![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
254 Cards in this Set
- Front
- Back
|
What 3 categories is the distal limb divided into? |
Foot, lower leg, distal femur |
|
|
How many bones are in the foot? |
26 |
|
|
How many phalanges are there? |
14 |
|
|
How many metatarsals are there? |
5 |
|
|
How many tarsals are there? |
7 |
|
|
What are two differences between the phalanges of the foot and hand? |
Foot phalanges are smaller and have less movement |
|
|
What are the instep bones? |
Metatarsals |
|
|
The base of the 5th metatarsal expands laterally into this |
A rough tuberosity, which provides for the attachment of a tendon |
|
|
What is the most commonly fractured metatarsal? |
The fifth metatarsal |
|
|
Between the proximal and distal phalanges of the first digit |
Interphalangeal joint |
|
|
The Joint at the head of the metatarsal |
Metatarsophalangeal joint |
|
|
The largest sesamoid bone in the body |
Patella |
|
|
Where are the sesamoid bones of the foot usually located? |
The posterior or plantar surface at the head of the first metatarsal near the first MTP joint |
|
|
The names of the two sesamoid bones on the first metatarsal |
Tibial sesamoid and fibular sesamoid |
|
|
Why are the sesamoid bones in the lower extremities more important radiographically than the ones in the upper extremities? |
It is possible to fracture the sesamoid bones in the lower extremities |
|
|
What are the names of the seven tarsal bones? |
Calcaneus, Talus, cuboid, navicular, medial cuneiform, intermediate cuneiform, lateral cuneiform |
|
|
The alternate name for the calcaneus |
Os calcis |
|
|
The alternate name for the talus |
Astragalus |
|
|
The alternate name for the navicular |
Scaphoid |
|
|
The calcaneus articulates anteriorly with which bone? |
Cuboid |
|
|
The calcaneus articulates superiorly with which bone? |
Talus |
|
|
The superior articulation of the talus and calcaneus forms which important joint? |
Subtalar joint |
|
|
What are the names of the three articular facets that appear at the subtalar joint? |
Posterior articular facet, anterior articular facet, middle articular facet |
|
|
The deep depression between the posterior and middle articular facets |
Calcaneal sulcus |
|
|
An opening formed by the calcaneal sulcus and a groove of the talus. Allows certain ligaments to pass through |
Sinus tarsi |
|
|
The second largest tarsal bone |
Talus |
|
|
The talus articulates with which bones superiorly? |
Tibia and fibula |
|
|
The talus articulates inferiorly with which bone? |
Calcaneus |
|
|
The talus articulates anteriorly with which bone? |
Navicular |
|
|
A flattened, oval bone located on the medial side of the foot between the talus and the three cuneiforms |
Navicular |
|
|
The navicular articulates posteriorly with which bone? |
Talus |
|
|
The navicular articulates laterally with which bone? |
Cuboid |
|
|
The navicular articulates anteriorly with which bones? |
The three cuneiforms |
|
|
What does cuneiform mean? |
Wedge-shaped |
|
|
The largest cuneiform |
Medial cuneiform |
|
|
The smallest cuneiform |
Intermediate cuneiform |
|
|
All three cuneiforms articulate with which bone proximally? |
Navicular |
|
|
The medial cuneiform articulates with which bone distally? |
The first and second metatarsals |
|
|
The medial cuneiform articulates with which bone laterally? |
The intermediate cuneiform |
|
|
The intermediate cuneiform articulates with which bone distally? |
The second metatarsal |
|
|
The intermediate cuneiform articulates with which bones on either side? |
The medial and lateral cuneiforms |
|
|
The lateral cuneiform articulates with which Bones distally? |
The second, third, and fourth metatarsals |
|
|
The lateral cuneiform articulates with which bone medially? |
The intermediate cuneiform |
|
|
The lateral cuneiform articulates with which bone laterally? |
The cuboid |
|
|
The cuboid articulates with which Bones medially? |
The lateral cuneiform and navicular |
|
|
The cuboid articulates with which Bones distally? |
The fourth and fifth metatarsals |
|
|
The bones of the foot are arranged in these two arches |
Longitudinal and transverse arches |
|
|
The arch of the foot that is located primarily along the plantar surface of the distal tarsals and the tarsometatarsal joints |
Transverse Arch |
|
|
