|
|
92. The LEAST effective method of protecting the spinal cord during surgery on the descending thoracic aorta is
A. reducing the duration of ischaemia
B. lowering the CSF (cerebrospinal fluid) pressure
C. spinal cord hypothermia
D. administration of a thiobarbiturate
E. use of shunts to bypass the aortic cross-clamp
|
D
thiopentone will decrease the metabolic activity of the spinal cord, but this is probably the least effective
|
|
|
. The LEAST correct statement regarding anterior spinal artery syndrome is that
A. most patients are elderly
B. the onset is sudden
C. there are no systemic symptoms
D. the myelogram and CAT scan are abnormal
E. sensory involvement is minor or patchy
|
D
Neurologic Complications of Spinal and Epidural Anesthesia - Regional Anesthesia & Pain Medicine 2000, table 3
• Usually elderly
• sudden onset
• no generalized, systemic symptoms
• Myelogram and CT normal
• Minor or patch sensory involvement
|
|
|
90. The most commonly reported cause of awareness during general anaesthesia for a non-obstetric procedure is
A. inadequate intra-operative opiate analgesia
B. equipment failure
C. the use of total intravenous anaesthesia
D. faulty anaesthetic technique
E. use of a laryngeal mask airway
|
D
CEACCP 2005: “Awareness is frequently associated with poor
anaesthetic technique”
|
|
|
89. In patients with mitral regurgitation
A. left ventricular damage does NOT occur before the onset of symptoms
B. mitral valve replacement has a lower operative mortality and incidence of late adverse outcomes compared to mitral valve repair
C. an ejection fraction of less than 60% may be an indication for surgery, even in the absence of symptoms
D. long term vasodilators have been shown to delay the need for surgery
E. the presence of a third heart sound always indicates heart failure
|
C
Stoelting:
• Development of ventricular hypertrophy and increased compliance of the left atrium permit the accommodation of the regurgitant volume without a major increase in left atrial pressure. This allows patients to maintain cardiac output and remain free of pulmonary congestion and be asymptomatic for many years
• Mitral valve repair is preferred to mitral valve replacement because it restores valve competence, maintains the functional aspects of the mitral valve apparatus, and avoids insertion of a prosthesis. The mitral valve apparatus is very important in sustaining left ventricular function. The absence of the subvalvular apparatus causes distortion of the left ventricular contractile geometry and impairment of left ventricular ejection
• Survival may be prolonged if surgery is performed before the ejection fraction is less than 60% or before the left ventricle is unable to contract to an end-systolic dimension of 45 mm (normal < 40 mm).
• Although vasodilators are useful in the medical management of acute mitral regurgitation, there is no apparent benefit to long-term use of these drugs in asymptomatic patients with chronic mitral regurgitation
• S3 can be heard and recorded in healthy young adults. However, it is usually abnormal in patients over the age of 40 years, suggesting an enlarged ventricular chamber (uptodate)
|
|
|
88. With respect to acute myocardial infarction
A. true posterior infarcts manifest on the ECG as a tall R wave in Lead V3
B. aspirin should NOT be given unless myocardial infarction is confirmed
C. regional anaesthesia is NOT recommended if thrombolytic therapy has been used within the previous 2 weeks
D. Angiotensin Converting Enzyme (ACE) inhibitors may be indicated in the acute period
E. Troponin I testing is unsuitable in the peri-operative period
|
|
|
|
87. The standard error of the mean is
A. dependent for its validity on a normal distribution in the population
B. an indication of the likelihood of making a type II error
C. about 2, if the standard deviation is 15 and the sample size 50
D. NOT necessary for calculating the confidence interval for the mean
E. the variance of the population of sample means
|
C
• The population does not have to be normally distributed because of central limit theorem: the shape of a a sampling distribution will approximate a normal distribution when the number of samples is high, even when the underlying population is not a normal distribution
• "Standard error is also known as the standard error of the mean. If one takes a number of samples from a population, we will have a mean for each sample. The SD of the sample means is the standard error" Myles and Gin
• "type II error occurs when one accepts the H0 incorrectly and the probability of this occurring is termed beta" Myles and Gin
• SE = SD / square root of sample size. So SE = 15/7
• "standard error is used to calculate confidence intervals, and so is a measure of precision"
• No, it is the standard deviation no variance of population means
|
|
|
86. The laryngeal mask when correctly inserted
A. may be safely used in a patient with latex allergy
B. lies with the sides facing the pyriform fossa
C. lies with the upper border under the base of the tongue
D. forms a seal around the laryngeal perimeter
E. has the black line on the tube, always facing the lower lip of the patient
|
A
Thouhg B,C & D also seem mostly correct
Product information:
Latex free
"When fully inserted using the recommended insertion technique, the distal tip of the LMA™ airway cuff reaches the distal end of the hypopharynx immediately above the oesophageal sphincter. Its sides face into the pyriform fossae and the upper border rests against the base of the tongue"
lies with the upper border under the base of the tongue - almost true See above
"In addition the LMA™ airway is contraindicated in patients with fixed decreased pulmonary compliance (e.g. patients with pulmonary fibrosis) because the LMA™ airway forms a lowpressure seal (approximately 20cm H2O) around the larynx."
