Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
8 Cards in this Set
- Front
- Back

Hx:8yo B parents are concerned about the appearance of the child's middle finger. The child denies pain and his digital neurovascular status is nl. A clinical photograph & Xrays are provided in fig. For children with this condition, which of the following is the best intervention to achieve a finger that is proportional to the rest of the hand? 1-Epiphysiodesis now; 2-Epiphysiodesis when the finger reaches adult length of the father
3-Compression wrapping until proportional size is achieved; 4-Resection of hypertrophic nerves 5-Osteotomy at skeletal maturity. |

Clinical photograph and radiographs demonstrate macrodactyly of the middle finger, a rare congenital malformation enlarging all structures of the digit.
Ishida et al reviews 23 cases of surgically treated macrodactyly finding favorable results with epiphysiodesis/epiphysiodectomy while resection of hypertrophic nerves was unsuccessful in preventing overgrowth. The epiphysiodesis is performed once the finger reaches the length of the same sex parent, using their digit as a template for final growth.Ans2 |
|

pt sustains the injury in Fig from a gunshot injury. The PE is notable for lack of sensation in his fourth and fifth digits as well as a positive Froment's sign. Which of the following factors has not been shown to be a significant prognostic indicator of functional recovery following nerve repair? 1-Duration to time of repair; 2-Repair level;
3-Length of repair; 4-Postop physical rehab; 5-Type of autograft used |
The clinical scenario describes an ulnar nerve laceration. Studies have shown that the ulnar nerve does not typically have good outcomes after nerve repair. (worse recovery than repairs of the tibial, radial, femoral, and musculocutaneous nerves) Many factors including age of patient, time to repair, repair level, and length of repair have been shown to be important determinants in nerve recovery following repair. The type of nerve graft (sural, saphenous, etc) used has not shown to be statistically significant in terms of functional recovery after nerve repair.Incorrect Answers
Answer 1: Earlier nerve repairs typically have better functional results. Answer 2: The lower level of nerve repair (more distal), the better functional results. Answer 3: Shorter length of the nerve repair typically leads to better functional results. Answer 4: Pre and post operative physical rehabilitation after nerve repairs has been shown to have better results.Ans5 |
|

You are seeing a 24yo male in the ER p/ he was involved in a knife fight. He has severed the common digital nerve to the index finger on his dominant hand, with an 8mm gap between nerve ends. In counselling him about repair, which of the following options is as good as autologous nerve grafting? 1-Glycolide trimethylene carbonate conduit; 2-Collagen conduit; 3-Silicone sleeve; 4- Primary end-to-end repair; 5-Polyglycolic acid conduit
|
Repair of segmental nerve loss in the hand using collagen conduits allows for nutrient exchange and accessibility of neurotrophic factors to the axonal growth zone during regeneration. While the other listed answers have been used, none has shown the efficacy of collagen conduits or autograft. Li et al. describe the repair of peripheral nerves with a tubular collagen conduit and review supporting data from in vitro and in vivo primate studies to this regard. Bertleff et al. describe the recovery of sensory nerve function after treatment of traumatic peripheral nerve lesions with a biodegradable poly(DL-lactide-epsilon-caprolactone) neurolac nerve guide, compared to their control of end-to-end repair, no autologous grafting. They show equal results between primary end-to-end repair and their synthetic graft. Waitayawinyu et al. compared 2 synthetic polyglycolic acid conduits to autogenous nerve grafting using histopathologic and neurophysiologic analyses in a segmental defect rat model. They found that collagen conduits and autografts produced comparable results, which were significantly better than polyglycolic acid conduits.Ans2
|
|

Which of the following nerves has the most favorable regenerative potential in restoring motor function after a graft repair within half a year after being injured? 1-Median; 2-Ulnar; 3-Radial; 4-Tibial; 5-Peroneal
|
Of the choices listed, the radial nerve has the best opportunity for recovery.
Roganovic performed a prospective study of 393 graft repairs of the median, ulnar, radial, tibial, peroneal, femoral, and musculocutaneous nerves showed that peripheral nerves differ significantly regarding the motor recovery potential, and the expression of differences depends on the level of nerve repair. The following nerves had excellent recovery potential: the radial, musculocutaneous, and femoral nerves. The following nerves had moderate recovery potential: the median, ulnar, and tibial nerves. The following nerve had poor recovery potential: the peroneal nerve.Ans3 |
|
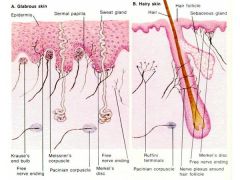
Which of the following structures are slowly adapting skin receptors that detect pressure, texture, and low frequency vibration and are best evaluated by static two-point discrimination? 1- Meissner's corpuscles; 2-Pacinian corpuscles; 3-Merkel's receptor; 4-Free nerve endings; 5-Ruffini corpuscles
|