The ankle joint is formed by which three bones? |
The distal tibia, the distal fibula, and the talus |
|
|
The expanded distal end of the fibula |
Lateral malleolus |
|
|
The medial elongated process of the tibia that extends down alongside the medial Talus |
Medial malleolus |
|
|
The Deep socket formed by the inferior portions of the tibia and fibula |
Mortise |
|
|
Why is the mortise not seen on a true frontal view of the ankle? |
Because of overlapping of portions of the distal fibula and tibia by the talus |
|
|
Which projection demonstrates the mortise of the ankle? |
AP oblique projection, with a 15 degree internal rotation |
|
|
An expanded process at the distal anterior and lateral tibia that has been shown to articulate with the superior lateral talus, while partially overlapping the fibula interiorly |
Anterior tubercle |
|
|
The distal tibial joint surface that forms the roof of the ankle mortise joint |
Tibial plafond (ceiling) |
|
|
The distal fibula is how many centimeters posterior to the distal tibia? |
1 cm |
|
|
The intermalleolar plane has what degree of rotation from the coronal plane? |
15-20° |
|
|
The weight-bearing bone of the lower leg |
Tibia |
|
|
The tibial spine is also known as what? |
Intercondylar eminence |
|
|
The two small pointed prominences located on the superior surface of the tibial head between the two condyles |
Medial and lateral intercondylar tubercles |
|
|
The articular facets making up the tibial plateau slope posteriorly how many degrees? |
10-20° |
|
|
A rough-textured prominence located on the mid anterior surface of the tibia just distal to the condyles |
Tibial tuberosity |
|
|
The distal attachment of the patellar tendon |
The tibial tuberosity |
|
|
A condition in which the tibial tuberosity separates from the body of the tibia |
Osgood-Schlatter disease |
|
|
A sharp ridge that extends from the tibial tuberosity to the medial malleolus |
The anterior crest |
|
|
This is often referred to as the shin bone |
Anterior crest of the tibia |
|
|
The short pyramid-shaped process on the distal extremity of the tibia |
Medial malleolus |
|
|
Located on the lateral aspect of the distal extremity of the tibia. For articulation with the distal fibula |
Fibular notch |
|
|
How is the fibula located to the tibia? |
Laterally and posteriorly |
|
|
The extreme proximal aspect of the fibular head |
The apex of the head of the fibula |
|
|
The smooth, shallow, triangular depression at the distal portion of the anterior femur that extends up under the lower part of the patella |
The patellar surface, or intercondylar sulcus, or trochlear groove |
|
|
When the leg is fully extended, where is the patella located in relation to the patellar surface? |
Superior to the patellar surface |
|
|
When the leg is flexed, where is the patella located in relation to the patellar surface? |
Distally over the patellar surface |
|
|
Why must the CR be angled 5 to 7 degrees cephalad for a lateral knee? |
The medial condyle extends more distally than the lateral condyle when the femoral shaft is vertical. With an angle, it will cause the two condyles to be directly superimposed when the femur is parallel to the IR |
|
|
What is the distinguishing difference between the medial and lateral condyles? |
The adductor tubercle, which is located on the medial condyle on the posteriolateral aspect |
|
|
Rough prominences which are attachment sites for the medial and lateral collateral ligaments |
Medial and lateral epicondyles |
|
|
Where is the patella embedded? |
In the tendon of the large quadriceps femoris muscle |
|
|
The posterior surface of the distal femur just proximal to the intercondylar fossa |
Popliteal surface |
|
|
Approximately what is the diameter of the patella? |
2 in |
|
|
Describe the outer anterior surface of the patella |
Convex and rough |
|
|
Describe the inner posterior surface of the patella |
Smooth and oval shaped for articulation with the femur |
|
|
What is the purpose of the patella? |
Serve to protect the anterior aspect of the knee joint, and acts as a pivot to increase the leverage of the large quadriceps femoris muscle |
|
|
When is the patella loose and movable? |
When it's in its more superior position when the leg is extended and the quadriceps muscles are relaxed |
|
|
When is the patella locked into position? |