"The mask aperture must face posteriorly (Figure 8) and the black line on the airway tube should be oriented anteriorly toward the upper lip."
|
|
|
85. Intra-operative hypoglycaemia in children is LEAST likely in
A. small-for-age children
B. Beckwith-Wiedeman Syndrome
C. infants following an overnight fast
D. infants on propranolol peri-operatively
E. intra-operative interruption of pre-operative total parenteral nutrition (TPN)
|
C
Five common features of BWS
• Macroglossia
• macrosomia (birth weight and length greater than the 90th percentile
• Midline abdominal wall defects (omphalocele/exomphalos, umbilical hernia, diastasis recti)
• Ear creases or ear pits
• Neonatal hypoglycemia
|
|
|
84. Transdermal fentanyl patches are used in the treatment of cancer pain. Once the patch is applied, blood concentrations peak at an average of
A. 1 hour
B. 2 hours
C. 4 hours
D. 12 hours
E. 24 hours
|
|
|
|
83. In a trial, 75 patients with an uncommon, newly described complication and 50 matched patients without this complication are selected for comparison of their exposure to a new drug. The results show
Complication present Complication absent
Exposed to new drug 50 25
Not exposed 25 25
From these data
A. the relative risk of this complication with drug exposure CANNOT be determined
B. the odds ratio of this complication with drug exposure CANNOT be determined
C. the relative risk of this complication with drug exposure is 2
D. the odds ratio of this complication with drug exposure is 1.33 (recurring)
E. none of the above
|
A
"Because accurate information concerning all patients at risk in a retrospective case-control study is not available (because sample size is set by the researcher), incidence rate and risk cannot be accurately determined, and the odds ratio is used as the estimate of the risk ratio" (Myles and gin p.74)”
|
|
|
82. Assuming correct positioning, complications of an intra-aortic balloon pump may include all of the following EXCEPT
A. systemic infection
B. peripheral vascular ischaemia
C. gas embolism
D. renal failure
E. neurological injury
|
E
least likely:
The complications of IABP are:
• ischaemia of the leg
• dissection of the aorta
• thrombus formation and embolisation
• renal artery occlusion
• splenic mesenteric and spinal cord infarction
• internal mammary occlusion
• thrombocytopaenia
• infection
• gas embolisation
|
|
|
81. Remifentanil is
A. metabolised by non-specific esterases in the liver
B. metabolised by plasma cholinesterase
C. rapidly metabolised with a context sensitive half life of around 3 minutes regardless of infusion duration
D. rapidly metabolised with a context sensitive half life of around 3 minutes after a one hour infusion and around 7 minutes after a 6 hour infusion
E. metabolised by non-specific esterases in the kidney and liver
|
|
|
|
80. A patient presents to the pain clinic with phantom pains following a below knee amputation. The character of pain LEAST likely to respond to therapy is
A. burning
B. tingling
C. squeezing
D. shooting
E. crushing
|
E
crushing pain not typical of neuropathic pain
? some evidence that shooting pain responds less (anaesthesia MCQ)
|
|
|
79. Peri-operative beta-blockade has been shown to decrease the incidence of post-operative myocardial ischaemia. This is most likely due to
A. reduced hypertension in the post-operative period
B. reduced incidence of post-operative hypoxaemic episodes
C. reduced heart rates in the post-operative period
D. improved glucose metabolism in the post-operative period
E. reduction in post-operative hypercoagulability
|
|
|
|
78. The most common complication of blunt cardiac trauma is
A. myocardial ischaemia
B. valve rupture
C. right ventricular rupture
D. arrhythmias
E. tamponade
|
D
'The Heart in Blunt Trauma' Anesthesiology Volume 95(2), August 2001, p 544-548
"Myocardial contusion may induce severe complications, the most frequent being arrhythmias. Arrhythmias may occur after even minor
myocardial contusion..."
|
|
|
77. In patients with acute symptomatic post-operative hyponatraemia
A. men and women are equally susceptible and have similar risks for severe morbidity and mortality
B. rapid correction at a rate greater than 12 mmol.L-1 per day carries a risk of osmotic demyelination syndrome
C. treatment should consist of hypertonic saline alone and frusemide is relatively contra-indicated
D. mortality is less than 10% and is lower in children compared with adults
E. sodium deficit is calculated using the formula:
mmol Na required = (desired Na - present Na) x 0.4 x weight (kg)
|
B
• They are equally susceptible, but women appear to be at dramatically increased risk of severe morbidity and mortality (miller)
• Rate should be no more than 0.5mmol/hr (i.e. 12mmol/day). Oh’s: In the absence of good evidence, recommended rates at which to increase the sodium concentration vary from 0.5 to 2 mmol/l per hour
• Hypertonic saline alone doesn’t sound right. Frusemide would compound the problem by Na excretion
• Not sure
• deficit = 60% x wt (kg) x (desired -actual Na)
|
|
|
76. The potential adverse effect of 6 units of Fresh Frozen Plasma LEAST likely to be a problem is
A. an allergic reaction
B. a febrile reaction
C. a haemolytic reaction
D. transmission of infectious disease (including hepatitis and HIV infection)
E. citrate toxicity
|
D
Australian Red Cross:
• Allergy: 1% to 3% of plasma infusions
