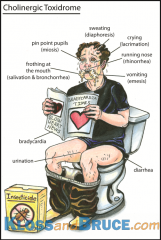
Change in mental status Brady cardia Meiosis bronchorrhea diarrhea salivation lacrimation urnination gi cramps |
|
|
Ipecac do we use? HOw long does it work? Contraindications Gastric lavage: |
ipecac is not used anymore - Used within 1 hour of ingestion(Gastric Lavage also 1 hour) /works within 15-30 min -DO NOT USE IN pts withOUT gag reflex, children under 6 months, pts who ingested sharp objects -patients who will be unresponsive SE for gastric lavage : Aspirational Pneumonia |
|
|
Activated Charcoal |
ADsorption prevents ABsorption Given in first 1-2 hours Reduces half life |
|
|
Beta blocker/ CCB antidote |
Glucagon |
|
|
Anticholinesterase |
Atropine |
|
|
Digoixin |
Digibind |
|
|
Dimercaperol/ Penicilinamine |
Heavy metal poison |
|
|
Calcium EDTA ; succimer |
Lead |
|
|
Biotransformation Phase 1 vs phase 2 |
Phase one oxidized or demethylated by CYP 450 Phase 2 made more polar or water soluble by conjugation -glucoronic acid via glucoronyl transferase -glutathione via glutahione s - transferase - sulfate - sulfotransferase |
|
|
CYP 450 major enzyme responsible for drug metabolism and production of potentially toxic metabolism T/F |
tru |
|
|
METABOLISISM Phase 1 does drug toxification Phase 2 does drug ______ |
Detoxification via phase 2 GSH transferases and glucoronidases If not detoxified by phase 2 it will cause hepatic injury |
|
|
Liver resistant yet vulnerable how ? How do toxins effect the liver? |
-covalent binding to proteins and reactive toxic metabolite -Creation of oxidative stress -Stimulation of an immune attack |
|
|
Acetaminophen toxicity epidemiology |
second most common cause of liver transplant in US |
|
|
CYP2E1 makes NAPQI from APAP metabolism . Its toxic but normally doesnt hang out very long because ? |
active metabolite NAPQI takes 0= and covalently binds to hepatocytes. It is usually conjugated to water soluble metabolites and excreted. Three things happen thats stops that. |
|
|
What three things occur that stop APAp from becoming excreted and more toxic |
1. too much APAP, exceeds capacity to go through phase 2 transformation which is preferred 2.Induction of phase 1 cyp2E1 by alcohol. Alcohol inducts 2E1 and makes it metabolize more and more APAP leaving us with more dangerous NAPQI 3. Your malnourished. Dont have enough glutothione which is rich in cytosine, 4 g ceiling amount of apap. Cimetidine is also used its a 2e1 blocker. |
|
|
Toxic dose of APAP children and adults |
Children: 140mg/kg Adult: 4g normal strength. XR is 3g 10g can deplete glutothionie storage in one day |
|
|
APAP toxicity timeline |
first 24 hours - "honeymoon phase" NVD but feel o.k day 2 : start to have liver failure --> you will see lab changes in liver enzymes, they will rise rise and then drop day 3: look at ALbumin(made by liver) and bilirubin (conjugated in liver)Pt will be jaundice and inr will be crazy because liver cant make conjugation factors. Ammonia levels will be raised and will cross BBB this causes enephalopathy or HEPATIC COMA coma caused by liver failure or mess up . body will go into multiple system failure |
|
|
Nomogram tells us serum of APAP useful in what kind of patients APAP toxidrome |
self harm patients . if apap level is 300 example we will treat them |
|
|
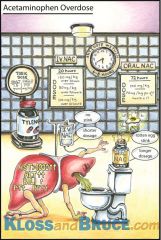
Antidote - N-acetylcysteine- how does it work how do we dose |
serves as a sulfhydryl group subsituting in for glutothione . It conjugates then excretes in urine. Dose 1: DIRNK 140mg/kg mixed in soda or juice THEN WE DO HALF Dose2: then DRINK 70mg/kg q4h X 17 doses can use nacetyl off lable as IV with micropore filtration 300mg/kg NOW FDA approved: aCEtadote brand IV LD: 150mg/kg over 15 min MD: 50 mg/kg over 4 hours then count infusion of 100 mg/kg over 16 hours USE Acetadote for more serious cases of APAP OD |
|
|
Vicodin (hydrocodon + APAP) is now a schedule FDA wants to unbundle APAP combos in drugs Darvacet was removed and replaced with? Infant tylenol became 1 standard concentration. |
2 before was 3 tramadol |
|
|
FDA wants to recommend : |
DC COMBO apap drugs with more than 325 mg |
|
|
ASA or ASPRIN used to be #1 form of toxicity because of direct GI irritation , stimulation of cns respirartory centers. patients used to get |
