Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
5 Cards in this Set
- Front
- Back

Figure A depicts a child with syndactyly. Following surgical treatment, the MC complication involves which of the following? 1-Nail plate; 2-Nail bed;
3-Web commissure; 4-Radial digital nerve 5-Radial digital artery |

Web creep, the most common complication of this procedure, is the distal migration of the web commissure seen in surgically corrected syndactyly patients. It is caused by abnormal scar tissue formation and increasing growth of underlying osseous structures. Informing parents of this complication preoperatively is advised, treated with either STSG or FTSG at 21 years, FTSG had higher rates of web creep, hyperpigmentation and hair presence. The authors did not favor one technique over the other.Ans3
|
|
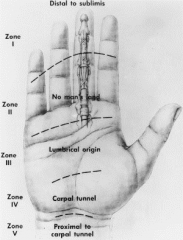
Hx:24yo M cuts his L middle finger with a knife while chopping vegetables. PE =a zone 2 flexor tendon laceration. He undergoes a 2-strand core suture repair with epitendinous suture. This particular repair is strong enough for each of the following rehabilitation protocols EXCEPT: 1-Kleinert protocol; 2-Duran protocol; 3-Synergistic motion protocol; 4-Low force and low tendon excursion passive range of motion; 5-Early digit active ROM protocol
|

Early active range of motion protocols are thought to decrease adhesions but risk rerupture or gap formation. the generation of muscle forces to either assist digit flexion or perform “place and hold” exercises require at least a 4-strand core suture with epitendinous repair. This patient only had a 2-strand repair.Ans5
|
|

Flexor tendons of the fingers within Zone 2 receive their primary nutritional supply from: 1-Vinculae
2-Phalangeal periosteum; 3-Musculotendon junction; 4-Tendon insertion; 5-Diffusion from the synovial sheath |
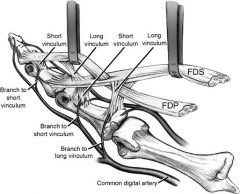
The vascularity of tendon varies depending on the type of tendon (e.g. with or without a sheath) and the location. Sheathed tendons (e.g. flexor tendons of the hand) have a dual blood supply via both vascular perfusion but also have regions that are relatively avascular where they receive nutrition through synovial diffusion. This is the case in zone 2 of the digital flexor tendons where the primary nutritional supply is from synovial diffusion through the parietal paratenon which allows for passive nutrient delivery to the flexor tendon within the sheath. The digital flexor tendons also receive minor direct arterial perfusion in zone 2 through the vinicular system, osseous bony insertions, reflected vessels from the tendon sheath and longitudinal vessels from the palm, but this is not the major blood supply.Tendons not enclosed by a sheath receive their blood supply directly from vessels entering from the tendon surface or from the tendon-to-bone insertion.Ans5
|
|

Which of the following skeletal dysplasias is caused by a sex linked mutation of the short stature homeobox (SHOX) gene? 1-Cleidocranial dysplasia
2-Leri-Weil dyschondrosteosis; 3-Pseudoachondroplasia; 4-Ellis-van Creveld (EVC) syndrome; 5-Achondroplasia |

Leri Weill dyschondrosteosis is a skeletal dysplasia characterized by short stature and bilateral Madelung deformities of the wrist. The SHOX gene is located on the X and Y chromosomes and a mutation on either of the sex chromosomes leads to the dysplasia (sex linked dominant). Madelung deformity is a result of disruption of the volar ulnar physis of the distal radius (leading to radial inclination and a radiopalmar tilt). Symptoms from the wrist deformity include ulnocarpal impaction, restricted forearm rotation, and median nerve compression.
-Cleidocranial dyplasia is an AD defect in CBFA-1, a transcription factor that activates osteoblast differentiation. -Pseudoachondroplasia is an AD mutation in COMP on chromosome 19. -Ellis-van Creveld (EVC) syndrome is an AR mutation in the EVC gene causing acromesomelic shortening and postaxial polydactyly among other anomalies. --Achondroplasia is an AD mutation of FGFR-3.Ans2 |
|

Hx:54yo M presents with a slowly enlarging mass on the dorsum of his L wrist which has been present x 3 yrs. He denies any significant symptoms. PE shows a 1 cm palpable mass. A MRI is shown in Figure A. A biopsy of this lesion would most likely show? 1-Synovial cells with mucin accumulation; 2-Proliferating histiocytes of moderate cellularity and frequent multinucleated giant cells; 3-Polymorphonuclear neutrophils; 4-Spindle cells arranged in intersecting bundles; 5- Lipocytes, spindle cells, and scattered atypical giant cells
|
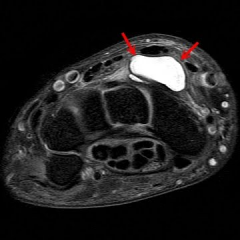
ganglion cyst. Histology of a ganglion cyst would show a mucin filled synovial cyst. MC mass found on the hand or wrist. Dorsal ganglions originating from the scapholunate (SL) ligament are the MC (60%). They are caused by trauma, mucoid degeneration, or synovial herniation. On exam, they appear fixed to the underlying deep tissue, but not to the skin and are commonly translucent to light illumination. T2-weighted MRI axial image of the wrist will show increased signal where the cyst is located. dorsal ganglions are the MC (60% to 70%) and are found between the third and fourth dorsal compartments arising most commonly from the scapholunate ligament. Supportive splints and anti-inflammatories in conjunction with aspirationare are an important part of nonop Tx. Aspiration of dorsal ganglions (not recommended for volar ganglions) yields a recurrence rate of around 50%.
Answer 2: Proliferating histiocytes of moderate cellularity and frequent multinucleated giant cells.Ans1 |