Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
66 Cards in this Set
- Front
- Back
|
What is the pathologic effect of acute necrotizing pancreatitis on alveoli?
|
Alveolar membrane hyalinosis
Major risk factor for progression to ADRS |
|
|
What is the genetic pathophysiology of Turner's Syndrome?
|
Classically, complete monosomy of 45 XO in 50-60% of Turner patients with another 30% demonstrating mosaicism.
Remainder have structural abnlts of X chromosome. In mosaic populaiton, one genetic line contains cells w/46XX while other genetic line contains 45XO. Both lines originate from single zygote. Most cases of monosomy X due to loss of parental X chromosome during MITOSIS In cases of aneuploidy, etiology is MEITOTIC nondisjunction. Mosaicism arises secondary to MITOTIC errors. |
|

|
PPV = TP/(TP + FP)
=130/(130+60) =130/190 |
|
|
If energy-dependent organic anion transport across the hepatocellular membrane is selectively inhibited, what would be the effect on biliary excretion?
|
Liver takes up indirect (unconj'd) bilirubin through PASSIVE process.
Secretes direct (conjugated) bilirubin into biliary system through ACTIVE transport (MRP2). Inhibition of MRP2 transport protein prevents conjugated bilirubin from being excreted into biliary system. Conjugated bilirubin can still exit hepatocyte by passive diffusion through basolateral OATP (where indirect bilirubin comes in through--again, this is PASSIVE). Thus, inhibition of canalicular active organic anion transporter (MRP2) results in conjugated hyperbilirubinemia. Because conjugated bilirubin is soluble and non-toxic (and doesn't bind albumin very strongly), it can be safely excreted in urine. |
|
|
Associated heart sound:
Decreased LV compliance |
S4
|
|
|
Associated heart sound:
increased LV end-diastolic pressure |
S3--assocd w/inc'd volume of blood in LV at end of diastole; believed to occur when inflor of blood from LA strikes blood already in LV (causing reverberation of blood between left ventricular walls)
|
|
|
Which molecules are neither reabsorbed nor secreted in the nephron?
|
Inulin, Mannitol
|
|
|
Which molecules are mostly secreted in the nephron?
|
PAH, Creatinine
|
|
|
Which molecules are mostly reabsorbed in the nephron?
|
Glucose, Sodium, Urea
|
|
|
What is the role of thyroid peroxidase?
|
Iodide oxidation, and coupling that forms T3/T4
|
|
|
Horizontal nystagmus
Ophthalmoplegia Ataxia Confusion, apathy Post glucose administration Diagnosis Pathophys |
Wernicke Encephalopathy: need to give thiamine first
Damage to mamillary bodies (foci of hemorrhage and necrosis) |
|
|
Which sensory pathway does not have relay nuclei in the thalamus?
|
Olfaction
|
|
|
List the sensory nuclei in the thalamus.
|
VPL: spinothalamic, medial lemniscus
VPM: gustatory pathways, trigeminal pathways Lateral Geniculate Body: Visual Medial Geniculate Body: Auditory |
|
|
What are the effects of C. diff toxins A and B?
|
A toxin = enterotoxin; acts as neutrophil chemoattractant leading to mucosal inflammn, loss of water into lumen (producing diarrhea), mucosal death
Toxin B: actin depolymerization, resulting in LOSS OF CELLULAR CYTOSKELETON INTEGRITY, cell death, mucosal necrosis |
|
|
Hepatocytes exposed to an external stimulate demonstrate a rapid increase in intracellular glycogen stores and a decrease in glucose release into blood.
What substance is this? Describe it second-messenger cascade. |
Insulin--promotes synthesis of glycogen, triacylglycerides, nucleic acids, proteins
Inhibits glycogenolysis, and gluconeogenesis via tyrosine kinase Tyrosine kinase causes phosphorylation of substrates--> Activates protein phosphatase Dephosphorylates glycogen synthase-->activating it and promoting glycogen synthesis Also dephosphorylates Fructose 1,6-bisphosphatase, inactiving it (thus inhibiting gluconeogenesis) |
|
|
22 year-old prengnat female
Hyperglycemia does not correct with calorie restriction Treatment of choice |
INSULIN
Oral medications avoided because of risk of fetal hyperinsulinemia/hypoglycemia |
|
|
What is the effect of corticosteroid administration on CBC?
|
Corticosteroids result in demargination of neutrophils previously attached to vessel wall, thus increase neutrophil count, and a decrease in lymphocytes, monocytes, basophils, and eosinophils.
|
|
|
How do ACE inhibitors result in renal failure?
|
ACE inhibitors block Ag mediated efferent arteriole vasoconstriction, leading to a reduction in renal filtration fraction.