respiratory alkalosis tehn metabolic acidosis methylsalicylate is topical ASA (aspercreme) also called oil of winter green |
|
|
Respirartory acidosis -->Metabolic acidosis --> interfares with coagulation factors. What are the Blood gas levels that lead to each? |
Respiratory alkalosis first (pCO2 < 35 mmHg,
Metabolic acidosis (HCO3< 18 mmol/L or B.E. < minus 4.0 mEq/L, pH < 7.35) direct stimulation of CNS respiratory , increase depth of respiration, increase bicarbonate excretion Direct irritation of GI |
|
|
How dos asa affect cns respiratory centers in brain? |
It uncouples mitochondrial oxidative phosphorylation as toxicity progresses you have uncoupling so you are unable to generate ATP. Body goes into anaerobic state and cells begin to die. increase in glucose utilization. body use so much glucose that it has to tap into fat stores and then we have an accumulation of KETO acids. and we trip into metabolic keto acidoisis. METABOLISISM IS INCREASED! o2 consumption , glucose utilization and co2 and heat production CNS deteriorates because no atp is around so we have a build up of lactic and pyruvic acid |
|
|
Explain increase demand for Glucose in ASA toxicity inhibit key enzymes with kreb cycle volume depletion- water electrolyte disturbance inhibit hepatic synthesis of clotting factors look out for tinnitus with ASA toxicity t/f?
|
1. form keto acids /cns deterioration 2. inhibit key enzymes with krebs cycle . increase levels of pyruvate and lactate 3. insensbible water loss / vomit / electrolyte disturbance Inhibit hepatic synthesis of clotting factors as well as ASA blocking of platlet aggregation |
|
|
Toxidrome |
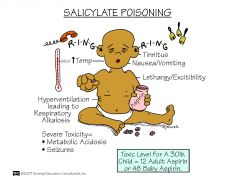
Hyper ventilate Hyper thermia -- mental: agitation/CONFUSI?ON/lethargy/coma -- Symptoms: tinnitus/NV --- PExam: diaphoresis/tender abdomen -- Lab anion gap metabolic acidosis respiratory alkalosis abnormal coagulation studies |
|
|
Treat with activated charcoal(sorbitol wont work for EC.) Gastric Lavage and whole bowel irrigation. saliene Diuresis and urninary alklization. monitor for sodium and fluid retention also pulmonary edema . this ocurs if you give it too fast (sodium bicarb) Use D5W for the drip if pt is hypoglycemic. What about HD? |
Hemodyalisis for patients whos serum level is : 1. over 120 in acute situation 2. greater than 100 6 hours of ingestion 3. OR 60 or more in chronic toxicity |
|
|
TCA toxicity kills you the fastest or slowest? - Amytriptilline:?BRAND -Nortripylene: ? BRAND pamela/ pamelor |
Fastest because it has a large volume of distribution and is VERY protein bound. 1. Elavil 2. Pamel-or |
|
|
What leads to fatalities with TCA overdose? TCA is associated with three combos of toxidromes, name them. 1. 2. 3. |
QRS PROLoNGATION Cardiac arrhythmia : Prolonged QRS complex with interventricular conduction delay which is called Branch block Alpha adrenergic blockage: Patient also has HyPOtension due to vascular alpha adrenergic receptors ANticholinergic symptoms : red a a beet, blind as a bat (dialated pupils), mad as a hatter, dry as a bone, hot as a hare, Full as a flask (urinary RETENTION !!!) |
|
|
TCAD toxidrome by symptom |
-Heart beats fast(qrs prolongation) tachycardia, -hypotension (adrenergic blockade) -hyperthermia from heart beating fast Mental status : mad as a HATTER(confuison lethargy dizziness and coma (anticholinergic). PE -mydraisis (dilated pupils blind as a bat) -dry as a bone (dry membranes Distended bladder (no bowel sounds) -red as a beet LAB : You will see a prolonged QRS with cardiac dysarrythmia |
|
|
Cardiotoxicity : how does it happen with TCA |
TCA: Inhibits fast sodium channel leading to slowing of phase 0 depolarizing -which results in QRS/QTc -arrhythmias (VT,VF,TdP) |
|
|
Explain further toxicities |
-cardiotoxicity (sinus tachycardia) is hard to differentiate from anticholinergic symptoms
-hypotension from impaired myocardial contractility and decreased PVR (alpha adrenergic blockade) & pulmonary edema - since edema occurs you want to treat fluid overload |
|
|
TCA levels that are toxic in the blood? What amount is toxic to ingest ? QRS complex is how many miliseconds |
TCA toxic levels are over 1000 -Over 1 G is toxic to ingest QRS is usually over 100 ms and indicator of toxicity |
|
|
WHAT IS MAIN TREATMENT??