• Febrile reaction: 0.1% to 1% of transfusions
• Haemolysis: The most common cause is transfusion of ABO-incompatible blood. ABO incompatibility occurs in about 1:12,000 to 1:77,000 of transfusions
• Infection:
HIV (antibody + NAT) 5.6 days Less than 1 in 1 million(1)
HCV (antibody + NAT) 3.1 days Less than 1 in 1 million(1)
HBV (HBsAg + NAT) 23.9 days Less than 1 in 1 million(1)
HTLV 1 & 2 (antibody) 51 days Less than 1 in 1 million(1)
vCJD [No testing] Possible, not yet reported in Australia
Malaria (antibody) 7–14 days Less than 1 in 1 million(2)
• Miller: infusion of more than 1 unit of blood every 10 minutes is necessary for ionized calcium levels to begin to decrease
|
|
|
75. In cadaveric donor renal transplantation the intra-operative measure most likely to improve immediate graft function and transplant outcome is
A. administration of 200 mg frusemide intravenously prior to unclamping of the newly grafted kidney
B. aggressive intra-operative volume expansion to central venous pressures of 10-15 mmHg
C. administration of 50 g mannitol intravenously prior to unclamping of the newly grafted kidney
D. use of a low dose dopamine infusion (2 g.kg-1.min-1) peri-operatively
E. administration of 0.8 g.kg-1 albumin intravenously prior to unclamping of the newly grafted kidney
|
B
Yao & Artusio:
“Probably the most important determinant of IMMEDIATE renal function ... is adequacy of perfusion of the transplanted kidney at the time when the vascular clamps are released. CVP should be used to guide fluid therapy... a cadaveric kidney seems to require higher arterial blood pressure and larger plasma volume to initiate diuresis than a normal kidney. Systolic BP is kept around 130 to 160mmHg and CVP around 10 to 15cmH20”
Mannitol given immediately before removal of the vessel clamps reduces the requirement of post-transplant dialysis, but has no effects on graft function in the long term
|
|
|
74. The incidence of vertebral artery injury in patients with cervical fractures or dislocations is
A. 1%
B. 10%
C. 40%
D. 70%
|
C
Though the answer seems to be more around 20%
Medscape
- Vertebral artery occlusion can be considered a common complication in approximately 20% of cervical spine fractures and/or dislocations.
Injury Volume 32, Issue 7, October 2001, Pages 565-568:
- Forty-seven patients with cervical spine trauma were evaluated prospectively with magnetic resonance imaging (MRI) and angiography (MRA) to determine the incidence of vertebral artery injury. Twelve patients (25%) had vertebral artery injuries
|
|
|
73. Post-operative ulnar neuropathy
A. usually presents within 48 hours of surgery
B. symptoms usually persist for over two years
C. is more common in men
D. can usually be avoided by careful positioning
E. can usually be avoided by protective padding of the elbow
|
C
Anesthesiology Clin N Am 20:(2002) 589– 603:
"This bony prominence is at least 50% larger in males, consistent with their greater susceptibility to perioperative ulnar nerve damage
|
|
|
72. When a new diagnostic test is evaluated in a group of subjects in whom the diagnosis is known, the following results are obtained.
Disease known Disease known
to be present to be absent
Test result positive x y
Test result negative 30 60
If a subject from this population tests negative, the probability of NOT having the disease is
A. unable to be calculated because “x” is unknown
B. unable to be calculated because “y” is unknown
C. unable to be calculated because “x” and “y” are unknown
D. 0.33
E. 0.67
|
E
NPV which = TN/(TN + FN) = 0.67
Sensitivity = TP / TP + FN = TP rate
Specificity = TN / TN + FP = TN rate
PPV = TP / TP + FP = probability of true positive given positive test result
NPV = TN / TN + FN = probability of true negative given negative test result
False positive rate = FP / TN + FP = 1 – spec
False negative rate = FN / TP + FN = 1 – sens
|
|
|
71. A permanent dual-chamber transvenous pacemaker set to a DDDR mode will
A. NOT be affected by diathermy
B. increase the ventricular pacing rate if the minute volume is increased
C. usually require reprogramming to VVO mode for surgery
D. revert to DDD mode if a magnet is placed over the generator site
E. result in a tachyarrhythmia if the patient develops atrial flutter
|
B
Will be affected by diathermy
Rate response does lead to increased pacing rate
Usually an asynchronous mode like VOO
Magnet usually reverts to an asynchronous mode
Would only happen if the AV node was intact
|
|
|
70. Conditions which cause a metabolic acidosis with normal anion gap include
A. chronic renal failure
B. diabetic keto-acidosis
C. salicylate poisoning
D. renal tubular acidosis
E. ethylene glycol poisoning
|
D
Causes of normal AG metabolic acidosis:
- renal tubular acidosis
- diarrhoea
- biliary / pancreatic fistulae
- excessive infusion of normal saline
|
|
|
69. Obstructive sleep disorder in children
A. is associated with pulmonary hypertension and dysfunction of left and right ventricles
B. has obesity as a major risk factor
C. is rarely seen in children less than 8 years old
D. is four times more prevalent in boys than girls
E. does NOT usually require tonsillectomy for its management
|
A
A. "Children with long-standing OSA syndrome who become chronically hypoxaemic and hypercarbic may develop acute respiratory failure and right ventricular failure." (Anaesthesia 1998; 53:571-579)