For pts dependent on efferent arteriole constriction to maintain renal perfusion (those with RAS), ACE-inhibitors can be detrimental by precipitating acute renal failure. |
|

Diagnosis
Treatment |
Primary Polydipsia (AKA psychogenic polydipsia)
Treat with water restriction |
|
|
At what stages do oocytes arrest?
|
Prophase of Meiosis I until ovulation
Metaphase of meiosis II until fertilization |
|
|
4 year-old male
Facial hair growth Enlarged genitalia Pubic hair growth Impaired upward gaze Diagnosis Pahtophys |
Germinoma of pineal region (histologically similar to testicular seminomas)
Result in precocious puberty due to production of beta-hCG production Compression (by mass effect) causes Parinaud Syndrome (paralysis of upward gaze) May also cause obstructive hydrocephalus due to aqueductal compression |
|
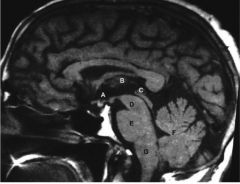
Label
|
A - Suprasellar region
B - Thalamus C - Pineal gland D - Midbrain E - Pons (locked-in syndrome occurs here!!) F - Cerebellum G - Medulla |
|
|
Erosions of buccal and gingival mucosa
Flaccid bullae with erosions over trunk Blisters spread laterally with pressure Traction on uninvolved skin produces bullae Diagnosis Pathophys |
Pemphigus vulgaris--antibodies against DESMOSOMAL proteins, namely DESMOGLEINS 3/1
|
|
|
Tense bullae over skin
Diagnosis Pathophys |
Bullous pemphigoid (no mucosal involvement!)
Antibodies against HEMIdesmosomal proteins |
|
|
42 year-old female
Fever, persistent sore throat Truncal bruising, blood oozing from venipuncture sites BM biopsy shows immature myeloid cells with giant cytoplasmic granules Diagnosis Specific translocation Treatment |
Acute promyelocytic leukemia (APL, M3 AML)--presents with persistent infection and coagulopathy
Presents with AUER rods Translocation is t(15;17) Treat with ATRA |
|
|
Philadelphia Chromosome:
Disease association Specific translocation Treatment |
CML
Results in BCR-ABL fusion protein t(9;22) |
|
|
Burkitt lymphoma translocation.
|
t(8;14), t(8;22), t(8;2)
|
|
|
25 year-old pregnant female
Amniocentesis in 25th week reveals elevated acetylcholinesterase Diagnosis Pathophys |
NT defect; if neuropore doesn't fuse, opening exists between NT and amniotic cavity.
Due to leakage of fetal CSF the following will appear in amniotic fluid: AFP, and acetylcholinesterase Due to a failure to fuse (embryonic pathophys) |
|
|
Antibodies against alpha-3 chain of collagen IV
|
Goodpasture Syndrome (these are anti-GBM antibodies)
|
|
|
Sarcoidosis:
Hypersensitivity Type |
IV
|
|
|
PSGN:
Hypersensitivity Type |
III
|
|
|
What region of bone is most likely to be affected by osteomyelitis? Why?
|
Metaphysis of Long Bones; due to rich vascularization and capillary fenestrae
|
|
|
What are the most common causes of osteomyelitis?
Pathophys? |
Staph aureus, Strep pyogenes (Group A strep); due to hemotogenous osteomyelitis (seeding of infection in normal bone)
|
|
|
What is the most common cause of osteomyelitis in diabetics?
Pathophys? |
Pseudomonas--results from chronic wounds spreading via contiguous focus of infection
|
|
|
What is the the effect of SIADH (in the setting of small cell carcinoma) on sodium content and fluid status?
Pahtophys. |
In SIADH (due to SCC), lung tumor pumps out ADH regardless of feedback.