When the leg is flexed and the muscles tighten |
|
|
What is the bone that the patella articulates with? |
Femur |
|
|
Why is the proximal fibula not part of the knee joint? |
It doesn't articulate with any aspect of the femur |
|
|
What are some of the important ligaments in the knee area? |
Fibular lateral collateral ligament, medial collateral ligament, posterior cruciate ligament, anterior cruciate ligament |
|
|
What are the purposes of the two collateral ligaments of the knee? |
To prevent adduction and abduction movements at the knee |
|
|
What's the purpose of the cruciate ligaments? |
They stabilize the knee joint by preventing anterior or posterior movement within the knee joint |
|
|
Where is the infrapatellar fat pad located? |
Posterior to the patellar ligament |
|
|
What is the purpose of the patellar ligament? |
To maintain the Integrity of the knee joint |
|
|
The largest joint space of the human body |
The articular cavity of the knee joint |
|
|
Crescent shaped fibrocartilage discs between the articular facets of the tibia and the femoral condyle |
Medial and lateral menisci |
|
|
All of the joints of the lower limb except one are classified as what kind of joints? |
Synovial joints |
|
|
Which joint of the lower limb is considered diarthrodial? |
Distal tibiofibular joint |
|
|
To decrease the angle between the dorsum pedis and the anterior part of the leg is to do what? |
Dorsiflex |
|
|
Extending the ankle joint or pointing the toe and foot downward with respect to the normal position |
Plantar flexion |
|
|
Inward-turning or bending of the ankle and subtalar joints |
Inversion |
|
|
Outward turning or bending of the ankle and subtalar joints |
Eversion |
|
|
Most sprained ankles result from an accidental what? |
Forced inversion or eversion |
|
|
What kind of joints are interphalangeal joints? |
Ginglymus or hinge |
|
|
What kind of joints are metatarsophalangeal joints? |
Modified ellipsoidal or condyloid |
|
|
What kind of joints are tarsometatarsal joints? |
Plane or gliding |
|
|
What kind of joints are intertarsal joints? |
Plane or gliding |
|
|
What kind of joint is the ankle joint? |
Saddle or Sellar |
|
|
What kind of joint is the femorotibial knee joint? |
Bicondylar |
|
|
What kind of joint is the patellofemoral knee joint? |
Saddle or sellar |
|
|
What kind of joint is the proximal tibiofibular joint? |
Plane or gliding |
|
|
What is the most common SID for lower limb radiographs? |
40 in or 102 cm |
|
|
What kind of shield may be used? |
Gonadal Shield |
|
|
What kvp should be used? |
70-85 |
|
|
For a small to medium plaster cast, what should the increase in kvp be? |
Increase 5 to 7 kVp |
|
|
For a large plaster cast, what should the increase in kvp be? |
Increase 8 to 10 kvp |
|
|
For a fiberglass cast, what should the increase in kvp be? |
Increase 3 to 4 kvp |
|
|
What is the CR angle for an AP projection of the toes? |
Between 10 and 15 degrees |
|
|
What is the kvp range for projections of the toes and sesamoids? |
55 to 65 kvp |
|
|
Where's the CR centered for an AP and Oblique projection of the toes? |
To the MTP joint in question |
|
|
What is the degree of rotation in the leg and foot when taking an AP oblique of the first, second, and third digits? |
30 to 45 degrees medially |
|
|
What is the degree of rotation in the leg and foot when taking an AP oblique of the fourth and fifth digits? |
30 to 45 degrees laterally |
|
|
How much of the toe should be demonstrated on an AP or AP oblique projection of the toes? |
All the way to the proximal half of the metatarsal |
|
|
How do you prevent superimposition on a lateral projection of the toes? |
Use tape, gauze, or a tongue blade to flex and separate unaffected toes |
|
|
How is the leg and foot rotated for a lateral projection of the first, second, and third digits? |
Medially |
|
|
How is the leg and foot rotated for a lateral projection of the fourth and fifth digits? |
Laterally |
|

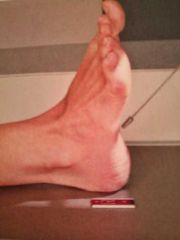
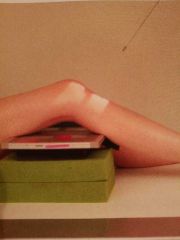
What projection is this? |
Tangential projection of the sesamoids |
|
|
How is the foot positioned for a tangential projection of the sesamoids? |
Dorsiflex the foot so that the plantar surface of the foot forms about a 15 to 20 degree angle from vertical. Dorsiflex the first digit and rest on IR to maintain position |