B. partly true: Definitely a risk factor in the fat kiddies, but is it a major risk factor?
"Obesity, a typical feature of adults with OSA, is uncommon in children but if observed, may be associated with reduced daytime activity. More typically these children have poor weight gain and small stature." (Anaesthesia 1998; 53:571-579)
C. "Children usually present between 3 and 7 years of age" (Anaesthesia 1998; 53:571-579)
D "In contrast with adult OSA, in children there is an equal prevalence of affected boys and girls" (Anaesthesia 1998; 53:571-579)
E. "In most cases the definitive treatment of children with OSA syndrome is surgical by adenotonsillectomy" (Anaesthesia 1998; 53:571-579)
|
|
|
68. When a reaction to an anaesthetic drug is suspected
A. the single most useful test to confirm a reaction is mast cell tryptase sampled 20-24 hours after the event
B. the single most useful test to confirm a reaction is mast cell tryptase sampled 8-12 hours after the event
C. the most valuable test to identify the drug responsible is radioimmunoassay (RAST)
D. the morphine IgE radioimmunoassay is a sensitive and efficient test for the detection of IgE antibodies to neuromuscular blocking drugs
E. the absence of an elevated mast cell tryptase (sampled at an appropriate time) excludes a Type I hypersensitivity reaction
|
D
- Tryptase levels rise within 1 hour and remain elevated for 4-6 hours
- Anaesth Intensive Care 2000; 28: 167-170 Immunoassays in the Diagnosis of Anaphylaxis to Neuromuscular Blocking Drugs: The Value of Morphine for the Detection of IgE Antibodies in Allergic Subjects:
o "The morphine RIA proved to be both a more sensitive and efficient test for the detection of IgE antibodies to NMBDs than the specific NMBD RIAs."
- RCPA Manual:
o "A negative result does not exclude an allergic basis especially with anaphylaxis following food ingestion."
|
|
|
67. Hypothermia during anaesthesia readily occurs in the elderly compared with younger adults because
A. basal metabolic rate increases with age
B. heat production increases with age
C. thermo-regulatory vasoconstriction is impaired during general anaesthesia
D. greater heat losses occur during surgical skin preparation
E. the fall in core temperature required to trigger shivering is increased during spinal blockade
|
C
Miller:
Thermoregulatory vasoconstriction is comparably impaired in infants, children, and adults given isoflurane or halothane. In contrast, the vasoconstriction threshold is about 1°C less in patients aged 60 to 80 years than in those between 30 and 50 years old
|
|
|
66. A 16 kilogram, 3 year old boy for unilateral inguinal herniotomy has general anaesthesia and a caudal with 8 mls of 0.25% plain bupivacaine. The LEAST correct statement regarding this anaesthetic management is that
A. the required level of the block is T12
B. the volume of local anaesthetic used is inadequate
C. the block duration is the same for all segments
D. peripheral nerve blocks are safer than neural axis blocks in children
E. use of adrenaline in the local anaesthetic would prolong the block
|
C
C seems the most wrong, though
- T12 maybe just low enough
- caudal dose is 1ml/kg
|
|
|
65. FALSE statements regarding natural latex rubber allergy include
A. sensitivity of skin prick testing is greater than that of specific IgE antibody detection (RAST)
B. signs of Type I hypersensitivity are usually immediate
C. latex antibodies fall in time in a latex free environment
D. the risk factors of frequent exposure and atopy are additive
E. theatre latex aerogens are lowest in the morning
|
B
Latex allergy: an update from ANESTH ANALG 2003;96:1219–29:
- RAST tests are highly specific, but their sensitivity is low... (while) the skin-prick test was very sensitive and specific
- Latex proteins are absorbed slowly when the exposure is airborne, and symptoms usually develop approximately 30 min after exposure." (Hepner and Castells,)
- A recent follow-up study (72) on latex allergy in health care workers demonstrated that although the skin-prick test remained positive 2 yr after latex avoidance, latex specific IgE levels decreased in most patients
- The American Society of Anesthesiologists Task Force of Latex Sensitivity recommends that patients who are latex allergic have a surgical procedure performed as the first case in the morning, when the levels of latex aeroallergens are the smallest
|
|
|
64. The MAC (minimal alveolar concentration) and blood/gas partition coefficient of desflurane are
A. 2% and 0.47 respectively
B. 4% and 0.47 respectively
C. 6% and 0.67 respectively
D. 6% and 0.42 respectively
E. 8% and 1.4 respectively
|
|
|
|
63. A 91 year old farmer presents for anaesthesia for a total hip replacement. He gives a history of failed endotracheal intubation with his last two anaesthetics, probably due to arthritis of the cervical spine. The rest of the history and examination is unremarkable. His American Society of Anesthesiologists Physical Status Score (ASA Status) is
A. ASA 1
B. ASA 2
C. ASA 3
D. ASA 4
E. ASA 5
|
B
Classing arthritis of spine as mild systemic disease
|
|
|
62. A 48 year old patient with traumatic brain injury from a motor vehicle accident is ventilated and sedated with propofol. The patient subsequently receives ketamine 5 mg.kg-1 intravenously. The most likely consequence of the ketamine administration is
A. a decrease in intracerebral pressure
B. a worse outcome from the brain injury
C. an increase in mean arterial pressure
D. an increase in cerebral arterio-venous oxygen content difference
E. an increase in middle cerebral artery blood flow
|
A
5mg/kg is a pretty big dose.
Ketamine Decreases Intracranial Pressure and Electroencephalographic Activity in Traumatic Brain Injury Patients during Propofol Sedation., Anesthesiology. 87(6):1328-1334, December 1997:
- In sedated and ventilated patients with traumatic brain injury, ketamine decreases ICP, does not decrease MAP, and AVDO2 and VMCA, do not change
- there were no statistically significant variations in heart rate, MAP, and CPP
- During the study period pH, PaO2, paC sub O2, AVDO2, and LOI remained unchanged
- No change was observed in VMCA
|
|
|
61. Normal features of changing physiology with age include
A. increased lean body mass
B. increased adrenal-cortical function
C. earlier onset of shivering
D. increased plasma albumin
E. decreased gastric pH
|
B
Miller:
"Changes in body composition with aging reflect a decrease in lean body mass, an increase in body fat, and a decrease in total body water”
"Production of androgens by the adrenal gland progressively decreases with age “, “Plasma levels of cortisol are unaffected by increasing age”
The shivering set point is decreased in the elderly so shivering occurs later. "the vasoconstriction threshold is about 1°C less in patients aged 60 to 80 years than in those between 30 and 50 years... Shivering is … roughly 1°C less than the vasoconstriction threshold."
