Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
68 Cards in this Set
- Front
- Back
|
location, relationships, features and neurovascular supply of the kidneys
|
-
|
|
|
relationship of the renal fascia to the kidneys and suprarenal glands
|
-
|
|
|
• Define the term end artery and explain the significance of this with respect to the segmental arteries of the kidneys
|
-
|
|
|
structure, length, course and relationships of the ureters including relationship to the peritoneum
|
-
|
|
|
locations of the 3 constriction points along the ureter and the relationship of these to ureteric colic
|
-
|
|
|
location and relationships of the bladder, its internal and external features and neurovascular supply
|
-
|
|
|
location and shape of the bladder in a newborn and adult
|
-
|
|
|
the range of developmental anomalies related to kidney, ureter and bladder development
|
-
|
|
|
Compare and contrast the urethra in both sexes and describe the location and innervation of the urethral sphincters
|
-
|
|
|
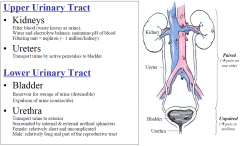
Urinary Tract; 2 sections
|
|
|
|
UTIs
|
Cystitis: lower (commonly called UTI)
Polynephritis: upper UTI |
|
|
Kidneys - Size
|
Size approximately 10 x 5 x 2.5 cm, retroperitoneal, right kidney lower than left, tilted in 2 planes (superior poles closer; anterior surfaces slightly lateral)
|
|
|
Kidneys - Location
|
|
|
|
Kidneys: Layers
|
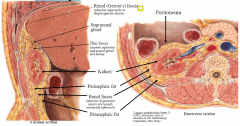
1. kidney
2. Thin fascia 3. perinephric fat 4. renal fascia (tight superior at the diaphragm fascia and loose inferiorly) 5. Paranephric fat |
|
|
Functions of the Kidney Layers
|
The fat and fascia help to maintain the position of the kidney
Loss of supporting fat (eg. anorexia) renal ptosis with potential kinking of ureters hydronephrosis Kidneys move vertically during respiration & when moving from supine to upright position Attachments of renal fascia determines direction of spread of infection (renal abscess) & blood (injury) spreads inferiorly due to loose attachment of anterior & posterior layers of renal fascia inferior to kidney |
|
|
Kidneys – External Features
|
Renal capsule (dense, fibrous, glistening appearance) on surface of kidney, extends into renal sinus
Renal hilum is a 1 cm long cleft on medial border through which structures enter/exit, it leads into the renal sinus Structures passing through hilum include renal artery and vein, renal pelvis, nerves and lymphatics |
|
|
Neurovascular Supply Kidney
|
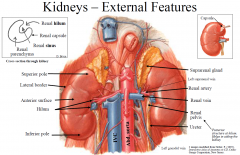
Ant. to Post.
1. Renal v. 2. renal a. 3. renal pelvis |
|
|
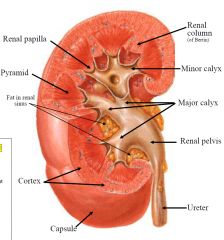
Kidneys – Internal Features
|
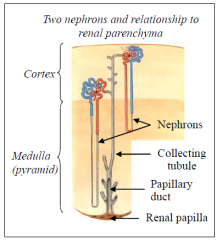
- Renal cortex around periphery; it extends between pyramids as the renal columns
- Renal medulla = collection of renal pyramids - Renal pyramids contain collecting tubules which open at renal papilla (apex of pyramid) - Renal papilla indents each minor calyx - Minor calyces join to form major calyces - 2-3 major calyces join to form renal pelvis - Renal pelvis is funnel-shaped, it narrows to form ureter |
|
|
Kidneys Internal Macrscopic Look
|
|
|
|
Kidneys – Blood supply
|
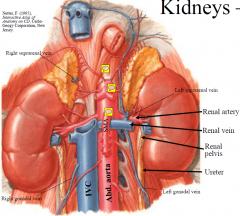
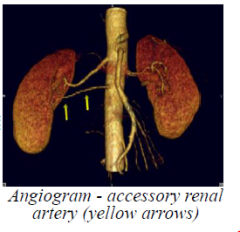
Left & right renal arteries are branches of the abdominal aorta (L2 level) and receive ~20-25% cardiac output
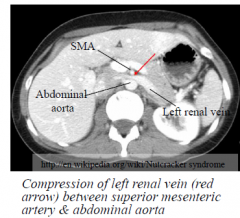
Lie posterior to the renal veins. The right renal artery passes posterior to the IVC Accessory renal artery is present in ~30% of population; usually a branch of the abdominal aorta Left & right renal veins drain to IVC. Left renal vein receives the left suprarenal vein and left gonadal vein Left renal vein passes in angle between the SMA & abdominal aorta and can be prone to entrapment (Nutcracker syndrome). This may cause haematuria, left flank pain and maybe a cause of left-sided varicocoele and/or left testicular pain |
|
|
Nutcracker Syndrome
|
|
|
|
Accessory renal artery
|
|
|
|
Kidney BS to the panrynchyma
|
|
|
|
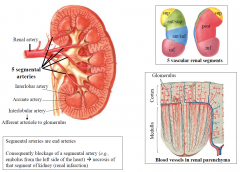
Kidney End Arteries
|
Consequently blockage of a segmental artery (e.g., embolus from the left side of the heart) necrosis of that segment of kidney (renal infarction)
|
|
|
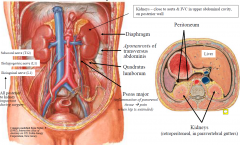
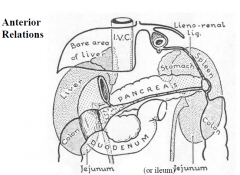
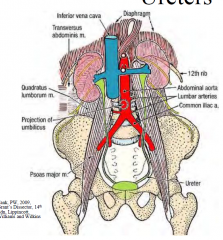
Kidneys - Relationships
|
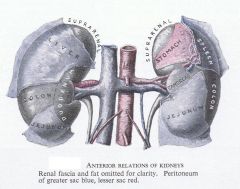
Anterior relations
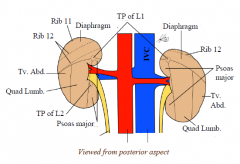
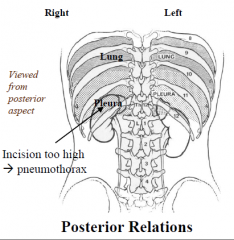
Left kidney: suprarenal gland, colon, jejunum, stomach, spleen, pancreas Right kidney: suprarenal gland, colon, jejunum/ileum, duodenum, liver Posterior relations 4 muscles - diaphragm, psoas major, quadratus lumborum, aponeurosis of transversus abdominis; 12th rib post to right kidney; 11th & 12th rib post to left kidney (# ribs damage to kidney blood in urine); 3 nerves (subcostal, iliohypogastric, ilioinguinal - potential damage with kidney surgery); subcostal artery & vein |
|
|
Posterior Kidney relations
|
|
|
|
Anterior Kidney Relations
|
|
|
|
Enlarged left kidney vs. Enlarged spleen
|