Low serum sodium levels, depressed plasma osmolality, and elevated urine osmolality (which normally should be MAXIMALLY dilutes given hyponatremia) indicate SIADH ADH leads to excess water absorption form kidneys, causing hypervolemia initially. Excess body water suppresses renin-aldosterone axis, causing LOW aldosterone. Low aldosterone leads to natriuresis. Eventually most patients with SIADH will equilibrate with normal total body volume and exhibit EUVOLEMIC HYPONATREMIA. |
|
|
Molecular effects of morphine binding mu opioid receptors.
|
Upon binding mu receptors, morphine activates potassium channels to increase potassium EFFLUX (via G protein mechanism)
Inc'd efflux leads to hyperpolarization of postsynaptic neurons and termination of pain transmission. |
|
|
34 year-old male
Episodes of exertional syncope Harsh systolic murmur Asymmetric interventricular septum hypertrophy Father died suddenly at 30 Diagnosis Pathophys of murmur |
Hypertrophic CM (paternal history!)--common cause of v fib
In 25% cases of HCM, mitral valve comes abnormally close to interventricular septum as it bulges into LV outflow tract. Bulging is a result of asymmetric septal hypertrophy Systolic murmur heard in patient with HCM is a systolic ejection murmur produced by LV outflow tract obstruction |
|
|
Hydrychlorothiazide:
AEs |
THiazide diuretics are known for causing:
HYPER problems: -hyperuricemia -hypercalcemia -hyperglycemia -hyperLIPIDemia HYPO problems hypokalemia hypotension |
|
|
What is the hemoglobin composition of fetal hemoglobin?
When does it disappear? |
alpha2-gamma2
Disappears 6 months post-partum |
|
|
14 year-old male
Easy bruising Loose skin Multiple Ecchymoses Diagnosis Pathophys |
Ehlers-Danlos Syndrome--mutations leading to deficiencies of lysyl-hydroxylase or pro-collagen peptidase enzymes; the latter of which acts on procollagen--has formed triple helix, but still contains N/C terminal nonhelical regions.
It's exported from cell and then cleaved into collagen fibrils by procclagen peptidase. Defective cleavage at N/C termini yield more solluble collagen that doesn't properly crosslink. Results in joint laxity, loose skin, easy bruisability. Remember that this cleavage occurs outside of the cell--in the ECM. |
|

Diagnosis
Pathophys |
Ectyhma gangrenosum
Occurs after Pseudomonas aeuriginosa invades perivascularly and releases tissue destructive exotoxins causing vascular destruction Common in neutropenia patients, hospitalized patients, patients w/burns and chronic indwelling catheters |
|
|
Why is developing a vaccine against gonorrhea so challenging?
|
Gonoccoci use their pili to mediate adherence to muscosal epithelium.
Ab x specific pilus protein would prevent mucosal adherence and initiation of infection However, each gonococcus possesses ability to modify pilus protein via antigenic variation and thus avoid host defense to some degree (as well as make vaccination against this pilus protein difficult) |
|
|
14 year-old female
Sickle Cell Progressive exertional dyspnea after febrile illness HCT 18% Retic 0.5% Diagnosis Pathophys |
Reticulocyte count persists at low end of normal, describing an aplastic crisis
In sickle cell this is secondary to parvovirus B19 infection of erythroid precursor cells in BM |
|
|
Parvovirus B19:
Viral type |
non-enveloped, ss DNA
|
|
|
55 year-old woman
Acute onset headache, difficulty with vision Becomes unconsious CT reveals acute hemorrhage in left temporal lobe and compression of anterior medial temporal lobe against tentorium cerebelli Diagnosis Pathophys of findings |
Transtentorial herniation = uncal herniation--complication of ipsilateral mass lzn, such as hemorrhage or brain tumor
First sign is fixed/dilated pupil on side of lesion due to compression of CN III. Ipsilateral paralysis of oculomotor mm, contralateral or ipsilateral hemiparesis, and contralateral homonymous hemianopsia (can only see one half of visual field) with macular sparing may also occur |
|
|
How does a pituitary adenoma result in amenorrhea?
|
Release of prolactin
|
|
|
65 year-old male
Loses consciousness while buttoning a tight shirt collar Has happened before BP 70/40 HR 45/min Pathophys |
External pressure on the carotid sinuses causes baroreceptors (which sense arterial wall stretch) to react as if there were a systemic blood pressure increase.