|
|
What is the CR method for tangential projection of the sesamoids? |
CR perpendicular to IR, directed to the first MTP joint |
|
|
What is the CR angle for an AP projection of the foot? |
10 degrees towards the heel |
|
|
Do we usually rotate the foot medially or laterally for an AP oblique projection of the foot? |
Medially |
|
|
Why would we rotate the foot laterally for an AP oblique projection of the foot? |
A lateral oblique best demonstrates the space between the first and second metatarsals and between first and second cuneiforms. The navicular is also as well visualized on the lateral oblique |
|
|
Where is the CR directed in a lateral projection of the foot? |
To the medial cuneiform, at level of base of third metatarsal |
|
|
What is the purpose of an AP weight-bearing projection of the foot? |
To demonstrate the bones of the feet to show the condition of the longitudinal arches under the full weight of the body |
|
|
What is the CR method for an AP weight-bearing projection of the foot? |
CR is angled 15° posteriorly to mid point between feet at level of base of metatarsals |
|
|
What is the patient position for a lateral weight-bearing projection of the foot? |
Patient stands on wood blocks in order to elevate foot from the ground |
|
|
What is the CR method for a lateral weight-bearing projection of the foot? |
CR is horizontal, directed to level of base of third metatarsal |
|
|
What is the IR size for projections of the toes? |
8 x 10 |
|
|
What is the IR size for a tangential projection of the sesamoids? |
8 × 10 |
|
|
What is the IR size for projections of the feet? |
10 x 12 |
|
|
What is the IR size for an AP weight-bearing projection of the foot? |
10 x 12, or 14 x 17 for bilateral study |
|
|
What is the IR size for a plantodorsal projection of the calcaneus? |
8 by 10 |
|
|
What is the kvp range for a plantodorsal projection of the calcaneus? |
65 - 75 |
|
What projection is this? |
Plantodorsal projection of the calcaneus |
|
|
For a plantodorsal projection of the calcaneus, where is the CR directed and what is the degree of the CR? |
CR directed to base of third metatarsal to emerge at a level just distal to lateral malleolus, and CR is angled 40 degrees cephalic from long axis of foot |
|
|
Is a lateral projection of the calcaneus done mediolaterally or lateromedially? |
Mediolaterally |
|
|
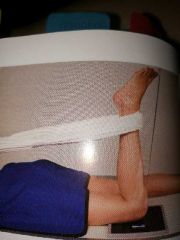
How is the lateral projection of the calcaneus positioned? |
Ankle and foot will be in a true lateral position, which places the lateral malleolus about 1 cm posterior to the medial malleolus. Dorsiflex foot so that planter surface is at right angle to leg. |
|
|
Where is the CR directed for a lateral projection of the calcaneus? |
CR perpendicular to IR, directed to a point 1inch inferior to medial malleolus |
|
|
What is the IR size for a lateral projection of the calcaneus? |
8 x 10 |
|
|
What is the IR size for a projection of the ankle? |
10 x 12 |
|
|
How is an AP projection of the ankle positioned? |
Foot is not forced into dorsiflexion; allow it to remain in its natural position. Foot and Ankle are adjusted for a true AP projection. Ensure that the entire lower leg is not rotated. The intermalleolar line should not be parallel to IR |
|
|
What is the CR method for an AP projection of the ankle? |
CR is perpendicular to IR, directed to a point midway between malleoli |
|
|
How much anatomy is demonstrated on an AP projection of the ankle? |
To include proximal 1/2 of metatarsals and distal tibia-fibula |
|
|
What are the three routine projections of an ankle? |
AP, AP mortise, lateral |
|
|
How is an AP mortise projection of the ankle positioned? |
Foot remains in natural extended position. Internally rotate entire leg and foot about 15 to 20 degrees until intermalleolar line is parallel to IR |
|
|
How is an AP oblique projection of the ankle positioned? |
Patient may dorsiflex the foot if needed so that the plantar surface is at least 80 to 85 Degrees from IR. Rotate leg and foot medially 45°. |
|
|
For a lateral projection of the ankle, do we usually position it mediolaterally or lateromedially? |
Mediolaterally |
|
|
How is a lateral projection of the ankle positioned? |
