![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
157 Cards in this Set
- Front
- Back
|
The bony thorax consists of the single (A) __ anteriorly, two (B) __, two (C) __, twelve pairs of (D)__ and twelve (E) __ posteriorly. |
A) Sternum B) Clavicles C) Scapulae D) Ribs E) Thoracic Vertebrae |
|
|
The two important bony landmarks of the thorax that are used for locating the CR on a PA or AP projection are the (A) __ and (B) __ respectively. |
A) Vertebra prominens B) Jugular notch |
|
|
What are the 4 divisions of the respiratory system? |
Pharynx, Bronchi, Trachea, Lungs |
|
|
What is the anatomical term for Adam's Apple? |
Thyroid Cartilage |
|
|
What is the anatomical term for Voice Box? |
Larynx |
|
|
What is the anatomical term for Breastbone? |
Sternum |
|
|
What is the anatomical term for Shoulder Blade? |
Scapulae |
|
|
What is the anatomical term for Collar Bone? |
Clavicle |
|
|
What are the 3 divisions of the structure located proximally to the larynx that serve as a common passageway for both food and air? |
Nasopharynx, Oropharynx, Laryngopharynx |
|
|
What is the name of the structure that acts as a lid over the larynx to prevent foreign objects such as food particles from entering the respiratory system? |
Epiglottis |
|
|
The trachea is located ___ to the esophagus. |
Anteriorly |
|
|
The __ bone is seen in the anterior portion of the neck and is found just below the tongue or floor of the mouth. |
Hyoid bone |
|
|
If a person accidently inhales a food particle, which bronchus is it most likely to enter, and why? |
The Right bronchus because it is larger and more verticle |
|
|
What is the name of the prominence, or ridge, seen when looking down into the bronchus where it divides into the right and left bronchi? Where is it located anatomically? |
Carina; approximately at the level of T5 |
|
|
What is the term for the small air sacs located at the distal end of the bronchioles, in which oxygen and carbon dioxide are exchanged in the blood? |
Alveoli |
|
|
The delicate, double -walled sac or membrane containing the lungs is called what? |
Pleurae |
|
|
The outer layer of this membrane adhering to the surface of the chest wall and diaphragm is known as what? |
partial pleurae |
|
|
The inner layer adhering to the surface of the lungs is __ or __. |
Pulmonary pleurae or Visceral pleurae |
|
|
The potential space between the partial, visceral, and pulmonary pleurae is |
Pleural Cavity |
|
|
Air or gas that enters the pleural cavity results in a condition know as |
pneumothorax |
|
|
What is the lower concave portion of the lung called? |
Base |
|
|
What is the central are in which bronchi and blood vessels enter the lungs? |
hilum |
|
|
What is name of the upper rounder portion of the lungs that is above the level of the clavicle? |
Apex |
|
|
What is the name of the extreme outermost layer of the lungs? |
Costophrenic Angle |
|
|
Why is the right lung smaller than the left lung and why is the right hemidiaphragm positioned higher that the left hemidiaphragm? |
B/c the liver is underneath the right lung |
|
|
What are the 4 important structures located in the mediastinum? |
Thymus gland, trachea, esophagus, heart, and great vessels |
|
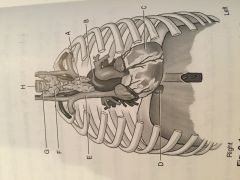
Identify the structures |
A) Thymus Gland B) Aortic Arch C) Heart D) Inf. Vena Cava E) Sup. Vena Cava F) Thyroid Gland G) Trachea H) Esophagus |
|
|
The heart is enclosed in a double walled membrane called the... |
Pericardium |
|
|
What are the 3 parts of the Aorta? |
Ascending, Decending, Arch of the Aorta |
|

Identify the structures |
A) Apex of the left lung B) Trachea C) Carina D) Heart E) Left costophrenic Angle F) Right Hemidiaphragm G) Hilum H) Apex of the lung I) Hilum J) Heart K) Bil Hemidiaphragm L) Bil Costophrenic |
|
|
What type of body habitus is associated with a broad and deep thorax? |
hyperthenic |
|
|
Which body habitus may cause the costophrenic angles to be cut off if careful vertical collimation is not used? |
Hypostenic and Asthenic |
|
|
What is the minimum number of ribs that should be demonstrated above the diaphragm on a PA radiograph an average adult chest with full inspiration? |
10 |
|
|
What objects should be removed or moved before a chest radiograph? |
Necklace, Bra, Religious medallion around neck, hair fasteners, oxygen lines |
