Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
7 Cards in this Set
- Front
- Back

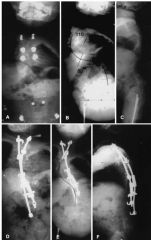
Hx:13yo M c/o L hip pain and an inability to ambulate. He does not have a hx of kidney dz. The initial xray Fig A. Which of the zones of the growth plate (Figures B-F, all the same magnification) is MC involved in this condition? ___________
|
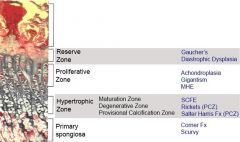
injures the hypertrophic zone of the growth plate, demonstrated in Figure D. It should be noted that SCFE secondary to renal osteodystrophy occurs at the secondary spongiosa, The zone of hypertrophy consists of chondrocytes that are 5-10x the size of normal chondrocytes, and is responsible for the synthesis of novel matrix proteins.
|
|

Hx:11yo obese M c/o SCFE. Which of the following figures accurately represents the method used to determine the xray severity of the epiphyseal slip and help guide tx? 1- Southwick method; 2- Klein's line; 3-Angle between the Hilgenreiner line and a line drawn from the triradiate epiphysis to the lateral edge of the acetabulum; 4-Shenton's line
5-center edge angle measurement. It is defined as the angle formed by a line drawn through the center of the femoral head and the edge of the acetabulum and another line perpendicular to a line drawn through the center of the femoral heads. |
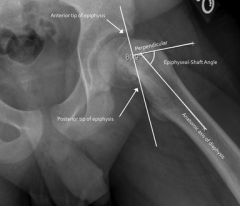
Determining the severity of SCFE using the Southwick method or slip angle is accomplished by subtracting the epiphyseal-shaft angle on the uninvolved side from that on the side with SCFE on the frog leg lateral pelvis radgiograph. The degree of slip is classified as mild (<30°), moderate (30° to 50°),or severe (>50°). Figure A shows an example of this calculation, where the slip angle is 44 degrees.Ans1
|
|

Hx:13yo Polynesian B c/o L groin pain and inability to place wt on the L leg xrays, Fig A & B. All of the following are true regarding this condition EXCEPT: 1-The L hip is MC involved; 2-Forceful manipulation is not indicated because it is assoc w/ an>risk of complications; 3-Associw/< fem anteversion and dec fem neck-shaft ang; 4-Pain is localized to the knee more often than the hip on initial presentation; 5-M are > F MC affected
|

hip pain 77-85% presented with hip or groin pain. 15%- 23% of patients had c/o knee pain or distal thigh pain, which can lead to unnecessary tests or misdiagnoses. Options 1,2,3, and 5 are all true statements .Ans4
|
|

Hx:14yo F c/o hx undiagnosed L SCFE x 3 yrs. now c/o 2 ys of activity-related L hip pain and pain w/ prolonged sitting, PE= restricted hip flex, an ER deformity, and obligatory ER upon hip flex manuevering. xrays Fig A . Which of the following osteotomies is MOST appropriate? 1-Medial displacement Chiari salvage osteotomy; 2-Prox fem varus osteotomy; 3-Flex, IR, and valgus-producing prox fem osteotomy (Imhauser osteotomy); 4-Bernese periacetabular osteotomy with extension, ER, and valgus-producing femoral osteotomy; 5-Valgus-producing intertrochanteric proximal femoral osteotomy (Pauwel osteotomy)
|

correction is obtained via an anterior-based closing wedge osteotomy, rotating the distal fragment internally, and utilizing the blade plate to create valgus. Valgus correction can be incorporated into the osteotomy to correct the medial displacement of the epiphysis. The osteotomy was designed to correct the retroversion deformity, improve hip motion and mechanics, and decrease the incidence of osteoarthritis. The retroversion deformity seen in late SCFE may cause anterior femoroacetabular impingement through a cam type mechanism, which may contribute to the early development of osteoarthritis.Ans3
|
|
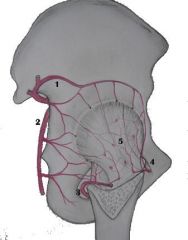
A R hip of an 8yo pt is modeled in Fig A. Which of the following vessels gives the greatest blood supply to the femoral head (name of vessel) ? 1. 1
2. 2; 3. 3; 4. 4; 5. 5 |

Answer 3 depicts the medial circumflex artery, which is the dominant blood supply of the femoral head in children older than 4 years of age, The lateral circumflex artery and ligamentum teres supplies a portion of the anterior femoral head until 2 to 4 years of age. When treating a patient with a SCFE its important to note that when multiple pins are placed in the posterosuperior quadrant, the lateral epiphyseal vessels may be damaged. This risk is minimized by placing a single screw in the center of the epiphysis, most important contribution to the vascular supply of the femoral head is from the posterosuperior lateral epiphyseal vessels that originate from the medial circumflex artery. These lateral epiphyseal vessels anastomose with the vessels from the round ligament and the posteroinferior epiphyseal vessels at the junction of the medial and central thirds of the femoral head.Ans3
|
|

Growth at the distal humerus physis accounts for what % of humeral length? 1-20%; 2-40%; 3-50%; 4- 60%; 5-80%
|
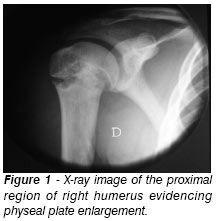
80% of growth in the humerus bone occured from the proximal humerus. Therefore, the distal humerus is responsible for the remaining 20% of growth.Ans1
|
|
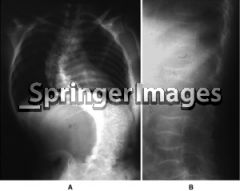
Hx:11yo G has been dx'd w/a severe form of osteogenesis imperfecta ->thin bones and multiple fx. f/u scoliosis which was noticed by her mother 1 year ago, no back pain and is neurologically intact. xray= 42-deg R thoracic curve, which has increased from 31-degree from her previous 9 mths earlier. What is the management for her spinal deformity? 1-Observation alone with serial xray and clinical monitoring; 2-PSF w/instrumenn; 3- ASF w/ instrumen; 4-Fixation w/telescoping rods
5-Custom-molded bracing with serial xrays and clinical monitoring. |
Children with severe forms of osteogenesis imperfecta and progressive scoliosis should be treated with posterior spinal fusion with instrumentation when the curve exceeds 35 degrees.Ans2
|