Leg and foot are in a true lateral position. Dorsiflex foot so that plantar surface is at a right angle to leg or as far as the patient can tolerate. |
|
|
What is the CR method for a lateral projection of the ankle? |
CR is perpendicular to IR, directed to medial malleolus |
|
|
What does an AP stress projection of the ankle demonstrate? |
Pathology involving ankle joint separation secondary to ligament tear or rupture |
|
|
How is an AP stress projection of the ankle positioned? |
Dorsiflex the foot as near the right angle to the lower leg as possible. Stress is applied with leg and ankle and position for a true AP with no rotation, where in the entire plantar surface is turned medially for inversion and laterally for eversion |
|
|
What are the routine projections for the tibia and fibula? |
AP and lateral |
|
|
What is the SID for projections of the tibia and fibula? |
40in for portrait, and 44 to 48 for diagonal |
|
|
What is the IR size for a projection of the tibia and fibula? |
14 x 17 |
|
|
How is an AP projection of the lower leg positioned? |
Foot is dorsiflexed to 90° if possible. Both ankle and knee joints are 1 to 2 inches from ends of IR. If the limb is too long, place the lower leg diagonally from corner to corner on IR to ensure that both joints are included. |
|
|
How is the lateral projection of the lower leg positioned? |
Leg is placed in a true lateral position with the plane of the patella perpendicular to IR. |
|
|
When is the projection of the knee taken in the bucky? |
When the knee is greater than 10 cm |
|
|
What is the IR size for a knee? |
10 x 12 |
|
|
What are the routine projections of the knee? |
AP, oblique medial, oblique lateral, lateral |
|
|
How is an AP projection of the knee positioned? |
Center leg and knee to CR. Rotate leg internally three to five degrees for a true AP knee. |
|
|
What is the CR method for an AP projection of the knee? |
CR 3-5 degrees cephalad. CR is directed to a point 1/2 in distal to apex of patella |
|
|
For an AP projection of the knee on a person with thin thighs and buttocks, what is the angulation of the CR? |
3-5° caudad |
|
|
For an AP projection of the knee on a person with average thighs and buttocks, what is the angulation of the CR? |
0° |
|
|
For an AP projection of the knee on a person with thick thighs and buttocks, what is the angulation of the CR? |
3-5° cephalad |
|
|
For medial AP oblique projection of the knee, what is the rotation of the leg? |
45° medially |
|
|
What is the CR method for medial AP oblique projection of the knee? |
CR angle is the same as the AP knee criteria. CR is directed to midpoint of knee at a level half an inch distal to apex of patella |
|
|
What is demonstrated on a medial AP oblique projection of the knee? |
The proximal tibiofibular articulation is open with the lateral condyles of the femur and tibia seen in profile |
|
|
What is demonstrated on a lateral AP oblique projection of the knee? |
The proximal fibula superimposed by the proximal tibia, the medial condyles of the femur, and the tibia seen in profile |
|
|
How is the lateral projection of the knee positioned? |
Adjust rotation of body and leg until the knee is in a true lateral position with the femoral epicondyles directly superimposed and plane of patella perpendicular to plane of IR. Flex knee 20 to 30 degrees for lateral recumbent projection |
|
|
What is the CR method for a lateral projection of the knee? |
Angle CR 5-7 degrees cephalic for lateral recumbent projection. Direct CR to a point 1 inch distal to medial epicondyle |
|
|
What is shown in profile on a lateral projection of the knee? |
Distal femur, proximal tibia and fibula, and patella |
|
|
What is an AP weight-bearing bilateral knee projection taken to find? |
Possible cartilage degeneration or other knee joint pathologies. Bilateral knee is included on same exposure for comparison |
|
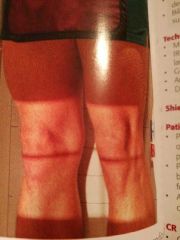
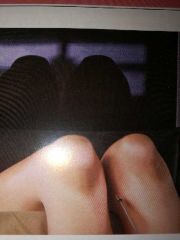
What projection is this? |
AP Weight Bearing Bilateral Knee |
|
|
How is an AP weight-bearing bilateral knee projection positioned? |
Patient stands erect on attached step or on step stool to place patient high enough for horizontal beam. Position feet straight ahead with weight evenly distributed on both feet and provide support handles for patient stability. |
|
|