|
|
True or False: Chest radiography is the most commonly repeated radiographic procedure b/c of poor positioning or exposure factor selection errors. |
True |
|
|
Chest radiography for the adult patient usually employs a kilovoltage peak of ___ to __ kV |
110 to 125 |
|
|
True or False: Generally, you do not need to use radiographic grids for adult patients for PA or lateral chest radiographs. |
False |
|
|
Optimal technical factor selection ensures proper penetration of |
Heart, Great Vessels, Lung regions, Hilar region |
|
|
Describe the way optimum density of the lungs and mediastinal structures can be determined on a PA chest radiograph. |
Outlines of the middle and upper vertebrae and ribs through the heart and other mediastinal structures. |
|
|
True or False: Because the heart is always located in the left thorax, the use of anatomic side markers on a PA chest projection may not be necessary. |
False |
|
|
Which device should used for the erect PA and Lateral chest projections for an infant? |
Pigg-O-Stat |
|
|
Which set of exposure factors is recommended for a chest exam of a young peds patient? |
70 to 85 kV, short exposure time |
|
|
True or False: Because they have a shallower (superior-inferior dimension) lung fields, the CR is often centered higher for geriatric patients. |
True |
|
|
To ensure better lung inspiration during chest radiography, exposure should be made during the __ inspiration. |
Full |
|
|
List the 4 possible pathologic conditions that suggest the need for both inspiration and expiration in PA chest radiographs. |
Pneumothorax, foreign body presence, fixation of diaphragm, distinguish opacity |
|
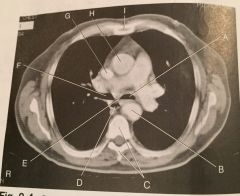
Identify the structures |
A) Left mainstem bronchus B) Descending Aorta C) T5 D) Esophagus E) Region of Carina F) Right mainstem bronchus G) Sup. Vena Cava H) Ascending Aorta I) Sternum |
|
|
List and explain briefly the 3 reasons chest radiographs should be taken with the patient in the erect position (when the patients condition permits). |
A) Diaphragm moves down B) Air and fluid levels in the lungs are better visualized C) Engorgement and hyperemia of pulmonary vessels can be prevented |
|
|
Why do the lungs tend to expand more with the patient in an erect position that in a supine position? |
Abdominal organs move downward allowing the diaphragm to move farther down and the lungs to fully aerate |
|
|
Explain the primary purpose and benefit of performing chest radiography using a 72-inch (183 cm) SID. |
Reduce distortion and magnification of the heart and other chest structures |
|
|
What is a common radiographic sign seen on a chest radiograph for a patient with respiratory distress syndrome? |
Air bronchogram |
|
|
What anatomic structures is examined to determine rotation on a PA chest radiograph? |
Symmetric appearance of sternoclavicular joints |
|
|
Which positioning tip will help prevent the patients chin and neck from being superimposed over the upper airway and apices of the lung for a PA chest radiograph? |
Extend the neck and chin upward |
|
|
Which lateral projection would you perform for a patient with severe pains in the left side of chest? |
Left |
|
|
Which lateral projection would you perform for a patient with no chest pain but recent hx of pneumonia in right lung? |
Right |
|
|
Which lateral projection would you perform for a patient with no chest pain or hx of heart trouble? |
Left |
|
|
Why is it important to raise the patient's arms above the head for a lateral chest projection? |
Prevents superimposition on the upper chest field |
|
|
The traditional CR centering technique for the chest is to place the top of the IR how many inches above the shoulder? |
1.5 to 2 inches or 4 to 5cm |
|
|
A recommended CR centering technique for a PA chest projection requires the technologist to palpate (A)___ and measure down from the bony landmark (B) ___ inches for a male and (C) ___ for a female. |
A) T1 B) 7 inches or 18 cm C) 8 inches or 20 cm |
|
|
Should the 14 X 17 inch IR be aligned lengthwise or crosswise positions for a PA projection of a hypersthenic patient? |
Crosswise |
|
|
Should the 14 X 17 inch IR be aligned lengthwise or crosswise positions for a PA projection of a hyposthenic patient?