Aggressive treatment ABC gastric lavage and charcoal NO IPECAC NO HD |
Main treatment is SODIUM BICARB |
|
|
Symptomatic treatment for TCAD Arrythmia? Hypotension? seizures? Phystostigmine? DO NOT USE leads to bradycardia and asystole (flat line) last line |
Arrhythmias: lidocaine is DOC for ventricular arrhythmias Hypotension: fluids first THEN dopamine and pressors Seizures: benzodiazepines |
|
|
Children are usually victims to iron overdose because of |
multivitamins |
|
|
Mechanisms of toxicity , what happens? |
GI irritant. Results in hemorrhage and bowel perforation. -excess iron absorption -Fluid and electrolyte imbalances --- Acts as mitochondrial poison and hepatotoxicity - metabolic acidosis occurs with iron due to mitochondrial upset CV effects SHOCK --- |
|
|
Levels of toxicity of IRON : How do you know dose is enough to send you over: over 500 mcg/dl : are serum levels useful? |
Progresses from -stage 1 NVD, blood in stool,acidosis/shock -Stage 2 - then seem fine but don't know if patient will present to stage 3 NVD-->ab pain-->blood in stool -->coma-->liver dysfunction more than 60 mg = severe lethal toxicity YES ! you can get in less than half an hour over 500 is a lethal serum level ! good unlike aspirin |
|
|
Radio opicites indication for what toxicity |
will show you you have iron toxicities |
|
|
Treatment for Iron toxicity |
Deforxamine( chelation therapy) is the preferred treatment IV so psuedo allergy can occur |
|
|
for iron & blood transfusions |
Patient gets iron toxicity ffrom transfusions, butyou give EPOGEN not defuroxime. Sickle cell disease and aplastic anmiea - gets blood transfusions. not defuroxime |
|
|
Cynide toxicity : occurs with what drug |
cyanide toxicity occurs with : sodium nitro prusside |
|
|
Cyanide toxicity causes: |
cyanide blocks mitochondrial cytochrome oxidase. prevents electron transport and oxygen utilization and oxidative metabolism |
|
|
Person can get Cyanide toxicity because of |
Hepatic impairment and renal impairment because thats where cyanide elimination and metabolism occurs |
|
|
In renal impairment patient develops what ? what chemical does it? Also what else can thiocynate affect whats a side effect? |
Patient accumulates Thiocyanate -this causes neurotoxic syndrome and can supress thyroid function Why does this happen if they are on nitro prusside for so long? because they don't get a nitrate free interval bitter almond breath. cyanide Side effects occur in the mouth. burning mouth , throat, agitation , syncope, N/V , HA, diaphoresis,dyspnea tachycardia,htn |
|
|
Treatment of cyanide toxicity |
Amyl nitrite, sodium nitrite, sodium thiosulfate and oxygen step 1. Any Nitrite converts hemeglobin to MET hemglobin (hgb goes to met ball hehe) which is a better carrier of cyanide Step 2. Thiosulfate reacts with cyanide and picks it up from met hemaglobin becomes thiocynate Step 3. Oxygen to reverse binding of cyanide to cytochorme oxidase by convert methemeaglobin to hemeglobin.