What is the CR method for an AP weight-bearing bilateral knee projection? |
CR is perpendicular to IR on average sized patients, or 5 to 10 degrees caudad on a thin patient. Directed to midpoint between knee joints at a level 1/2 inch below apex of patella |
|

What method is this? |
Rosenberg method |
|
|
How is a Rosenberg method position? |
Patient stands erect, if needed stand on a step stool in order to be high enough for a 10° caudad angle. Position feet straight ahead with weight evenly distributed on both feet and knees flexed to 45°. Patella touches the upright bucky. |
|
|
What is the CR method for the Rosenberg method? |
CR is angled 10° caudad. Center directly to midpoint between knee joints at a level half an inch below apex of patella. |
|
|
What is the Rosenberg method? |
An PA axial weight-bearing bilateral knee projection |
|
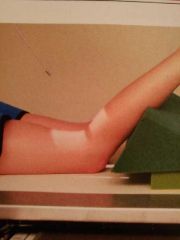
Which method is this? |
Camp Coventry method |
|
|
What are the camp Coventry, holmblad, and beclere methods used for in the knees? |
To demonstrate the intercondylar fossa, femoral condyle, tibial plateau, and intercondylar eminence. Evidence of bony or cartilaginous pathology, osteochondral defect, or narrowing of joint space |
|
|
What is the knee angulation for a camp Coventry method? |
40 to 50 degrees flexion |
|

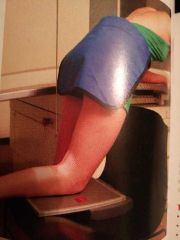
Which method is this? |
Holmblad method |
|
What is this method? |
Holmblad variation |
|

What is this method? |
Holmblad variation for wheelchair |
|
|
How is the camp Coventry method positioned? |
Patient lays prone on table. Knee is flexed 40 to 50 degrees. Support is placed under ankle |
|
|
How is the kneeling holmblad method position? |
Patient kneels on all fours, IR is placed under affected knee and center IR to popliteal crease. Patient leans forward slowly 20 to 30 degrees and holds the position, resulting in a 60 to 70 degree knee flexion |
|
|
What is the CR angulation for the camp Coventry and holmblad methods? |
CR is perpendicular to IR and lower leg |
|
What method is this? |
Beclere method |
|
|
What is the Beclere method done to find? |
Osteochondral defects, narrowing of the joint space, evidence of bony or cartilaginous pathology, & to demonstrate the intercondylar fossa, femoral condyle, tibial plateau, and intercondylar eminence |
|
|
When is the Beclere method done? |
When a patient cannot assume the prone position for a PA axial projection |
|
|
What is the IR size for the camp Coventry, holmblad, and Beclere methods? |
8 x 10, or 14 x 17 for bilateral studies |
|
|
How is the Beclere method position? |
Knees flexed 40 to 45 degrees, and position support under IR as needed to place IR firmly against posterior thigh and lower leg |
|
|
What is the CR method for a Beclere method? |
CR is perpendicular to lower leg or about 40 to 45 degrees cephalic. CR is directed to a point half an inch distal to Apex of patella |
|
|
What is the IR size for a projection of the patella? |
8 x 10 |
|
|
How is the PA projection of the patella positioned? |
A true PA position. Align interepicondylar line parallel to plane of IR, which usually requires about 5 degrees internal rotation of anterior knee. |
|
|
What is the CR method for a PA projection of the patella? |
CR is perpendicular to IR, directed to Mid patella area |
|
|
How is the lateral projection of the patella positioned? |
Adjust rotation of body and leg until knee is in a true lateral position. Flex knee only 5 to 10 degrees. |
|

What is this method? |
Merchant method |
|
|
What is the merchant bilateral method used to find? |
Subluxation of patella and other abnormalities of the patella and patellofemoral joint |
|
|
How is the merchant bilateral method positioned? |
Patient is in supine position with knees flexed 40 degrees over the edge of the table resting on a leg support. Patient must be comfortable and relaxed. Knees and feet are placed together and lower legs are secured to prevent rotation. IR is on edge against legs about 12in below the knees, perpendicular to x-ray beam |
|
|
What is the CR method for the merchant bilateral method? |
CR is angled 30° caudad from horizontal plane. Adjust if needed for true tangential projection of patella femoral joint spaces. CR directed to a point midway between patella |
|
|
What should be visualized on the merchant bilateral method? |