|
Lengthwise |
|
|
What bony landmark is palpated for centering of the AP chest projection? |
Jugular Notch |
|
|
True or False: With most digital test units, the question of IR placement into either vertical or crosswise positions is eliminated b/c of the larger IR. |
True |
|
|
True or False: In general, for an average patient more collimation should be visible on the lower margin of the chest image that on the top for a PA or lateral chest projection. |
False; it should be equal |
|
|
True or False: For most patients, the CR level for a PA chest projection is near the inferior angle of the scapula. |
True |
|
|
True or False: The height or vertical dimension of the average-to-large person's chest is greater that the width, or horizontal dimensions. |
False; greater width |
|
|
True or False: Single-photon emission computed tomography (SPECT) is frequently used to diagnose Myocardial Infarction (MI). |
True |
|
|
True or False: Ultrasound is not an effective modality to detect pleural effusion. |
False; it is effective |
|
|
True or False: Echocardiography and electrocardiography are basically the same procedure. |
True |
|
|
What is Cystic Fibrosis? |
One of the most common inherited diseases |
|
|
What is Pulmonary Edema? |
Condition most frequently associated with CHF |
|
|
What is Dyspnea? |
Shortness of breath |
|
|
What is Pneumothorax? |
Accumulation of air in the pleural cavity |
|
|
What is Empyema? |
Accumulation of pus in the pleural cavity |
|
|
What is Silicosis? |
A form of occupational lung disease |
|
|
What is tuberculosis? |
A contagious disease caused by an airborne bacterium |
|
|
What is Bronchiectasis? |
Irreversible dilation of the bronchioles |
|
|
What is COPD? |
Most common for of Emphysema |
|
|
What is Bronchitis? |
Acute or Chronic irritation of bronchi |
|
|
What is Atelectasis? |
Collapse of all or portion of the lung |
|
|
What is Pleurisy? |
Inflammation of pleura |
|
|
For left lung atelectasis should exposure factors be increased, decreased, or remain the same? |
Increased |
|
|
For lung neoplasm should exposure factors be increased, decreased, or remain the same?
|
Remain the same |
|
|
For severe pulmonary edema should exposure factors be increased, decreased, or remain the same?
|
Increased |
|
|
For respiratory distress syndrome should exposure factors be increased, decreased, or remain the same?
|
Increased |
|
|
For secondary tuberculosis should exposure factors be increased, decreased, or remain the same?
|
Increased or remain the same |
|
|
For advanced emphysema should exposure factors be increased, decreased, or remain the same?
|
Decreased |
|
|
For large pneumothorax should exposure factors be increased, decreased, or remain the same?
|
remain the same |
|
|
For pulmonary emboli should exposure factors be increased, decreased, or remain the same? |
Remain the same |
|
|
For primary tuberculosis should exposure factors be increased, decreased, or remain the same? |
Remain the same |
|
|
For advanced asbestosis should exposure factors be increased, decreased, or remain the same? |
Remain the same |
|
|
What is a form of occupational lung disease? |
Anthracosis, Silicosis, Asbestosis |
|
|
What chest projection is recommended to detect calcification or cavitations with in the upper lung region near the clavicles? |
AP lordotic |
|
|
Why is a PA chest preferred over an AP projection? |
The heart is closer to the IR to reduce magnification |
|
|
The CR is placed at the level of ___ vertebra for a PA chest projection. |
T7 |
|
|
The shoulders need to be rolled forward for the PA projection to allow ___ to move laterally and be clear of the lung fields. |
Scapulae |
|
|
Why should a left lateral be performed unless departmental protocol indicates otherwise? |
It shows the heart better |
|
|
How much seperation of the posterior ribs on a lateral chest projection indicates excessive rotation from a true lateral position? |
> 1cm or .5"-.75" |
|
|
To prevent the clavicles from obscuring the apices on an AP projection of the chest, the CR should be angled (A) ___ so that it is perpendicular to the (B)___. |