•Kidney retroperitoneal and can feel space between enlarged kidney & costals
•Kidney moves inferiorly with inspiration, but spleen moves obliquely (towards umbilicus) •Percussion usually resonant over kidney (due to gas in overlying bowel) but dull over spleen •Notched border of spleen may (or may not) be palpable |
|
|
Kidney Transplant
|
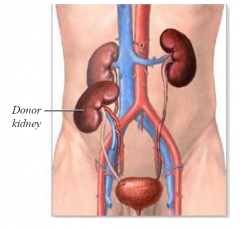
•Donor kidney transplanted iliac fossa (extraperitoneal)
•Donor’s renal artery & vein connected to external iliac vessels, ureter connected to bladder •Patient’s kidneys usually remain in place |
|
|
Ureters
|
Ureters 25 cm long, expansible tubes of smooth muscle; 3-5 mm wide; extend from renal pelvis to bladder; upper ½ in abdominal cavity, lower ½ in pelvic cavity; midpoint crosses pelvic brim anterior to bifurcation of common iliac artery; passes obliquely through bladder wall; ends at ureteric orifice in urinary bladder
|
|
|
BS of ureters
|
Blood supply From adjacent arteries, which anastomose along ureter
|
|
|
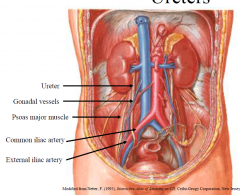
Ureters – Course
|
Abdominal course: retroperitoneal; almost vertical on psoas major, crossed anteriorly by gonadal vessels
Pelvic course: extraperitoneal; from pelvic brim passes posterolaterally on pelvic wall, then at level of ischial spine turns medially and anteriorly towards bladder “Water under the bridge” in male & female; “bridge” = ductus deferens in male; uterine artery in female |
|
|
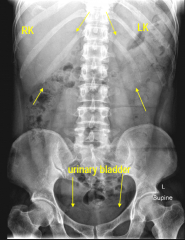
Ureters: Radiographically
- before a CT scan lookinf for colic |
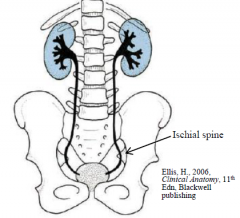
In searching for a ureteric stone on a plain radiograph of the abdomen, one must imagine the course of the ureter in relation to the bony skeleton. It lies along the tips of the transverse processes, crosses in front of the sacroiliac joint, swings out to the ischial spine and then passes medially to the bladder. An opaque shadow along this line is suspicious of calculus. This course of the ureter is readily studied by examining a radiograph showing a radio-opaque ureteric catheter in situ.
|
|
|
Ureters Constriction Points
|
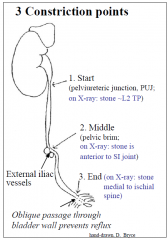
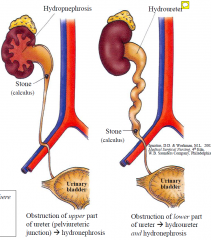
3 sites of constriction/narrowing along ureter where ureteric calculus may lodge.
+/- ureteric colic (loin to groin pain); +/- hydroureter and hydronephrosis (with progressive renal parenchymal damage) |
|
|
Hydroureters or Hydronephrosis
|
|
|
|
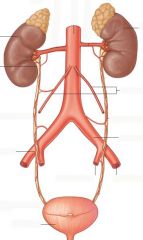
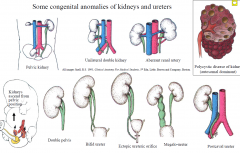
Development – Kidneys, Ureter
Some congenital anomalies of kidneys and ureters |
|
|
|
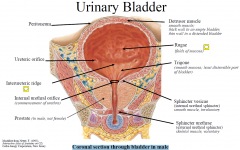
Urinary Bladder
Internal features: |
Rugae - folds of mucous membrane in empty bladder that disappear as bladder distends
Trigone - triangular area situated posteriorly limited by 2 ureteric orifices and an internal urethral orifice An interureteric ridge/crest extends between the ureteric orifices |
|
|
Coronal section through bladder in male
|
|
|
|
Bladder – Relationships in Female
|
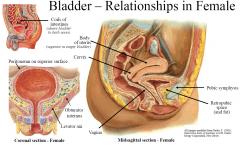
Anterior - retropubic space and pubic bone/pubic symphysis
Superior - coils of intestines and body of uterus Inferolateral - levator ani & obturator internus Posterior - cervix of uterus and vagina (not rectum) |
|
|
Bladder – Relationships in Male
|