Intercondylar sulcus and patella of each distal femur should be visualized in profile with joint space open |
|
|
What is another name for the merchant bilateral method? |
Tangential- axial or Sunrise / Skyline projection |
|
What is this method? |
Inferosuperior projection of the patella |
|

What is this method? |
Hughston method |
|
|
How is the inferiosuperior projection of the patella positioned? |
Patient is in supine position with legs together, 40 to 45 degree knee flexion. IR is placed on edge resting on mid thighs, tilted to be perpendicular to CR |
|
|
What is the CR method for an inferiosuperior projection of the patella? |
CR is directed inferiosuperiorly at a 10 to 15 degree angle from lower leg to be tangential to patellofemoral joint |
|
|
How is the Hughston method positioned? |
Patient is in prone position with IR placed under knee. Slowly flex knee between 50 to 60 degrees from full extension of lower leg. Have patient hold foot with gauze or rest foot on supporting device |
|
|
What is the CR method for the Hughston method? |
CR is angled 45 degrees cephalad |
|
What method is this? |
Settegast method |
|
|
How is the Settegast method positioned? |
Patient is in prone position with ir under knee. Slowly flex knee to a minimum of 90 degrees. Have patient hold onto gauze or tape to maintain position |
|
|
What is the CR method for the Settegast method? |
CR tangential to patellofemoral joint space, which is 15 to 20 degrees from lower leg |
|
|
What is the major disadvantage of the Settegast method? |
The acute knee flexion tightens the quadriceps and draws the patella into the intercondylar sulcus, reducing the diagnostic value of the projection |
|

What is this method? |
Hobbs modification |
|
|
How is the Hobbes modification positioned? |
Patient seated in a chair with IR placed under knees resting on a step stool or support to help reduce OID. Knees should be flexed with feet placed slightly underneath the chair |
|
|
What is the CR method for the Hobbs modification? |
CR is perpendicular to IR, tangential to patellofemoral joint. CR is directed to mid patellofemoral joint. |
|
|
What is the minimum SID for a Hobbs modification? |
48 to 52 inches, to reduce magnification because of increased OID |
|
|
How do you know when you have a good AP oblique projection of the toes? |
Digits and question and distal half of metatarsals should be included without superimposition. Increased concavity on one side of shafts and by overlapping of soft tissues of digits. Heads of metatarsal should appear directly side by side with no overlapping |
|
|
How can you tell when you have a good AP projection of the toe? |
IP and MTP joint spaces are open |
|
|
How can you tell when you have a good lateral projection of the toe? |
Digits should be seen in lateral position free of superimposition. If separation of toes and possible, the distal Phalanx at least should be separated in the proximal Phalanx should be visualized through superimpose structures. Increased concavity on anterior surface of the distal Phalanx and posterior surface of the proximal phalanx |
|
|
How can you tell when you have a good tangential projection of the sesamoids? |
Sesamoids free of superimposition. A minimum of the first three distal metatarsal should be included in collimation. Open space between sesamoids and first metatarsal |
|
|
How can you tell when you have a good AP projection of the foot? |
Equal distance between 2nd through 5th metatarsal. Base of first and second metatarsals are separated, but base of 2nd to 5th metatarsal appear to overlap. Intertarsal joint space between first and second cuneiform should be demonstrated |
|
|
How can you tell when you have a good AP oblique projection of the foot? |
3rd through 5th metatarsals are free of superimposition. First and second metatarsals also should be free superimposition except for base area. Tuberosity at base of 5th metatarsal seen in profile. Joint spaces around cuboid and sinus tarsi are open and demonstrated |
|
|
How can you tell when you have a good lateral projection of the foot? |
Tibiotalar joint spaces open, distal fibula superimposed by the posterior tibia, distal metatarsals are superimposed. Entire foot demonstrated with a minimum of 1 inch of distal tib fib. Tuberosity of 5th metatarsal seen in profile |