A) + or - 5 degrees B) Sternum |
|
|
What is the name of the condition characterized by fluid entering the pleural cavity? |
Pleural Effusion |
|
|
Which specific position would be used if a patient were unable to stand but the physician suspects the patient to have fluid on the left lung? |
Left Lateral Decubitus |
|
|
What is the name of the condition characterized by free air entering the pleural cavity? |
Pneumothorax |
|
|
Which specific position would be used if the patient were unable to stand but the physician suspects the patient to have free air in the left pleural cavity? |
Right Lateral Decubitus |
|
|
What circumstances or clinical indications suggests that an AP lordotic projection should be ordered? |
To r/o calcifications and masses beneath the clavicle |
|
|
What positions/projections would be used for a patient who is to ill or weak to stand for an AP lordotic projection? |
AP semiaxial projection with the patient supine |
|
|
Which anterior oblique projection would best demonstrate the left lung? |
Right Anterior Oblique (RAO) |
|
|
Which posterior oblique projection would best demonstrate the left lung? |
Left posterior oblique (LPO) |
|
|
For certain studies of the heart, the ___ anterior oblique requires a rotation of ___ degrees. |
A) Left B) 60 |
|
|
True or False: A grid is not recommended for a Left Posterior Oblique (LPO). |
Flase |
|
|
Where is the CR placed for a lateral projection of the upper airway? |
Level of C6 or C7 midway between the layrngeal prominence of the thyroid cartilage and jugular notch |
|
|
Careful collimation during a chest radiograph will improve image quality by decreasing ___ radiation to the IR. |
Scatter |
|
|
What are the recommended patient instructions when performing an erect PA chest on a female patient with large breasts? |
Lift the breasts up and outward and the removed hands as she leans against the bucky |
|
|
True or False: No lead shielding is necessary for male patients or women greater than age 65 during radiographic imaging of the chest. |
False; shielding is always necessary reguardless of age |
|
|
An erect chest PA radiograph aids the patient to achieve full inspiration and helps prevent ___ and ___ of the pulmonary vessels. |
Engorgment and Hypermia |
|
|
A radiograph of a PA view of the chest reveals sternoclavicular (SC) joints are not the same distance from the spine. The right SC joint is closer to the midline than is the Left SC joint. What is the positioning error? |
Rotation. The patient is rotated into a slight Right Anterior Oblique position. |
|
|
A radiograph of a PA projection of the chest shows only 7 posterior ribs above the diaphragm. What caused this problem, and how can it be fixed on the repeat exposure? |
The lungs are underinflated. Make sure the patient takes a deep breath and take the xray on the 2nd inhalation. |
|
|
A radiograph of a PA and left lateral projection of the chest reveals the mediastinum is underpenetrated. The technologist used the following factors for the image: 72" SID, upright bucky, full inspiration exposure, 75kV, and 600-mA and a 1/60 second exposure time. Which factor is the cause of the problem and how can it be improved? |
The kV should be between 110-125kV. Increase the kV and decrease the mA. |
|
|
A radiograph of a PA chest projection of the chest reveals the top of the apices are cut off and a wide collimation border can be seen below the diaphragm. In what way can this be corrected? |
Center the CR to T7, make sure the IR is centered to the CR and the top collimation boarder is at the vertebral prominence. |
|
|
A patient with a clinical history of advanced emphysema comes to the radiology dept for a chest xray. Automatic Exposure Control (AEC) will not be used. How the should radiographer manually alter the exposure setting for the patient? |
Decrease the kV moderatly |
|
|
A patient with severe pleural effusion comes to the radiology dept for a chest xray. Automatic Exposure Control (AEC) will not be used. How the should radiographer manually alter the exposure setting for the patient?
