Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
54 Cards in this Set
- Front
- Back
|
LAD refers to __________.
|
enlarged lymph nodes
|
|
|
Painful LAD is seen with _______________.
|
acute infection
|
|
|
Painless LAD is seen with ______________.
|
chronic inflammation, metastatic carcinoma, lymphoma
|
|
|
What region of the lymph node would expand in rheumatoid arthritis?
|
Follicles
|
|
|
What region of the lymph node would expand in early HIV?
|
In HIV we see generalized lymphadenopathy and the region is the follicles (HIV infects CD4+ cells, however, cells of the follicle, the follicular dendritic cells are also CD4+)
|
|
|
What region of the lymph node would expand in viral infections?
|
Paracortex
|
|
|
What region of the lymph node would expand in sinus histiocytosis?
|
This is classically seen in lymph nodes draining tissue with cancer (reactive).
|
|
|
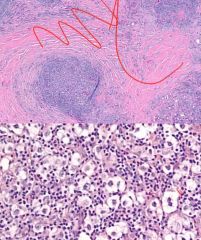
Histiocytes live deep in the ________ of lymph nodes.
|
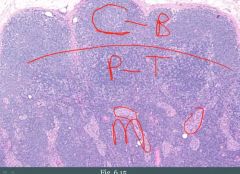
medulla
Sinus histiocytes would be present in the encircled areas. |
|
|
Lymphoma is what?
|
Neoplastic proliferation of lymphoid cells that form a mass.
|
|
|
Where do lymphomas arise?
|
May arise in lymph nodes, but may arise in extranodal tissues
|
|
|
Lymphomas are divided into [...]
|
NHL (60%)
HL (40%) |
|
|
What cell type make up the vast majority of NHLs?
|
B-cell type
|
|
|
What key lymphomas arise from small cell neoplastic B-cells?
|

Small cells indicate more mature cells. More mature cells would tend to make structures similar to normal tissue.
Follicle, Mantle, Margin |
|
|
Follicular lymphoma what?
|
Neoplastic proliferation of small B cells (CD20+) that make follicle-like nodules.
|
|
|
Follicular lymphoma presents as [...]
|
Clinically presents in late adulthood with painless LAD
|
|

What could this be?
|
Follicular lymphoma.
|
|
|
Follicular lymphoma is driven by what?
|
A translocation: t(14;18).
BCL2 (18) translocates to the immunoglobulin heavy chain locus (14) |
|
|
Immunoglobulin heavy chain is located on chromosome ____.
|
14
|
|
|
Follicular lymphoma is due to _______________ (overproliferation/absence of apoptosis).
|
absence of apoptosis
|
|
|
Patients with follicular lymphoma are relatively ___________.
|
asymptomatic
|
|
|
Treatment in follicular lymphoma?
|
Treatment is reserved for those who are symptomatic.
Low-dose chemotherapy (CTX) or rituximab (anti-CD20). |
|
|
Complication of follicular lymphoma?
|
(1) Can progress to diffuse large B-cell lymphoma which presents as an enlarging lymph node.
|
|
|
How do you distinguish follicular hyperplasia from follicular lymphoma?
|
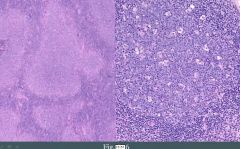
(1) In follicular lymphoma, architecture is disrupted.
(2) Lack of tingible body macrophages in germinal centers. - Normally in response to infection, B-cells undergo hypermutation and many of them die by apoptosis, only to be eaten by macrophages. (3) Expression of Bcl2 in follicles (4) Monoclonality |
|
|
What is mantle cell lymphoma?
|
Neoplastic small B cells (CD20+) that expand the mantle zone.
|
|
|
How does mantle cell lymphoma present?
|
Clinically presents in late adulthood with painless LAD.
|
|
|
Mantle cell lymphoma is driven by what?
|
t(11;14)
Cyclin D1 on 11 is translocated to IgH locus on 14. Overexpression of cyclin D1 promotes progression through G1/S checkpoint. |
|
|
What is a marginal cell lymphoma?
|
Neoplastic small B-cells (CD20+) that expand marginal zone.
|
|
|
This type of lymphoma is associated with chronic inflammatory states.
|
Marginal cell lymphoma
|
|
|
What chronic inflammatory states may lead to marginal zone lymphoma?
|
Marginal zone is formed by post-germinal center B-cells (they enter, get activated, that's when margins are produced).
Hashimoto's thyroiditis Sjogren syndrome H. pylori gastritis |
|
|
What is a MALToma? Where is it classically seen?
|
Marginal zone lymphoma of mucosal sites (e.g., stomach). Seen with chronic H. pylori gastritis.
|
|
|
This lymphoma may regress if the inciting agent is removed.
|
Gastric MALToma (if H.pylori is eradicated)
|
|
|
What is Burkitts lymphoma?
|
Neoplastic proliferation of intermediate-sized B-cells (CD20+). It is associated with EBV.
|
|
|
Burkitt's lymphoma classically presents as?
|
Extranodal mass in a child or young adult.
|
|
|
What forms of Burkitt's lymphoma is there?
|