|
|
|
Hydroxycobalamine and its role in cyanide toxicity ? |
hydroxycobalamine when given creates a non toxic cyanocoblamine. It frees up oxygen from cytochrome oxidase in mitochondria so oxygen can work |
|
|
CCB and beta blocker - antidote ?How does it work? |
Glucagon works by promoting intracellular reentry of calcium from calcium channel blockers. Thus, glucagon has chronotropic and iontropic effects by increasing camp. It improves sypmtoms with ccb and BB blocker overdose. glucagon+calcium gluconate |
|
|
Beta blocker overdose |
B1: increase in HR and contractility too much beta blockers cause DECREASED levels of cAMP. -you have decreased myocardial contractility. -decreased automaticity of pacemakers cells . ALSO CALLED DYSRYTHMIAS B3 : controls temp so over dose can cause hypothermia. b2: non-selctive blockade : impaired gluconeogenesis, decreased insulin release |
|
|
Beta blockers that cause toxicity: name the agents : |
Lipophilic drugs cross bbb faster so cause toxicity. (seizure risk) These agents inhibit sodium fast channels and widen the QRS which may potentiate other arythmias. acebutolol: sectral propanolol :inderal betaxolol: nebivilal? atenolol: tenormin solotol an disa agents also prolong qt |
|
|
cholinergic effects: |
SLUG : THINGS LEAKING drool,lacrimation, urinary incon, hyperactive bowel sounds(GI ) |
|
|
Beta Blocker Over dose will antagonize effects at heart leading to : |
DECREASE DECREASE in whats important/ HR and BP Brady cardia, Hypotension, mental status change, delirium, seizure, coma. sometimes broncospasam and hypocalcemia. antagonisim at beta 1 --> need to increase camp--> increase calcium |
|
|
how to treat BB overdose: |
ABC, Fluids MAGNESIUM tdP,Glucagon Calcium gluconate to increase ionotropy because thats what you have to do Insulin incase too much glucagon stil give fluids before you give presssors |
|
|
A lipid emulsion therapy can also be given. explain and what else is this used for? |
Give for bb OD or TCA. Lipids act like a sink. They surround molecules that are lipophillic and pulls them out like a DRAIN. acts also as energy to improve myocardial function lipid sinkm for TCA,bupivicaine, chlopromazine and beta blockers Insulin improves myocyte metabolisim convert % to ml ie:10%= 10g/100ml ie 20%= 20g/200ml ie:30g= 30g/300ml |
|
|
treatment again for BB |
First line: glucagon It actually activates cAMP in increases calcium entry, - calcium salts -gluconate and chlorid, increases iontropy |
|
|
Insulin and glucose is indicated as treatment options but when do you use it? |
Ideally for those hemodynamicly unstable |
|
|
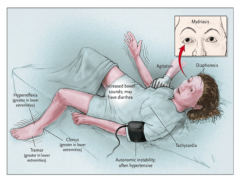
Clinical triad of serotonin Syndrome |
1. Mental status change 2. autonomic hyperactivity 3. neuromuscular abnormalities Intensity of symptoms : some have mild some have sevre. severe is -delirium -neuromuscular rigidity -hyperthermia |
|
|
Symptoms progress -----> |
Akathisia(mild)-->tremors--->mental change -->clonus-->hyperthermia-->muscle hypertonicity /death ATM(ental change) CHM(uscle hypertonicity) clonus is when muscles are always twitching, you risk seizures and muscle cells break down . myoglobin gets lodged in kidney and you risk Rhabdomyolysis when it blocks kidneys. |
|
|
look out for serotonergic properties with analgesics ie: |
Tramadol (ULTRAM ) + Celexa(citalopram) + venlafaxine (effexor) not a good combo |
|
|
Mild cases of serotonin syndrome look like what? |
ANti-cholinergics toxicity! Except for being hot. These patients are -Afebrile meaning they have no FEVER! hot a hare on anticholinrgics -Tachycardia -shivering (becuase shivering heart rate is up because your moving) -diphoresis( SWEAT)' (not in anti cholinergics, in Anti chol you are dry as a bone, no sweat.) Mydriasis- dialted pupils (catecholamine release) - tremors /clonus *new* |
|
|
Moderate signs of SSyndrome |
-mydraisis (catecholamine relase causes this) -Hyperactive bowel sounds (TCA absent) -diaphoresis (clamy(TCA and antich dry and hot) - lower extremity (hyperflexia) EYES horizontal ocular clonus / nystagmus Hypervilgilant (bird like reflexes ) peculiar head turnings |
|
|
severe case of serotonin syndrome |
SEVERE HYPERTENSION hyperthermia severe muscle rigidity rhabdomylysis renal failure DIC (coagulation goes haywire) disorder with coagulation |
|
|
Serotonin is produced from |
