Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
8 Cards in this Set
- Front
- Back

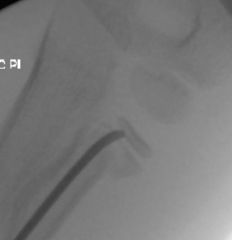
Hx:5yo G falls off of a trampoline & sustains a tibia fx. The tibia fx is reduced & placed into a LLC in the ER. A post-reduction xray is provided in Fig A. The parents should be counseled that a temporary tibial deformity may occur. Which best describes the deformity? 1-Recurvatum; 2-Varus; 3-Malrotation; 4-Valgus; 5-Procurvatum
|

Pediatric proximal tibia metaphyseal fractures, or Cozen fractures, heal reliably but often progress to a valgus deformity. The valgus deformity seen with Cozen fractures is secondary to an increase in metaphyseal growth medially.However, the affected tibia was longer than the contralateral tibia in 100% of cases with an average limb-length discrepancy of 9 mm.Ans4
|
|

Hx:13yo F c/o 1yr long hx of ant & lat foot & ankle pain. PE=limited subtalar motion compared to her contralateral foot. A lat xray FigA.CT in Fig B. What foot deformity is commonly associated w/ this condition? 1-Hindfoot varus; 2-Rigid pes planus
3-Pes Cavus; 4-Equino-cavovarus; 5-Rocker bottom foot |

Tarsal coalition, most commonly occurring as a talocalcaneal or calcaneovnavicular coalition, is the leading cause of peroneal spastic flatfoot and leads to a rigid pes planus deformity of the foot, "C-sign", which is shown in Illustration A. This is a radiodense outline between the talus and calcaneus best seen on the lateral foot radiograph that forms the shape of a "C". This is indicative of a talocalcaneal coalition.Ans2
|
|

Hx:14 yoG has chronic foot pain which has failed to respond to previous surgical coalition resection and soft tissue interposition. A xray foot in Fig A. A CT = talocalcaneal coalition w/ almost complete involvement of the subtalar joint. What is the tx of choice? 1-revision coalition resection and extensor digitorum brevis interposition
2. revision coalition resection and fat interposition 3. tibiotalocalcaneal arthrodesis 4. talonavicular arthrodesis 5. triple arthrodesis |

sx coalition before DJD changes have occurred, resection is the usual tx; however, this is not indicated if the pt has failed previous coalition resection surgery, and has >50% involvement of the subtalar joint. 3ple arthrodesis involves fusion of the subtalar, calcaneocuboid, and talonavicular joints and is the most effective procedure for fixed hindfoot and forefoot deformities. Subtalar fusion if NO significant hindfoot deformity, CI <(10-12 yrs) because of the limitation it puts on foot growth. Wilde et al found fair or poor results in all ten feet with preop CT scans showing an area of relative coalition to be >50% and heel valgus > 16 degrees.Ans5
|
|

Hx;10yo M c/o 6 mths of b/l foot pain @ the tarsal sinus. Clinical images of standing exam & heel rise in Fig A & B xray L foot Fig C & D. Which of the following findings is assoc w/ this patient's condition? 1-Dynamic supination during swing phase of gait; 2-Limited push-off power, limited forefoot contact, and excessive heel contact during stance phase of gait; 3-recurrent ankle sprains
4-PTT insufficiency; 5-Weak tibialis anterior relative to the peroneus longus resulting in first ray plantar flex |

Recurrent ankle sprains may be assoc w/tarsal coalition between the talus, the calcaneus, and/or the navicular. Calcaneonavicular coalitions are MC in children = 8 to 12 yrs, talocalcaneal coalitions are MC in the 12 to 15 yr age group. 10% to 20% of pts w/ tarsal coalitions have 2 coalitions and 50% are b/l.Ans3
|
|

Hx:10yo B c/o injury to his dominant elbow & presents to the ED w/ the injury Fig A & B. Following CR and casting, the fx remains angul 20 deg & translated 2mm. What is the next step in managt? 1-Immob in full pronation; 2- Immob in full supination; 3-Immob in neutral rotation; 4- CRPP; 5-ORIF
|

Indications for surgical management following closed reduction are angulation >30 degrees and fx translation >3mm, If adequate, the forearm is casted in neutral to slight pronation for 10-14 days as this is the most functional position.Ans3
|
|

12yo B falls 8 ft from a tree limb and lands on his outstretched hand, c/o elbow pain & displaced radial neck fx is noted on xray CR is attempted w/ sedation. A post-red xray is Fig A. Which of the following actions should be taken? 1-mmobilization in a sling until pain subsides; 2-Immobilization in a LAC x 6 wks to allow for callus formation and subsequent bony remodeling; 3- CT to further eval fxe and physis; 4-Hinged EXFIX of the elbow
5-ORIF |
radial neck fracture with greater than 45 degrees of residual angulation following closed reduction. The majority of pediatric radial neck fractures can be treated with closed reduction. Up to 30 degrees of angulation is considered acceptable. Greater than 30 degrees of angulation, a child approaching skeletal maturity, and loss of pronation/supination range of motion are indications for open reduction to prevent residual deformity.Ans5
|
|

Hx:6yo B has R elbow pain p/ falling onto an outstretched hand 8 hrs ago.xrays are shown in Fig A. Overnight, he develops increasing pain and swelling in his R forearm. What associated condition can develop w/ the fx sustained in fig A? 1-EPL rupture; 2-PIN neuropraxia; 3-Forearm compartment synd; 4-Common extensor origin avulsion; 5-MCL rupture
|

non-displaced pediatric radial neck fractures as evidenced by a mildly abnormal angular configuration of the lateral aspect of the proximal radial metaphysis. Peters et al reports on 3 patients who developed volar compartment syndrome with a radial neck fracture. Important clinical information is that they all fell from standing height on an outstretched hand, and the compartment syndrome developed 12-24 hours after the injury. All had severe pain that was exacerbated by passive flexion and extension of the fingers. All were treated with fasciotomies with good clinical results.Ans3
|
|

Hx;4yo B w/ Klippel-Feil synd has elevation of the L scapula since birth. Spine xray shows no evidence of scoliosis. What shoulder motion is likely to be most limited? 1-add; 2-abd; 3-IR; 4-ER; 5-extension
|

most common congenital shoulder abnormality. Associated conditions with Sprengel's deformity include Klippel-Feil syndrome, congenital scoliosis, and torticollis. Function of the shoulder is typically good, with the limitations in abduction and forward flexion being present in moderate-severe cases. In cases which require surgery due to functional or cosmetic reasons, the average level of shoulder abduction is around 90 degrees.Ans2
|