(1) African form that usually involves the jaw
(2) Sporadic form that usually involves the abdomen |
|
|
Burkitt's lymphoma is driven by what?
|
Translocations of c-myc. t(8;14) is the most common.
|
|
|
What would you see on histology of Burkitt's lymphoma?
|
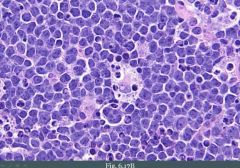
High c-myc drives a very high proliferation of cells.
We see high mitotic rate and starry sky appearance. Tumor cells are blue (the sky). They are turning over so quickly that they are dying. Tingible body macrophages eating them forms the star. |
|
|
What is DLBCL?
|
Diffuse Large B-Cell Lymphoma
Neoplastic large B-cells (CD20+) that grow diffusely in sheets. |
|
|
What is the MC form of NHL?
|
DLBCL
|
|
|
DLBCL is clinically _____________ (indolent/aggressive).
|
aggressive. It doesn't look like anything.
|
|
|
DLBCL can arise how?
|
Sporadically or from transformation of follicular lymphoma.
|
|
|
DLBCL presents how?
|
Presents in late adulthood as an enlarging LN or extranodal mass.
|
|
|
In Hodkin's lymphoma you don't have a big mass of malignant cells, instead you have?
|
Rare neoplastic cells called Reed sternberg cells that produce cytokines that draw in other inflammatory cells, which then results in the production of a mass.
|
|
|
Key hallmark of Hodkin's lymphoma. What are its markers?
|
Reed-Sternberg cell. CD15+, CD30+.
|
|
|
Describe the Reed-sternberg cell.
|
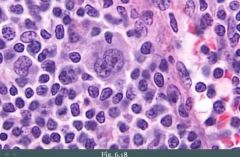
Large B cell with multilobed nuclei and prominent nucleoli.
|
|
|
What is the result of reed sternberg cells that secrete cytokines?
|
(1) Occasionally results in 'B' symptoms (which are fevers, chills, night sweats)
(2) Attract reactive lymphocytes, plasma cells, macrophages, and eosinophils (3) May lead to fibrosis |
|
|
What forms the basis of classification of Hodkin's lymphoma?
|
Reactive inflammatory cells that are present
|
|
|
The MC form of Hodkin lymphoma is?
|
Nodular sclerosis subtype (70%)
|
|
|
What subtypes of Hodkin's lymphoma are there?
|
(1) Nodular sclerosis
(2) Lymphocyte-rich (3) Mixed cellularity (4) Lymphocyte-depleted |
|
|
Describe the classical presentation of nodular sclerosing subtype of Hodkin's lymphoma.
|
Classic presentation is enlarging cervical neck or mediastinal lymph node in a young adult, usually female.
|
|
|
A biopsy is performed in a female young adult with Hodkin's lymphoma. What do you see?
|
Lymph node divided by bands of fibrosis. RS cells are present in lake-like spaces (lacunar cells)
|
|
|
What important consideration is there regarding lymphocyte-rich variant of Hodkin's lymphoma?
|
Best prognosis
|
|
|
What important consideration is there regarding mixed cellularity variant of Hodkin's lymphoma?
|
Abundant eosinophils (IL-5)
|
|
|
What important consideration is there regarding lymphocyte-depleted variant of Hodkin's lymphoma?
|
Worst prognosis.
|
|
|
The lymphocyte-depleted variant of Hodkin's lymphoma is seen in ________ and _________.
|
elderly; HIV+ individuals
|