Merkel's skin receptors are slowly adapting skin receptors that detect pressure, texture, and low frequency vibration and can be appropriately evaluated by static two-point discrimination. Merkel's disk receptors adapt slowly and sense sustained pressure, texture, and low-frequency vibrations.Ans3
|
|

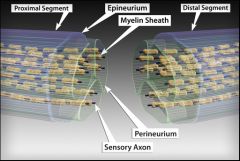
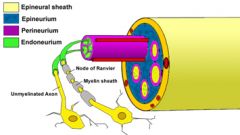
Which of the following peripheral nerve structures functions to cushion the nerve against external pressure? 1. Endoneurium; 2. Fibronectin; 3. N-cadherin; 4. Epineurium; 5. Perineurium
|
The epineurium is a supportive sheath surrounding peripheral nerves that cushions fascicles against external pressure. It is comprised of a loose meshwork of collagen and elastin fibers that are aligned parallel with the nerve fibers.
Illustration A & B depicts the contents of a nerve including epineurium, perineurium, and endoneurium. Incorrect Answers: Answer 1: Endoneurium is a fibrous tissue that covers the axon, Schwann cell, and myelin of each nerve fiber. Answer 2: Fibronectin and laminin are extracellular matrix glycoproteins that facilitate directional nerve fiber branching. Answer 3: N-cadherin is an adhesive membrane glycoproteins on neural ectoderm and facilitate growing axons. Answer 4: Perineurium is a dense connective tissue which surrounds nerve fascicles. It provides high tensile strength. The perineurium also limits diffusion within the intraneural environment and subsequently prevents injury from edema.Ans4 |
|

Hx:35yo professional football player c/o severe wrist pain after making a tackle. He reports paresthesias in his thumb and index finger. AP and lateral xrays of the wrist are shown in fig A & B respectively. What is the next step in management? 1. SAC thumb spica, 2. LAC thumb spica, 3. urgent CR and splinting; 4-MR arthrogram of the wrist to assess lig injuries; 5-bone scan to assess vascularity
|

This patient is presenting with a perilunate dislocation with carpal tunnel symptoms. The most important next step in treatment is reduction of the dislocation. Kozin et al note that these injuries can be overlooked and have variable propagation patterns through the carpus/carpal ligaments. This patient has a radial styloid fracture due to avulsion of the radiocarpal ligaments. Melone et al note that these injuries were historically treated with closed reduction and pinning, but more recently the trend is for open reduction and fixation, for optimal anatomic restoration.Ans3
|
|
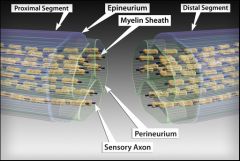
Axon regeneration almost always occurs following a Seddon second-degree nerve injury, also known as axonotmesis, because what anatomic structure is not injured.
1. Epineurium 2. Endoneurium 3. Perineurium 4. Myelin sheath 5. Schwann cell |
By the Seddon classification there are three grades of injury. 1st degree injury or neuropraxia is a nerve bruise with axonal continuity leading to a reversible conduction deficit that resolves with time without Wallerian degeneration. 2nd degree injury or axonotmesis is when there is a disruption to the axon and myelin sheath with an intact endoneurium - recovery is possible due to the integrity of this intact endoneurial connective tissue layer surrounding the nerve. 3rd degree injury or neurotmesis is the most severe form of injury in the Sedon classification and represents complete nerve injury with disruption of axon, myelin sheath and endoneurium - in these injuries surgical repair is indicated because there will not be spontaneous recovery.
Sunderland further breaks down axonotmesis into third-degree (class II) where the there is a lesion of the endoneurium, but the epineurium and perineurium are intact, fourth-degree class II) where only the epineurium remains intact, and fifth degree (class III) where there is a complete transection of the nerve. Ans2 |