![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
20 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
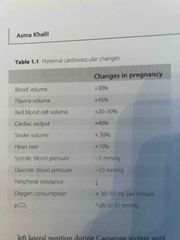
Cardiovascular changes |
1) Increased plasma volume but no further increase after 32 weeks
2) Increased red cell mass until term but decreased haematocrit and Hb
3) Increased cardiac output by 40%. Starts early in pregnancy and plateaus at 24-30weeks. Returns to prepreg levels after delivery
4) increased stroke volume early in pregnancy 5) Heart rate increases by 10% late in pregnancy 6) from 8 to 36 weeks systolic and diastolic BP drop between 5-10mmHg due to a decrease in peripheral resistance 7) ECG changes - increase HR, LAD 15 degrees, inverted T wave in lead 3, Q in lead 3 and AVF, non-specific ST changes |
|
|
|
ECG changes |
ECG changes - increase HR (10-15%) - LAD 15 degrees - inverted T wave in lead 3 - Q in lead 3 and AVF - non-specific ST changes
These are due to: - Left ventricular hypertrophy and dilation - No change in the contractility - Upward displacement of the diaphragm - Apex shifted anterior and to the left |
|
|
|
Respiratory changes |
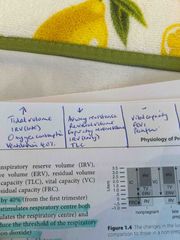
1) Ventilation increases by 40% from first trimester 2) Progesterone stimulates respiratory centre and is a bronchodilator 3) Decrease airway resistance 4) Increased tidal volume (not respiratory rate) 5) No change in the vital capacity or FEV1 or peak flow rate 6) Decreased Residual volume 7) Decreased expiratory reserve volume 8) IRV decreased in early but increased in late pregnancy 9) Decreased total lung capacity 10) Increased oxygen consumption |
|
|
|
Respiratory changes summary |
Back (Definition) |
|
|
|
ABG in pregnancy |
PCO2 falls to 31mmHg PaO2 increases to 14kPa during third trimester and then falls to <13.5 at term - increased CO and O2 consumption Decreased HCO3 Decreased sodium Na Decreased osmolarity by 10mmol/l |
|
|
|
Urinary system |
1) Kidney increases in size by 1cm length 2) Ureters dilated as progesterone is a smooth muscle relaxant 3) Increased renal blood flow from first trimester 4) Increased GFR 5) Decreased: urea, creatinine, urate and HCO3 6) Mild glycosuria and proteinuria 7) Decreased plasma osmolarity |
|
|
|
Gastrointestinal tract changes |
1) Gastric relaxation 2) Delayed gastric emptying 3) Relaxation of the gastro-oesophageal sphincter 4) Reflux 5) Constipation |
|
|
|
Liver changes |
1) ALP produced by placenta increases 3x normal level 2) Reduced Cholecystokinin release 3) Reduced gallbladder contractility = more likely to have gallstones |
|
|
|
Haematological system |
1) Increased erythropoeisis from early pregnancy due to increased erythropoietin and placental lactogen 2) Physiological anaemia - due to increased plasma volume > red cell volume 3) Increased WBC and peaks after delivery. Primarily neutrophils 4) Increased iron demand and increased iron absorption (erythroid hyperplasia) in second half of pregnancy. Iron deficiency anaemia 5) Haemostasis in pregnancy 6) Increase in all coagulation factors except XI (9) and XIII (13) from the first trimester 7) Increased ESR - erythrocyte sedimentation rate (double non pregnant) 8) Increased platelet production but decreased count (dilution) 9) Fibrinolysis is low in labour but returns to normal within 1 hour of delivery of the placenta. |
|
|
|
Physiology of lactation |
Prolactin - polypeptide hormone Increase in prolactin and human placental lactogen (HPL) Early pregnancy- hyperplasia of the alveolar cells and lactiferous ducts Late pregnancy- alveolar cell hypertrophy and initiation of secretion Milk is made when progesterone and oestrogen levels fall rapidly after delivery Milk production averages 500-1000ml per day In women who do not suckle, milk production gradually falls and may persist for 3-4 weeks postpartum. Mothers who are breastfeeding twins produce twice as much milk |
|
|
|
Suckling stimulus |
Back (Definition) |
|
|
|
Milk |
Suppression - dopamine antagonists = bromocriptine and cabergoline Stimulate milk production- metoclopramide (dopamine antagonist) |
Thyrotropin-releasing hormone may also play a role in stimulating prolactin production After 6 weeks postpartum prolactin levels decline but slower if suckling continues |
|
|
Breastfeeding amenorrhorea |
High prolactin levels during breastfeeding tend to suppress ovulation and therefore cause amenorrhoea.
10% of exclusively breastfeeding mothers fall pregnant if they don’t use any contraception.
If a woman conceives during lactation rising progesterone and oestrogen will suppress milk production |
|
|
|
Postpartum lochia decreases over 3-6 weeks |
Turning from: Red - lochia rubra To Pink - lochia serosa To Yellowish-white - lochia alba |
|
|
|
Third stage of labour |
From delivery of baby until delivery of placenta and membranes Prostaglandin F2a |
|
|
|
Progesterone |
1) Stimulates respiratory centre both directly (stimulates respiratory centre) and indirectly (reduces the threshold of the respiratory centre to carbon dioxide.
2) progesterone is a bronchodilator 3) Progesterone is a smooth muscle relaxant 4) suppresses formation of myometrial gap junctions and the effect of IL-8 which causes cervical ripening 5) Progesterone also decreases uterine sensitivity to oxytocin 6) Antiprogesterones like mifepristone cause cervical ripening and increase myometrial contractility |
|
|
|
Physiology of labour |

Back (Definition) |
|
|
|
Insulin resistance |
Increases during pregnancy But in the first trimester there is increased insulin sensitivity followed by increased insulin resistance as the pregnancy continues |
|
|
|
Thyroid in pregnancy |
Increased thyroid size and increased production of thyroid hormones. Increase in overall activity of the thyroid gland due to high levels of HC
Increase in thyroid binding globulin due to higher oestrogen levels which leads to higher levels of thyroid hormones |
|
|
|
Cholesterol during pregnancy |
Increases significantly in maternal plasma to support fetal development including the formation of steroid hormones and cell membrane |
|