Anterior - retropubic space and pubic bone/pubic symphysis
Superior - coils of intestines Inferolateral - levator ani (is a part of pelvic diaphragm) & obturator internus Inferior - prostate Posterior - rectum, ductus deferens, seminal vesicles |
|
|
Urethra - Female
|
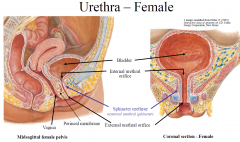
-Female urethra commences at internal urethral orifice at neck of bladder,
-Ends at external urethral orifice (in the vestibule of vagina between vaginal opening and clitoris). -Approximately 4 cm long, passes anteriorly and inferiorly (important to understand for catheterisation), -Passes through pelvic diaphragm, surrounded by external urethral sphincter (skeletal muscle, voluntary) -Urethra is short; therefore females are prone to lower urinary tract infections |
|
|
Urethra – Male
|
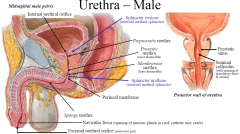
- Male urethra commences at internal urethral orifice at neck of bladder, ends at external urethral orifice
- 4 parts: preprostatic (through bladder neck; surrounded by sphincter vesicae); prostatic (~3 cm); membranous (~ 1cm; though sphincter urethrae and perineal membrane); spongy or penile (~15 cm, corpus spongiosum & glans penis). - The prostatic part (widest & most dilatable part) has an elevation (seminal colliculus) that receives openings of the ejaculatory ducts and utricle |
|
|
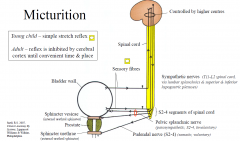
Micturition
4 components |
1. Sympathetic nerves are excitatory to smooth muscle of bladder base, neck & proximal urethra & have an inhibitory effect
2. Visceral afferents detect bladder stretch; stretch information travels with pelvic splanchnic nerves S2-4 segments of spinal cord connections to higher centres desire to micturate. Micturition inhibited by higher centres until a convenient time. NOT YET DEVELOPED IN CHILDREN 3. Parasympathetic fibres travel via pelvic splanchnic nerves contraction of detrusor muscle and relaxation of sphincter vesicae. 4. Voluntary component of bladder emptying involves relaxation of pelvic diaphragm & sphincter urethrae. Higher centres do not control micturition until 2-3 years, prior to this bladder empties reflexly |
|
|
Micturition Process
|
|
|
|
X-rays
|