This results in inc'd firing of GLOSSOPHARYNGEAL NERVE from carotid sinus, which will result in inc'd Psymp tone. Note that AORTIC ARCH baroreceptors carry information via VAGUS. |
|
|
Why does rectal administration of a drug have greater bioavailability than oral administration of that drug?
|
Rectal drug administration, such as with suppositories, partially bypasses first-pass (hepatic) metabolism.
Rectum is drained by superior, middle, and inferior rectal veins. Superior rectal veins drain to portal circulation via inferior mesenteric vein. Middle and inferior rectal veins, however, drain to systemic circulation via internal iliac and internal pudendal veins, respectively. Thus, 2/3 of venous drainage of rectal region goes directly into systemic circulation. |
|
|
Presence of insulin D-glucose transport across adipose membrane is much faster than __-glucose transport.
How? Name specific transporters. |
Glucose transport occurs along its [ ] gradient via transporter (without expenditure of energy-->facilitated diffusion)
Glucose transporters catalyze entrance of D-glucose rather than L-glucose into cells. GLUT4 is insulin-sensitive transporter in skeletal muscle and cardiac muscle cells, and adipocytes. Under influence of insulin, transporter protein incorporated into cell membrane. GLUT 2 located in liver, small intestine, and kidneys; facilitates EXPORT of glucose from cells. Only in intestinal and renal tubular epithelium does glucose travel against its [ ] gradient; requires energy (uses Na/glucose cotransporter) |
|
|
30 year-old male
Fever, bloody diarrhea, abdominal distention, tenderness Ulcerative colitis BP 100/70 HR 130 Diagnosis Pathophys Diagnostics |
Abdominal pain, distention, along with fever and signs of shock (dec'd BP, inc'd HR) + ulcerative colitis-->TOXIC MEGACOLON
Begins with complete cessation of neruomuscular activity in intestinal wall Rapid colonic distention ensues Prone to rupture-->perforation is life-threatening! Diagnose w/plain X-ray Barium contrast and colonoscopy are contraindicated due to risk of perforation |
|
|
Warfarin skin necrosis:
Pathophys |
Warfarin inhibits vitamin K dependent carboxylation of glutamic acid residues of clotting factors II, VII, IX, and X
Also decreases carboxylation and fn of Protein C and Protein S. Remember that activates Protein C deactivates factors V and VIII; also remember that actions of protein C are inc'd in presence of protein S Inhibition of anticoag activity of Protein C can predispose pts to wawrfarin-induced skin necrosis (usually in first week of tx) Risk is strongest in pts w/preexisting prot C deficiency |
|
|
Protein with alpha-helical secondary structure found in neurons
Undergoes conformational change to beta-pleated sheet Highly resistant to proteases Causes intracellular accumulation Diagnosis Effects |
This is describing pathogenesis of PrP (prion protein) of Creutzfeldt-Jakob dz
Results in spongiform transformation of gray matter (vacuoles within neurons/neutrophils grow into cysts and involve larger areas of brain tissue) |
|
|
58 year-old man
Decreased strength (3/5) in right hand only CT scan initially shows no abnormalities 4 weeks later, repeat brain imaging shows 9 mm lake-like cavitary lesion in internal capsule Diagnosis Pathophys |
LACUNAR INFARCT (lcus = lake in Latin): Ischemic cerebral infarct secondary to vascular occlusion
Commonly caused by atherosclerotic thrombi or by emboli from cardiac lzns Lesion turns into cystic space surrounded by scar tissue--size of necrotic area depends on diameter of occluded blood vessel |
|
|
Diagnostic criteria for Charcot-Bouchard aneurysm
|
microaneurysms <1 mm in diameter
Occur in small penetrating arterioles that perfuse basal gnaglia, pons, subcortical white matter Due to long-standing HTN Would appear as hemorrhagic stroke on initial CT scan (immediately!) as a focus of intraparenchymal hyperdesnity. |
|
|
Phenelzine:
MOA |
Inhibits monoamine oxidase-->dec'd degradation of 5HT, NE, DA
|
|
|
Why must a physician wait two weeks after discontinuing an MAOI before starting an SSRI?