"The circulating level of albumin decreases with age, whereas α1-acid glycoprotein levels increase."
Apparently gastric pH is increased
|
|
|
60. A healthy 20 year old patient undergoing nasal surgery under general anaesthesia has the nose packed with gauze soaked in 0.5% phenylephrine and a submucosal injection of lignocaine with 1:100,000 adrenaline. Over the next 10 minutes the blood pressure rises from 130/80 to 220/120 mmHg and the heart rate from 60 to 100 beats per minute. The LEAST appropriate management of this situation would be to
A. deepen anaesthesia with isoflurane
B. administer labetalol
C. watch and observe
D. administer glyceryl trinitrate
E. administer sodium nitroprusside
|
B
Negative inotropy against tight circulation
Controversial as there are case reports of pulmonary oedema and cardiac arrest following administration of beta-blockers in this situation
|
|
|
59. In assessing the adequacy of oxygen delivery to meet the body's oxygen demands the best indicator is
A. arterial PO2
B. arterio-venous oxygen content difference
C. oxygen flux calculation
D. mixed venous PO2
E. cardiac output
|
|
|
|
57. Systemic vascular resistance index (SVRI) is calculated from
A. systemic vascular resistance multiplied by body surface area
B. systemic vascular resistance divided by body surface area
C. mean aortic and central venous pressure difference divided by cardiac output
D. cardiac index divided by the mean aortic and central venous pressure difference
E. none of the above
|
A
Miller:
"The appropriate formulas are SVR index = SVR x BSA,
and PVR index = PVR x BSA"
i.e. SVRI = ((MAP-CVP)*80)/CI
so,
SVRI = ((MAP-CVP)*80)/(CO/BSA)
SVRI = ((MAP-CVP)*80)*(BSA/CO)
SVRI = (((MAP-CVP)*80)/CO)*BSA
SVRI = SVR * BSA
|
|
|
54. In an acute malignant hyperthermia episode
A. the serum creatinine kinase level peaks within one hour
B. the peak serum creatinine kinase level is a good indicator of the amount of muscle involved
C. elevated creatinine kinase levels contribute to acute renal failure
D. the serum myoglobin level does NOT peak for at LEAST 24 hours
E. muscle rigidity occurs in 75% of cases
|
E
In an acute malignant hyperthermia episode
A. the serum creatinine kinase level peaks within one hour - false: "Additional features that increase the likelihood of underlying MH are signs of metabolic stimulation and grossly elevated plasma creatine kinase (CK) and myoglobin concentrations. There may also be evidence of myoglobinuria; this occurs earlier than CK increases. CK reaches a peak approximately 24 h after the insult and, even in patients with no muscle disorder, can reach 50 times the upper limit of normal." (Malignant hyperthermia BJA CEPD Reviews 2003 Feb 01, 3: 5-9.)
B. the peak serum creatinine kinase level is a good indicator of the amount of muscle involved - false: "The CK increase resulting from surgery is similar to that seen after these acute MH episodes because of coincident muscle damage, but it also may be a result of CK release from other tissues. CK is found in brain and intestinal tissue; CK may increase substantially after a bowel infarction (6). Maternal labor appears to increase CK, possibly in relation to physical exertion (e.g., pushing) during the second stage of labor (14,15). Other conditions associated with increased CK include myocardial infarction (6), fever (16), stroke (17), and tubal pregnancy" (A & A November 1995 vol. 81 no. 5 1039-1042)
C. elevated creatinine kinase levels contribute to acute renal failure - false: "Plasma myoglobin concentrations are sufficient to cause renal tubular damage and acute renal failure." (Malignant hyperthermia BJA CEPD Reviews 2003 Feb 01, 3: 5-9.)
