Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
7 Cards in this Set
- Front
- Back

Hx;14yo B c/o leg-length discrepancy with the R leg shorter than the L. He has nl height for his age and his skeletal age is equal to his chronologic age. hx & PE of Tanner staging reveals that he began puberty 1 mth ago. His estimated final LLD at skeletal maturity is calculated to be 30mm. Which of the following surgical options is the most appropriate to equalize the limb length discrepancy? 1-Physeal stapling of the medial tibial and femoral physis now with staged removal of staples at age 16; 2-Lengthening of the right femur with ring external fixator now; 3-Epiphysiodesis of the left femur only in 1 year; 4-Epiphysiodesis of the left femur and left tibia now; 5-epiphysiodesis of the bilateral femurs and shortening of the left tibia now
|
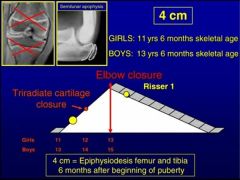
The calculated discrepancy at maturity is given as 3cm of shortening. Epiphysiodesis is the typical answer for growth differences between 2 and 5 cm.Ans4
|
|
Hx:14-yo B sustains a significant distal fem physeal fx. Assuming that he has a complete growth arrest, what is the predicted LLD? 1. 1cm; 2. 2cm; 3. 3cm; 4. 4cm; 5. 5cm
|
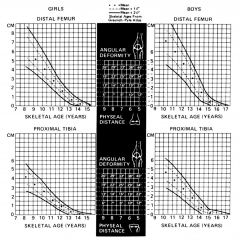
assumes that girls and boys stop growing at 14 yo and 16 yo, respectively. Additionally, this method assumes a certain contribution of each physis to longitudinal annual growth:
Proximal femur – 4mm per year Distal femur – 10mm per year Proximal tibia - 6mm per year Distal tibia – 5mm per year. total=25 In this question, the boy has two years of growth remaining with a predicted arrest thru his distal femoral physis. Therefore, he will lose 20 mm or 2 cm of growth.Ans2 |
|

Hx;9yo M sustains the fx seen in Fig A. If a complete growth arrests occurs, his expected LLD at skeletal maturity would be? 1. 2 cm; 2. 3 cm; 3. 4 cm; 4. 5 cm; 5. 6 cm
|
Proximal femur – 3mm per year
Distal femur – 9mm per year Proximal tibia - 6mm per year Distal tibia – 5mm per year. Tot=23 In this question, the boy has 7 years of growth remaining with a predicted arrest thru his distal femoral physis. Therefore, he will lose 63 mm or 6 cm of growth.Ans5 |
|
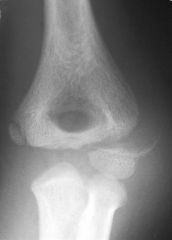
Hx: 36yo M c/o L hand weakness. A current clnical photograph of his hand is ulnar claw-hand deformity, medical history is(+) for the elbow injury Fig, which was treated non-op 28 yrs prior. Current xray evaluation of the patients elbow will most likely reveal what deformity? 1-Cubitus valgus
2-AVN of the lateral fx; 3-Fishtail deformity of the distal humerus; 4-Fx nonunion and a nl carrying ang; 5-Myositis ossificans |

Cubitus valgus deformity may occur due to a nonunion, malunion, or premature physeal closure. Acute neurologic injuries are rare with these injuries, however tardy ulnar nerve palsy (as demonstrated by the claw-hand deformity in Figure A) occurs late in the treatment and follow-up of lateral condyle fractures and usually is due to cubitus valgus. In addition to claw-hand deformity, other classical examination findings consistent with ulnar nerve palsy include Froment sign (compensatory thump IPJ flexion due to weak adductor pollicis) and Wartneberg sign (persistent abduction and extension of the small digit during active adduction due to weak interosseous and lumbrical musculature). Interosseous and/or first web space atrophy is another common finding.Ans1
|
|

Hx:7yo G undergoes ORIFof a displaced humeral lateral condyle fx. Dissection around which portion of the fx fragment should be avoided to protect its blood supply? 1-medial; 2-lateral; 3-superior; 4-anterior; 5- posterior
|
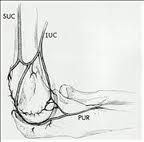
predominant blood supply to the lateral condyle of the distal humerus comes posteriorly. Nonunions occur because of these fractures are intra-articular and bathed in synovial fluid. When nonunions occur, the characteristic deformity is a cubitus valgus and subsequent ulnar nerve symptoms. Skak et al found that trochlear growth may become impaired after this fracture. DIsplaced lateral condyle fractures require (typically open) reduction and internal fixation to obtain anatomic articular alignment. Jakob et al noted that dissection during ORIF can lead to osteonecrosis of the condylar fragment, so care should be taken.Ans 5
|
|

Hx:5yo B has a hx of b/l dislocated radial heads, b/l knee dislocations, and flattened facies. What other important orthopaedic-related condition must be checked in this patient? 1-congenital vertical talus
2-congenital trigger thumb; 3-tibial hemimelia 4-cervical kyphosis; 5-congenital pseudoarthrosis of clavicle |

arsen’s syndrome is characterized by multiple dislocated joints, including hip, knee, elbow/radial head, foot deformities, scoliosis, and potentially lethal cervical kyphosis. It is important to obtain screening radiographs of the cervical spine in these patients to identify kyphosis and prevent neurologic complications. Progressive kyphosis may require cervical fusion. In addition to the orthopaedic manifestations, patients can also have laryngeal or tracheal problems, lesions of the heart valves, or aorta, and hyperelasticity syndromes that present as hypotonia.Ans4
|
|

Hx:5-yo B c/o a limp and pain over the medial aspect of the foot. xrays fig A and B. Orthotics have failed to improve his symptoms. What is the next appropriate management of this condition? 1-core decompression; 2-triple arthrodesis; 3-subtalar fusion; 4-IV abx w/ I & D; 5-short-leg walking cast
|

osteonecrosis of the navicular bone, otherwise known as Kohler’s disease. Treatment is traditionally symptomatic and pain usually can be relieved by limiting activities, and using orthotics. If this does not work, then a short leg walking cast for 4-6 weeks would suffice. Surgery is not indicated for this entity since it is self limiting.Ans5
|