Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
3 Cards in this Set
- Front
- Back
|
asdfas
|
sdfasf
|
|
|
External Ventricular Device waveform
|
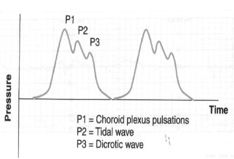
Interpretation of Waveforms
- High amplitude of 50-100mmHg sustained for 15 min (‘A waves’) – raised ICP - Saw tooth with small changes in pressure every 0.5-2 minutes (‘B waves’) – poor intracranial compliance - Low amplitude oscillations up to 20mmHg for 1 min (‘C waves’) – normal - Flat ICP trace – compression or kinking of transducer - Rounded appearance of the waveform – raised ICP |
|
|
Increased intracranial pressure management
|
exclude artefact/measurement errors
ensure adequate oxygen delivery — PaO2 — treat clinically significant anaemia maintain cerebral perfusion pressure to > 60mmHg (CPP = MAP – ICP) – fluids (avoid albumin–SAFE TBI) — inotropes, vasopressors optimise venous return from brain: — head up positioning, no venous obstruction (remove hard collar), low PEEP avoid cerebral vasoconstriction — PaCO2 35-40mmHg decrease cerebral metabolic rate: — sedation, analgesia — paralysis — avoid hyperthermia — treat seizures — barbiturate coma osmotherapies: —mannitol 0.25 to 1 g/kg, target Osm 300-320 mOsm/kg — hypertonic saline, target Na+ 145-155 Repeat CT scan to exclude a new mass lesion Consider hypothermia (decrease cerebral metabolism, possible neuroprotection) — Adverse outcome in paediatric TBI RCT from CCCTG — McIntyre MA suggesting titrated to ICP and prolonged duration maybe beneficial — Ongoing trials including POLAR in ANZ Consider surgical techniques (to reduce volume in the ‘box’, or to ‘ope |