|
|
How can you tell when you have a good AP weight-bearing projection of the foot? |
Open TMT joint space and visualization of joint between first and second cuneiforms. |
|
|
How can you tell when you have a good plantodorsal projection of the calcaneus? |
Open talocalcaneal joint space, no distortion of the calcaneal tuberosity, adequate elongation of the calcaneus |
|
|
How can you tell when you have a good lateral projection of the calcaneus? |
Superimposed Superior portions of the talus, open talocalcaneal joint, lateral malleolus superimposed over posterior half of the tibia and Talus. Tarsal sinus and calcaneocuboid joint space should appear open |
|
|
How can you tell when you have a good AP projection of the ankle? |
Medial mortise joint is open in the lateral mortise is closed. Some superimposition of the distal fibula by the distal tibia and Talus. Malleolo, talus, proximal half of metatarsals should be demonstrated |
|
|
How can you tell when you have a good AP mortise projection of the ankle? |
Entire ankle mortise joint should be open and well visualized |
|
|
How can you tell when you have a good AP oblique projection of the ankle with a 45 degree rotation? |
Mortise joint closed off. Lateral malleolus and Talus joint should show no or only slight superimposition, but medial malleolus and Talus or partially superimposed. Distal tibiofibular joint open |
|
|
How can you tell when you have a good lateral projection of the ankle? |
Tibiotalar joint open with uniform joint space. Distal fibula superimposed over posterior half of tibia. |
|
|
How can you tell when you have a good AP projection of the lower leg? |
Femoral and tibial condyles and profile with intercondylar Eminence centered within intercondylar fossa. Overlap of the fibula and tibia is visible at both proximal and distal ends |
|
|
How can you tell when you have a good lateral projection of the lower leg? |
Tibial tuberosity demonstrated in profile. Posterior borders of femoral condyles appear superimposed |
|
|
How can you tell when you have a good AP projection of the knee? |
Symmetric appearance of femoral and tibial condyles and the joint space. Medial half of the fibular head should be in super imposed by tibia. Intercondylar Eminence is seen in the center of intercondylar fossa |
|
|
How can you tell when you have a good AP oblique projection of the knee? |
Proximal tibiofibular articulation open with the lateral condyles of the femur and tibia seen in profile. Half of the patella should be seen free of superimposition by the femur. |
|
|
How can you tell when you have a good lateral projection of the knee? |
Distal femur, proximal tibia and fibula, and patella are shown in lateral profile. Patellofemoral and knee joints should be open. Adductor tubercle should not be visible on the medial condyle. Posterior borders of femoral condyles directly superimposed |
|
|
How can you tell when you have a good tunnel view of the intercondylar fossa? |
Intercondylar fossa should appear in profile, open without superimposition by the patella. Symmetric appearance of distal posterior femoral condyles in superimposition of approximately half of fibular head by tibia. Articular facets and intercondylar Eminence should be well visualized without superimposition |
|
|
How can you tell when you have a good tangential projection of the patella? |
Intercondylar sulcus and patella of each distal femur should be visualized and profile with patellofemoral joint space open. No rotation of knee is present, as evidenced by symmetric appearance of patella, anterior femoral condyles, and intercondylar sulcus |
|
|
Benign, neoplastic bone lesion caused by a consolidated overproduction of bone at a joint |
Exostosis |
|
|
A common term for osteomalacia is |
Rickets |
|
|
A fracture of the metatarsals |
March fracture |
|
|
A fracture of the distal tibia and fibula |
Potts fracture |
|
|
A fracture of the 5th metatarsal |
Jones fracture |
|
|
Abnormal separation or avulsion fracture between base of first and second metatarsals and cuneiforms |
Lisfranc joint injury |
|
|
An aseptic or ischemic necrosis. Lesions typically involve only one hip. Occurs predominantly in 5 to 10 year old boys, and a limp is usually the first clinical sign |
Legg-Calve Perthes disease |