|
Increase the kV slightly |
|
|
A patient comes to the radiography dept for a presurgical chest exam. The clinical history indicates a possible situs inversus of the thorax. Which positioning step or action must be taken to perform a successful chest exam? |
Ensure the correct placement of markers on the IR b/c the heart and other structures maybe transposed from left to right |
|
|
A radiograph of a lateral projection of the chest reveals the posterior ribs and costophrenic angles are sperated more that 1/2 in or 1cm, indicating excessive rotation. Describe a possible method for determining the direction of rotation. |
Determine which hemidiaphragm is more posterior or anterior the left hemidiaphragm can frequently be identified by visualization of air bubbles or the inferior hear shadow |
|
|
A patient enters the ER with a possible foreign hemothorax in the right lung caused by a MVA. The patient is unable to stand or sit erect. Which specific position would best demonstrate this condition? |
Right Lateral Decubitus position |
|
|
A young child enters the ER with a possible foreign body in on of the bronchi of the lung. The foreign body, a peanut, cant be seen on the PA and lateral projections. Which additional projections could the technologist perform to locate the foreign body? |
AP and Lateral upper airway projection |
|
|
A routine chest series indicates a possible mass beneath the a patients right clavicle. The PA and Lateral projections are inconclusive. What additional projections could be take to rule out this condition? |
AP Lordotic |
|
|
A patient has a possible small pneumothorax. Routine chest projection (PA and LAteral) fail to reveal the pneumothorax conclusively. Which additional projections could be take to rule out this condition? |
Lateral Decubitus AP with affected side up and/ or inspiration and expiration PA projections |
|
|
A patient with a history of pleurisy comes to the radiology dept. What radiographic series should be performed? |
Erect PA and Lateral |
|
|
A patient with a possible neoplasm in the right lung apex comes to the radiology dept. for a chest exam. The PA and Lateral projections dont clearly demonstrate the neoplasm b/c of superimposition of the clavicle over the apex. The patient is unable to stand or sit erect. Which additional projections can be taken? |
AP semiaxial projection; CR is angled 15- 20 degrees cephalad to project the clavicles above the apices and clearly demonstrate the possible tumor. |
|
|
PA and left lateral projections demonstrate a suspicious region in the left lung. The radiologist orders an oblique projection that will best demonstrate or "elongate" the left lung. Which specific oblique projections will best elongate the left lung? |
Left Posterior Oblique or Right Anterior Oblique |
|
|
Aspiration |
Occurs when foreign objects are swallowed or aspirated into the air passage of the bronchial tree. |
|
|
Atelectasis |
A condition in which collapse of all or a portion of a lung occurs as the result of obstruction of the bronchus or puncture or "blowout" of an air passageway. |
|
|
Brochiectasis |
An irreversible dilation or widening of bronchi or bronchioles that may result from repeated pulmonary infection or obstruction. |
|
|
Bronchitis |
an acute or chronic condition in which excessive mucus is secreted into the bronchi causing and SOB |
|
|
Chronic Obstructive Pulmonary Disease (COPD) |
A form of persistent obstruction of the airway that usually causes difficulty in emptying the lungs of air; maybe caused by emphysema or chronic bronchitis |
|
|
Cystic Fibrosis |
The most common of inherited diseases, is a condition in which secretions of heavy mucus cause progressive clogging of bronchi and bronchioles. |
|
|
Dyspnea |
Difficulty in breathing |
|
|
Emphysema |
An irreversible and chronic lung disease in which air spaces in the alveoli become greatly enlarged as a result of alveolar wall destruction and loss of alveolar elasticity. |
|
|
Epiglottitis |
Swelling of the epiglottis |
|
|
Neoplasm |
New growth or tumor |
|
|
Benign |
Non Cancerous |
|
|
Malignant |
Cancerous |
|
|
Pleural Effusion |
A condition of abnormal accumulation of fluid in the pleural cavity |
|
|
Empyema |
Pus in the lungs |
|
|
Hemothorax |
blood in the lungs |
|
|
Pleurisy |
inflammation of the pleura surrounding the lungs |
|
|
Pneumonia |
An inflammation caused by a virus resulting in accumulation of fluid within certain sections of the lungs |
|
|
Aspiration pneumonia |
Caused by aspiration of a foreign object into the lungs, which irritates the bronchi, resulting in edema |
|
|
Bronchopneumonia |
Bronchitis of both lungs that caused by strep or staph bacteria. |
|
|
Lobar Pneumonia |
Pneumonia generally confined to one or two lobes of the lungs |
|
|
Viral (Interstitial) Pneumonia |
causes inflammation of the alveoli and connecting lung structures. |
|
|
Pneumothorax |
an accumulation of air in the pleural space that causes partial or complete collapse of the lung and results in immediate and severe SOB and chest pain |
|
|
Pulmonary Edema |
Excess fluid within the lung that most frequently is caused by a back up in pulmonary circulation commonly associated with CHF |
|
|
Respiratory Distress Syndrome (RDS) |
An emergent condition in which the alveoli and capillaries of the lungs are injure or infected resulting in leakage of fluid and blood into the spaces between the alveoli |
|
|
Tuberculosis (TB) |
A contagious disease that is caused by airborne bacteria. |
|
|
Anthracosis |
Caused by deposits of coal dust |
|
|
Asbestosis |
caused by inhalation of asbestos dust that results in pulmonary fibrosis |
|
|
Silicosis |
A permanent condition of the lung that is caused by inhalation of silica dust. |
|
|
Sarcoidosis |
Fibrous Scaring |