Decarboxylation and hydroxylation of L-tryptophan if you have dysregulation of mech cotrollowing it and over production you can have serotonin syndrome. TrIPtans TRIP you into serontonin syndrome |
|
|
How does it affect alll these symptoms ? |
Usually serotonin affects wakefullness, affective behavior, food intake , theromoregulaton, migranes. emeisis , sexul behavior, motor tone, GI MOTILITY, pain ieL anti emetics are antagonist not really agonist encouraging production of extta serrotonin, but what it does is that it antagonizes the receptor and stimulates production of serrotonin at other receptors |
|
|
drugs that cause serotonin syndrome. |
Anti depressants Trazdone-desyrel nefazodone-serzone busprione - BUSPAR venlafaxine-effexor -clomipramine- anafril/clofranil MAO-I phenelzine- nardil isocarboxazid- marplan Moclobemide- auroix clorgiline- clorgylene Seleigiline (parkinsons)eldepry; resegiline-azilect Valproic acid: valproate analgesics Meperidine-Demerol fentenyl- duragesic tramadol- ultram pentazocine- naloxone? ondesteraon - zofran metoclopramide - REGLAN (regulate gerd) sumatriptan (imitrex |
|
|
sibutramine is ? other herbals that cause _____ |
sibutramine also called meridia. A drug herbal associated with serotoin syndrome. Its was originally an anorexic drug that supresses appetite. now a diet pill called asian bee pollen. be careful with serotonin drugs and: dextromethorphan MDMA LSD st johns wort ginseng Tryptophan linezolid - zyvox ritonivr |
|
|
These drugs INHIBIT metabolisim of serotonin |
tranylcypromine (parnate) phenelzine(narDIL) Selegeline (eldepryl) like ELDER-pryl since its for parkinsons linezolid(zyVox) |
|
|
These drugs INCREASE serotonin release |
Increase serrotonin release: Amphetamines -stimulant Mirtazipine Anorectics ---buspirone & lithium stimulate post synaptic receptors These have ssri like mechanisims be aware: Tramadol ,TCA,venlafaxine |
|
|
Neruromalignant hyperthermia symtoms ? What causes it? |
caused by anesthetics deflourane, decamethonium . side effects like rapid breathing which is asscoiated with VERY HIGH heart rate and VERY HIGH TEMPERATURE (clammy and sweaty with ssri) RIGID muscles / rhabdo risk |
|
|
Neurleptic malignant syndrome ? |
muscle rigidity, fever, autonomic instability,[1]and cognitive changes such as delirium, and is associated with elevated plasma creatine phosphokinase.[2] Theincidence
with neurolepti and antipsych drugs |
|
|
How do we treat serotonin syndrome? |
Look for symptoms -tremor/ hyperflexia -spontanous clonus or inducible -muscle rigidity -temperature 38 degrees(not high) -agitation/ diaphoresis
YOu REMOVE OFFENDING DRUG administer 5hT2 antagonist L Antidote : CYproheptadine (Periactin) binds to serotonin receptors olanzapine and chlorpromazine also has eveidance DO NOT GIVE proplanolol, datrolene or bromocriptine for serotonin syndrome. Be careful not to misdx as malignant hyperthermia or NM syndrome |
|
|
Tell patient dont over dose with migraine and tramadol therpies |
these are common drugs that cause serotonon syndrome ! |
|
|
Lead is a big problem alot of conditions are ___ LEad level of concern : why children? most common cause? paint chips |
symptomatic and go untreated largely - when lead levels reach 10 and over IQ damange occurs its when you should be concerned . levels more than 10 zdecreases syn of vit - their stomachs absorb lead like water to wells and dry trenches ! 40% |
|
|
calabash balls have high levels of |
lead in it harms 1st trimester baby . Alarcon,alkohl,azarcpm, bali goli |
|
|
How does lead get absorbed into the GI tract?? |
it get absorbed in GI tract and compete with calciumso diet plays a role |
|
|
SO lead stays in the body for a short/long time? Its redistributed to bone teeth and hair lead primariy effects : how? |
long time after its absorbed it dist to soft tissues, espeically kidneys and liver! it also hoes to teeth bone and hair. blue line in gums "lead line" ALL lead cirulates through the body in a vehicle and that vehicle are ERYTHROCYTES !!! anemias associated with lead poison -Blood/GI/Neuromuscular/RENAL lead blocks enzyme : ferocheltase and protoprophyrin |
|
|
Enzymes it affects? GI effects how does lead affects that |
Lead effects smooth muscle of GI tract which produces a vague abdoinal syndrome . STomach pain is aan early sign of disease. the more lead the more consipation and "lead colic" |