Be specific. |
MAOIs such a phenelzine irreversibly bind and inhibit MOA A and B, resulting in dec'd inactivation of 5HT, NE, DA.
Takes 2 weeks (at least!) to regenerate MAO enzyme to levels adequate for normal NT metabolism. Co-administration of an SSRI and MAO can result in serotonin syndrome! |
|
|
37 year-old female
Lower abdominal discomfort Enlarged uterus Normal endometrial glands within myometrium Diagnosis |
Adenomyosis--uterine enlargement results from uterine SM hypertrophy and hyperplasia in response to ectopic endometrial glandular tissue
Other syx include menorrhagia and dysmenorrhea |
|
|
Goodpasture Syndrome:
Exact mechanism Presentation (include extrarenal symptoms) Immunofluorescence Findings |
Anti-glomerular BM antibodies that target alpha-3 chain of TYPE IV COLLAGEN (GBM is composed of collagen type IV!)
Will develop rapidly progressive GN-->RBC casts, mild proteinuria. Ab's cross-react w/other BM's, esp hose in lung alveoli, causing pulmonary hemorrhage (hemoptysis). Immunofluorescence will show linear IgG and C3 deposition, CRESCENT FORMATION on light microscopy (crescents will have FIBRIN deposition) |
|
|
3 week-old infant
Jaundice Dark urine, light-colored stools Enlarged liver, firm on palpation Biopsy shows intrahepatic cholestasis and proliferation of intrahepatic bile ducts Diagnosis |
Extrahepatic biliary atresia (congenital obstruction of extrahepatic bile ducts)
By 3rd week of life, there is TOTAL obstruction. Affected children will ahve acholic (light) stools and dark urine. Enlarged, firm liver. Lab values include inc'd direct bilirubin, alk phos, and gamma-glutamyl transferase If biliary drainage not restored surgically, bile stasis will cause dev't of biliary cirrhosis by 6 months. |
|
|
A chemotherapeutic agent classified as a guanosine derivative demonstrates significant antiviral activity against HSV1, HSV2, and VZV.
The same agent demonstrates weak antiviral activity against EBC and CMV. What accounts for this difference? |
Drug described is likely acyclovir (a guanosine analog)
Once acyclovir enters herpes-infected host cell, it's converted to acyclovir monophosphate via virally-encoded thymidine kinase. This is the RLS in activation of acyclovir. EBV and CMV do not produce the same thymidine kinase that HSV and VZV do. As a result, EBV or CMV infected cells cannot easily convert acyclovir into its active triphosphate form. |
|
|
What are the normal morphological changes in the aging heart?
|
Decrease in LV chamber apex-t-base dimensions (not hypertrophy)
Sigmoid-shaped ventricular septum Myocyte atrophy with interstitial fibrosis Accumulation of cytoplasmic lipofuscin pigment Note that hypertensive heart dz is assocd w/concentric hypertrophy of LV |
|
|
How do beta-blockers mask the symptoms of hypoglycemia?
|
Mask adrenergic syx of hypoglycemia by blocking beta-receptors
|
|
|
What nerve is blocked intravaginally during child birth?
|
Pudendal
|
|
|
65 year-old female
Poor memory, urinary incontinence, gait abnormalities Enlarged ventricular system Minimal cortical atrophy Diagnosis Pathophys of Presentation |
Normal pressure hydrocephauls--dec'd absorption of CSF leads to inc'd CSF volume, which is accommodated by ventricular enlargement
Expanded ventriculi place traction on cortical efferent and afferent fibers. This disrupts pathways that transmit impulses from cortex to sacral micturition center Later in dz, lack of inhibition from cerebral cortex leads to frequent and uncontrolled micturition or urge incontinence. Bladder fills w/urine and empties reflexively when full. Patient has no sensation of bladder fullness and no control over bladder fn. Voluntary relaxation of urethral sphincter remains intact. (In short, incontinence due to stretching of cortical fibers; not cerebellar inhibitory fibers) |
|
|
Murmur accentuated with handgrip
|
VSD (not PDA!)
Increases with handgrip due to increased afterload Small VSDs often asyx and detected incidentally during routine cardiac auscultation |
|
|
How does COPD result in polycythemia?
|
COPD-->hypoxia sufficient to stimulate inc'd EPO production by kidney-->inc'd RBC production
|