D. the serum myoglobin level does NOT peak for at LEAST 24 hours - false: "Increases in serum myoglobin occur earlier after muscle injury than increases in CK. Peak levels of CK may not be observed until 12 to 24 hours after muscle injury." (Malignant hyperthermia and myotonic disorders, Anesthesiology Clinics of North America - Volume 20, Issue 3 (September 2002))
E. muscle rigidity occurs in 75% of cases - true: "The occurrence of generalized muscle rigidity is the most specific sign of MH [11] [12]" (Malignant hyperthermia and myotonic disorders, Anesthesiology Clinics of North America - Volume 20, Issue 3 (September 2002))
|
|
|
53. To rule out raised intracranial pressure in an awake patient, the most reliable finding is
A. absence of papilloedema
B. presence of retinal vein pulsation
C. absence of headache
D. absence of diplopia
E. absence of vomiting
|
B
J Neurol Neurosurg Psychiatry 2003;74:7-9: Spontaneous retinal venous pulsation: aetiology and significance
“as the intracranial pressure rises the intracranial pulse pressure rises to equal the intraocular pulse pressure and the spontaneous venous pulsations cease. Thus it is shown that cessation of the spontaneous venous pulsation is a sensitive marker of raised intracranial pressure”
|
|
|
51. In ARDS (Adult Respiratory Distress Syndrome),
A. ECMO (extra-corporeal membrane oxygenation) has been shown to improve survival
B. inverse ratio ventilation improves oxygenation in most patients
C. high frequency ventilation improves oxygenation in most patients
D. steroids are indicated only if sepsis is present
E. limiting peak inspiratory pressure does NOT reduce barotrauma
|
E
American thoracic society - EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) IN PATIENTS WITH ARDS
“ECMO has not clearly been demonstrated to improve outcome compared to standard of care management of adult ARDS”
Mixed evidence for IRV – certainly doesn’t appear to be most patients
Two RCTs comparing HFOV to conventional ventilation revealed encouraging results but failed to show a mortality benefit of HFOV over conventional ventilation
NEJM ARDSnet study 2006 - no benefit to using steroids
Limiting plateau pressure rather than peak is what reduces barotrauma
|
|
|
50. With respect to general anaesthesia for caesarean section
A. ketamine is NOT appropriate as an intravenous induction agent
B. rapacuronium has a similar onset of action to suxamethonium
C. awareness can be reduced by use of bispectral index monitoring
D. inhalational anaesthetics should be discontinued after delivery
E. fetal outcome is significantly improved by the use of 100% oxygen at emergency caesarean section
|
C
B-aware trial – BIS monitoring reduced risk of awareness by 82% in GA caesarians
Rapacuronium does have a similar onset time to sux though
|
|
|
47. Masseter muscle spasm in response to suxamethonium
A. has an incidence of 0.03-0.1%
B. is associated with a likelihood of malignant hyperpyrexia of 40- 60%
C. requires immediate discontinuation of the anaesthetic if the mouth is unable to be opened
D. is associated with pseudocholinesterase deficiency
E. is NOT seen if the patient has been pre-treated with a small dose of a non-depolarising muscle relaxant
|
|
|
|
46. Trans-cranial doppler monitoring of middle cerebral artery flow velocity
A. enables easy comparison of bilateral flow
B. enables diagnosis of embolism during carotid endarterectomy
C. distinguishes between changes in intracranial pressure (ICP) and changes in intracranial vessel tone
D. shows flow reversal if the ICP is less than the diastolic arterial pressure
E. has a lower failure rate in females
|
B
ANZCA Blue Book 2003 'Transcranial Doppler Ultrasound' and Miller
Option A – False, Bilateral flow is easily detected however does not correlate well to adequate perfusion of the brain.
Option B - True and best answer. Reference Miller 6th Edition. TCD is used for the detection of embolism.
Option C - False. TCD by its nature is 'doppler' and doppler shift is related only to flow characteristics. Flow may be affected by vessel tone (ie basis of vasospasm detection at day 7-10), but is unable to determine changes in pressure.
Option D - False.
Option E - False. TCD has a higher failure rate in females due to smaller acoustic window
|
|
|
45. A low ejection fraction is most likely to be seen in a patient with
A. poor left ventricular (LV) systolic function
B. poor LV systolic function and severe mitral regurgitation
C. poor LV diastolic function
D. septic shock
E. a post myocardial infarct ventricular septal defect
|
A
MR leads to decreased ESV as blood regurgitating into atrium during systole. EF = (EDV-ESV)/EDV, therefore EF not decreased
|
|
|
39. Regional anaesthesia for modified radical mastoidectomy requires blockade of the following nerves EXCEPT
A. greater auricular
B. auriculotemporal
C. auricular branch of vagus
D. facial
E. tympanic branch of glossopharyngeal
|
D
The surgeon would probably want to monitor facial nerve function rather than have it blocked
|
|
|
36. Radiation from X-rays
A. has a non-cumulative effect on the bone marrow
B. affects the thyroid gland more in patients over 16 years old
C. has a recommended maximum whole body dose for the general population of 1,000 µSv.year-1
D. should be limited to less than 100 µSv.year-1 in pregnancy
E. has a recommended maximum whole body dose for occupational exposure of 500,000 µSv.year-1
|
C
Radiation safety for anaesthesiologists:
- Effects are cumulative
International Commission on Radiological protection (ICRP): recommended dose limits:
Occupational Exposure:
Employees 18yrs and over: maximum annual whole body dose 50mSv (50,000µSv) in any one year with maximum of 100mSv in 5years (20mSv/year when averaged over 5yrs).
Limit to abdomen of women of reproductive capacity 13mSv (13,000µSv) in any 3mth period.
Trainees <18yrs: maximum annual whole body dose 6mSv (=6000µSv)
General Public: maximum annual whole body dose 1mSv (=1000µSv).
In special circumstances a higher value of effective dose could be allowed in a single year, provided that the average over 5yrs does not exceed 1mSv/yr.
|
|
|
35. A Swan-Ganz catheter can be unreliable for measuring pulmonary artery systolic and diastolic pressures because the length and compliance of the tubing affects the measuring system by
A. reducing its resonant frequency
B. reducing its frequency response
C. reducing its damping coefficient
D. inducing a zero error
E. inducing baseline drift
|
A
Kerry Brandis:
Long compliant tubing
- reduces the resonant frequency
- increases the damping coefficient
E - Wrong; length & compliance of the the tubing does NOT cause baseline drift. A baseline drift will affect the accuracy of sys & dias but this is not related to the tubing length and compliance
D - Wrong; zero errors are caused by incorrectly zeroing the system, and not by the tubing. A zero error will result in inaccurate recording of sys & dias pressures but this error is not related to the length & compliance of the tubing.