|
|
whats pathenmenoic for lead toxicity? what else is seen? what about detrimental effect ? |
Lead palsy which is seen in acute toxicty. Marked by wrist and foot drop. also hyperkinetic aggresive behavior is seen/ ADHD is missdx lot -Lead encephalopathy. had been seen with levels as low as 50 and over 100. Early signs of lead encephalopthy : clumsiness, vertigo,headace, insomina... LATE SIGNS OF lead induced encephalopathy EXcited / confused behavior/ delerium / tonic and cloni convulsions worst outcome: COMA |
|
|
Lead poison can be found out with Blood lead level test. also you can do erythrocyte protophyrophin levels abdominal x ray |
since this enzyme is inhibited |
|
|
what do you treat lead poison with ? MUST USE BOTH !!! Who is contraindicated ? |
Dimercaperol (BAL) Contraindicated with ppl who have a peanut allergy G6PD- deficient - USE: CaNaEDTA to chelate calcium. NEPHROTOXIC so monitor renal bun/creatnine DO not use Na2EDTA |
|
|
Un approved Treatment Heavy Lead ? Allergies : |
Penicillamine - for heavy metals copper and lead Allergies: PCN be aware |
|
|
ONLY FDA approved kid (mostly) antidote for lead CAVEAT With children taking this |
Succimer or CHET-met CHEMET They must be in a lead free environment . if not they have to be in hospsital with it. Transient increase in LFT. If not will lead rebound despite treatment recheck lead 7-21 day after treatment |
|
|
MAINSTAY TREATMENT OF LEAD IS |
to decrease blood lead levels |
|
|
OXY eliete also called ______ causes |
Oxy elitie is a dietary supplement with the active dangerous compound called AGELIN. Its calle dbael apple if in nature. concentrated AGELIN messes with liver acute hepatitis is being inverstigated |
|
|
amioderone has a long half life thats what |
mimics cirrhosis even though its called acute nothing short about it |
|
|
chlolestatic rxns are: sign of cholestatic: WHat happens? |
Blockage to bile flow due to drugs -early jaundice associate with puritis/itchiness Gal stones block bile and you get bilary sludge. |
|
|
What drugs causes cholestatic disease ? labs for cholestatic disease |
Biliary sludge is caused by estrogens,cotrimoxazole,rifampin nafcillin,chlorpromazine, erythromycin colic stool seen GREY elevated transaminiase 2-8xs upper limit Elevated alk phos 3x's limit normal:30-120 hyper bilirubnia (25) Normal:0-1 |
|
|
Veno occlusive disease What causes it what labs what treats prophylaxis ?? |
Cuased by taking a drug called Busulfan. veno occulsive WIPES out immune system. Its similar to cholestatic but MUCH MORE SEVERE and SERIOUS YOu get a giant liver + Weigh gain ie: ascites (5% above) bilirubin is high over 1 / alk phos is high over 120, AST over 35 Encephalopthy occurs from excess ammonia ! pt cant metabolize ammnnia clots form . TREAT WITH DRUG URSoDIOL or Actigall it dissolves billiary salts decrease extra vascular problems increase intravascular problems give tpa for clots prophylaxis: defobrotide |
|
|
allergic hepatitis : |
allergic rxn at the heaptic level. fever/rash/lymphadenopathy/eosinophilia results in hepatic necrosis and cholestasis looks like on the outside like mono Drug that causes this is famous phenytoin and co-trimoxazole These drugs act like haptens and ellicit an immune response at the level of liver |
|
|
idiosyncratic hepatoxic rxns |
NON-dose related DOES NOT INvOLVE THE IMMUNE SYSTEM may be genetic link with slow acetylators INH causes it alot. increaases transaminase when ast and alt is over 500 you gotta stop drug -mixed forms of hepatic dysfunction allopurinol,aspirin, sulfonamides, quinidine, HMG-co-reductase inhibitors,valproic acid , INH, and troglitazone trovafloxacin and quinilone |
|
|
indolent cirrhosis |
caused by high doses of methtrexate. Cirrhosis sneaks up on you over TIME! with like warning or signs. LIVER biopsy is the key for earlu dx. Usually do it after you have take over 2500 mg of methotrexate to check for indolent cirrhosis |
|
|
kava kava and vitamin A are bad because they cause liver toxicity. |
Mega doses of vitamin A (toxic level over 20,000) are bad bad so is kava kava(sleep remedy) which is a mood altering agent |
|
|
market withdrawl from being toxic to liver |
Accutane - isotrentenoin Beycol-cerivastatin bextra-Valdecoxib (NSAID) Cylert- pemoline Pemoline -cyclert-adhd ALL removed due to livr toxicity |