- plain radiograph
- radiograph + contrast - CT scan - CT + Contrast |
|
|
Contrast media
|
negative agents air carbon dioxide positive agents iodine-containing water-soluble media e.g. iohexol, iopamidol barium oily media |
|

|
stag horn calculus (not contrast medium)
|
|
|
Nuclear Medicine
|

DMSA – taken up by functioning tubules DTPA, MAG3 – filtered and concentrated by kidney in the same way as radiographic, CT and MRI contrast media graphical recording with time on y-axis & activity on x-axis |
|
|
Ultrasound and Doppler
|
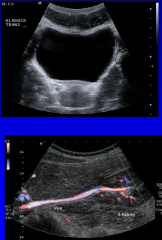
sound reflected back from tissue interfaces time difference indicates distance of interface Doppler ultrasound used to measure blood flow safe so usually the first diagnostic imaging test |
|
|
Nuclear magnetic resonance
|

magnetism and radio-frequency waves
images show multiple different tissue characteristics contrast media based on Gd-DTPA behave like x-ray CT contrast media NMR spectroscopy identifies chemical constituents |
|

|
Horseshoe kidney
|
|
|
Relation to skeleton
|
kidney L1 to umbilicus covered by 12th rib 3 vertebral bodies long in the adult about 9-13 cm long left usually lies slightly superiorly to right (because of liver) |
|
|
Orientation of kidneys
|
lower pole anterior to upper pole lower pole lateral to upper pole hilum anteromedial |
|
|
Variations in position of kidney
|
normal respiratory movement ptotic or pelvic kidney malrotated kidney horse-shoe kidney duplicated ureter |
|
|
Relations with other organ
|
|
|
|
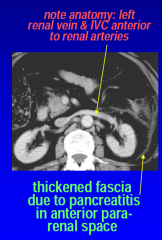
Retroperitoneal fascial spaces
|
|
|
|
Lobar anatomy
|
embryological origin from many lobes (like a bunch of grapes) progressive fusion of lobes continues after birth foetal lobation or “lobulation” may persist on renal surface |
|
|
Kidney on ultrasound
|
size easily measured fat in renal sinus white medulla darker than cortex cortex darker than liver collecting system normally collapsed blood vessels resemble collecting system unless colour Doppler US turned on |
|
|
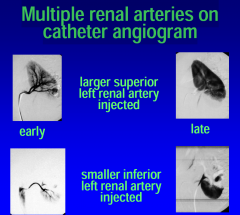
Multiple renal arteries on catheter angiogram
|
|
|
|
Nephrogram phase of intravenous pyelogram (IVP)
|

tomogram using a moving x-ray tube and film to blur overlapping structures – now replaced by CT
|
|
|
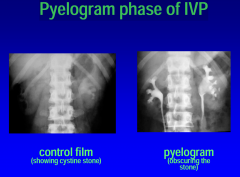
Pyelogram phase of IVP
|
|
|
|
DMSA scintigram
|
DMSA binds to renal tubular cells maps normal functioning kidney |
|
|
DTPA scintigram
|
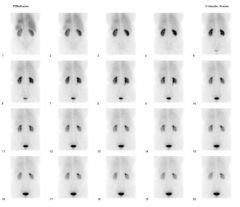
injected bolus circulates to whole of body first pass through kidney monitored injected agent clears to interstitial fluid throughout body urine |
|
|
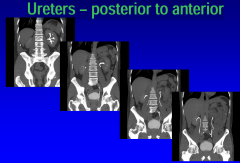
Ureters – posterior to anterior
|
|
|
|
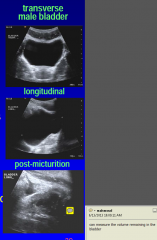
Bladder US
|
|
|
|
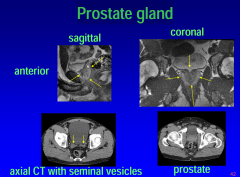
Prostate gland Imaging
|
|
|
|
Male urethra
|
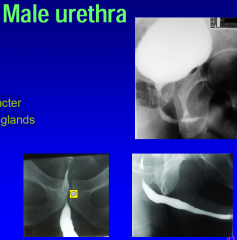
prostatic part membranous external sphincter bulbourethral glands bulbar urethra penile urethra |
|
|
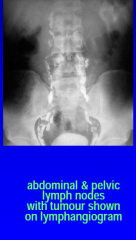
lymph angeogram (oil filled contrast)
|
|