C: - Increased length & compliance results in increased damping. The effect of this though is dependent on the actual value of the damping coefficient. For example if the damping coefficient is increased to 0.64 (optimal damping) then depending on the frequency response and the resonant frequency (these 2 are inter-related) of the system then it is possible that the systolic & diastolic may be recorded MORE accurately.
B - The useable frequency response is decreased by a reduced resonant frequency, but the effect of this is dependent on the actual value of the damping coefficient AND the . It is however also determined by the damping coefficient. The optimum frequency response is obtained with a high resonant frequency and if this is very high (as in some catheter tip transducers) then the damping coefficient is unimportant. However in clinical catheter transducer systems, the damping coefficient is typically low (eg values in the range 0.2 to 0.3 would be common).
A - Resonant frequency is decreased by long tubing and systolic & diastolic pressures would be less accurately recorded.
|
|
|
33. Bowel preparation for colonoscopy
A. may cause hypophosphaturia, hypercalcaemia and dehydration
B. can be avoided in high risk patients
C. no longer causes significant fluid loss with modern formulations
D. may cause Trousseau’s sign to be positive
E. may result in arrhythmias and a shortened QT interval
|
D
Bowel Preparation: Current Status
Clin Colon Rectal Surg. 2009 February; 22(1): 14–20
“Electrolyte alterations that may occur include hyperphosphatemia, hypocalcemia, hypernatremia, and hypokalemia, which in most patients are minimal and or transient in nature”
Still fluid loss with newer preps
Trousseau’s sign is for hypocalcaemia – BP cuff inflated above SBP for 3min. leads to spasm of hand/wrist muscles if positive
B seems correct also – certainly have seen this done
|
|
|
32. A two year old child sustains a simple fracture of the lower end of the forearm one hour after having a full meal. The most appropriate approach is to
A. postpone surgical reduction for 12 hours and treat as an elective case
B. allow immediate reduction using a rapid sequence induction, cricoid pressure and intubation
C. allow immediate reduction using a regional technique
D. allow immediate reduction, after gastric emptying with a tube followed by rapid sequence induction, cricoid pressure and intubation
E. wait 4 hours and treat as elective
|
A
Controversial
- No urgency to perform immediately
- Ideally delay 6hrs + RSI
- There should be some gastric emptying, especially if the arm is immobilized and pain controlled.
|
|
|
30. The hyperglycaemic hyperosmolar non-ketotic syndrome
A. may be associated with a high serum sodium
B. only occurs in elderly patients
C. is commonly complicated by thromboembolism
D. is characterized by only a moderate degree of hyperglycaemia
E. is NOT characterized by dehydration
|
A & C
Na could be up or down. Some sources say thromboembolism is common
Typically middle aged to elderly type II diabetic patients
25% are undiagnosed diabetics
Relatively uncommon but has high mortality (up to 15%)
Precipitants
Infection
Myocardial infarction
Diabetogenic or dehydrating drugs (e.g. diuretics, steroids, beta blockers)
Other
Thromboembolic complications common
|
|
|
29. Carbon monoxide poisoning results in hypoxic injury by
A. reducing the arterial pO2
B. shifting the oxygen-haemoglobin dissociation curve to the right
C. decreasing alveolar ventilation
D. increasing the number of oxygen binding sites available on haemoglobin
E. binding to mitochondrial cytochrome oxidase
|
|
|
|
28. A previously healthy 35 year old diesel mechanic gives a two year history of intermittent but progressive weakness on exertion in the hands and arms. He recently developed diplopia whilst driving his car home from work. He smokes 10 cigarettes and drinks one bottle of beer per day. The most likely diagnosis is
A. myasthenic syndrome
B. toxic peripheral neuropathy
C. syringomyelia
D. fascioscapulohumeral muscular dystrophy
E. none of these
|
E
Myasthenic syndrome (not gravis) = eaton lambert. Exercise improves weakness, no ocular involvement
B, C & D woulnd’t affect vision
MS would be another possibility
|
|
|
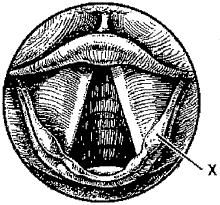
27. The feature indicated by the line 'X' is the
A. cuneiform cartilage
B. vestibular fold
C. vallecula
D. corniculate cartilage
E. arytenoid cartilage
|
|
|
|
26. When using low-flow circle absorber techniques, the uptake of nitrous oxide must be considered. In a healthy 70 kg adult the expected uptake of nitrous oxide, with a 70% inspired concentration, after 1.5 hours would be about
A. 1000 mL.min-1
B. 500 mL.min-1
C. 250 mL.min-1
D. 100 mL.min-1
E. <50 mL.min-1
|
D
Severinghaus formula: uptake of N2O (in mls/min) is equal to 1000 divided by the square root of the time elapsed (in mins)
1000/10 = 100ml/min
|
|
|
20. During cardio-pulmonary bypass perfusion for cardiac surgery, total body hypothermia is often utilised. This hypothermia
A. will NOT ensure, on its own, amnesia and analgesia below a core temperature of 30 degrees Celsius
B. increases the transfer of oxygen from blood to tissues due to a shift in the oxygen-haemoglobin dissociation curve
C. induces some degree of red blood cell lysis
D. decreases the solubility of oxygen in arterial blood
E. results in decreased effectiveness of heparin as an anticoagulant
|
A
A seems obvious
B – no the curve shifts to the left
C – not that I know of
D – Yes, as temp decreases there will be less oxygen entering gas phase above the liquid
E – not that I know of
|
|
|
18. A 30 year old male presents with a single sudden shaking chill with a rapid rise in temperature. Within a few hours agonizing left pleuritic pain and cough with rust coloured sputum supervene. On examination the man appears acutely ill with rapid shallow respiration. With no treatment he continues to run a temperature up to 40.5C for a week at which time he experiences a dramatic improvement. Physical examination on day 2 of the illness would probably show all of the following over the left chest
EXCEPT
A. restricted hemithorax movement
B. flat percussion sound
C. bronchial breathing
D. decreased fremitus
E. whispering pectoriloquy
|
D
Should be increased fremitus
|
|
|
17. In a patient undergoing a femoro-popliteal bypass, the most predictive independent risk factor for the development of post-operative myocardial infarction would be
A. a previous history of coronary artery bypass grafts
B. diabetes mellitus
C. an episode of intra-operative myocardial ischaemia
D. hypercholesterolaemia
E. an episode of post-operative myocardial ischaemia lasting over 60 minutes
|
|
|
|
16. The lobar collapse which is most easily missed on chest X-ray, is
A. right upper lobe
B. left lower lobe
C. right lower lobe
D. left upper lobe
E. right middle lobe
|
B
From cardiac silhouette obscuring view
|
|
|
15. A 30 year old man has received 40 units of packed red blood cells as rapidly as possible. At the end of the first hour of care the LEAST likely complication is
A. metabolic acidosis with increased anion gap
B. metabolic alkalosis due to citrate toxicity
C. coagulation abnormalities
D. hypocalaemia
E. shift of the oxygen-haemoglobin dissociation curve to the left
|
B
Citrate is metabolized to HCO3 so alkalosis can occur, but I don’t think this would be the most likely. Acidosis is surely more likely in the first hour
Coagulopathy definitely possible
Hypocalcaemia from citrate effect
Decreased 2,3DPG with stored blood leads to left shift
|
|
|
13. The following blood gas result is from a patient breathing room air who has been unwell for three days
pH 7.56
PCO2 46 mmHg PO2 90 mmHg HCO3 39 mEq.L-1 B.E. +16.2 mEq.L-1
These results can best be described as
A. primary respiratory acidosis with metabolic compensation
B. uncompensated primary metabolic alkalosis
C. compensated secondary respiratory alkalosis
D. primary metabolic alkalosis with partial respiratory compensation
E. mixed metabolic and respiratory alkalosis
|
D
Expected CO2 in metabolic alkalosis is = 0.7 x HCO3 + 20
Therefore expected CO2 = 47
|
|
|
11. Nitric oxide, when used as supportive treatment for adult respiratory distress syndrome,
A. potentiates the effect of the endothelial releasing factor in the lungs
B. must be given by inhalation as it is rapidly metabolised by leucocytes
C. may cause systemic hypotension when administered in a concentration of about 40 ppm
D. must be administered continuously as the effect lasts only about 30 minutes
E. will reduce the venous admixture when administered in a concentration of 20 ppm4
|
E
Half-life is <5sec
Oh’s Intensive Care:
“Binding to haemoglobin in the pulmonary circulation rapidly inactivates NO, and systemic effects are only reported following high concentrations of iNO”
“Doses as low as 60 parts per billion iNO may improve oxygenation; however, commonly used doses in ARDS are 1–60 parts per million, with the higher doses required for reduction in pulmonary artery pressure”
“Although clinical trials have shown no improvement in mortality or reversal of ALI, iNO was safe and did significantly improve oxygenation initially (as compared to placebo or no iNO), but this was not sustained beyond 12–24 hours”
|
|
|
9. If the tracheal diameter measured on a PA chest X-ray at the level of the sternoclavicular joint is between 16mm and 18mm, the best choice of double lumen tube would be
A. 41 Fr
B. 39 Fr
C. 37 Fr
D. 35 Fr
E. 33 Fr
|
B
(2 x trachea) + 5
= (2 x 17) + 5
= 39
|
|
|
8. You are assessing the circulation of a patient using a pulmonary artery catheter. The mean arterial blood pressure is 100 mmHg, CVP is 5 mmHg. The pulmonary capillary wedge pressure is 15 mmHg and the
cardiac output is 5 L.min-1. In this patient the systemic vascular resistance (in dynes.sec.cm-5) is
A. 3.2
B. 3.8
C. 150
D. 1280
E. 1520
|
|
|
|
7. During one lung ventilation, hypoxic pulmonary vasoconstriction in the non-ventilated lung
A. is increased by high pulmonary artery pressures
B. is increased by applying PEEP (positive end-expiratory pressure) to the ventilated lung
C. reduces the shunt fraction by approximately 50%
D. is abolished by isoflurane
E. is increased by hyperventilation
|
C
Almost repeat from previous exam
CEACCP 2002
"Another mechanism for shunt reduction is regional hypoxic pulmonary vasoconstriction which actively divers blood flow from hypoxic to well oxygenated lung. It is an active process, triggered by alveolar hypoxia, which results in a 50% reduction in blood flow to the atelectatic lung."
|
|
|
5. When used to prevent aspiration pneumonitis
A. ranitidine has a similar onset time and a shorter duration of action than cimetidine
B. anticholinergic drugs increase gastric acidity and increase lower oesophageal sphincter tone
C. non-particulate antacids have a longer duration of action than particulate antacids
D. metoclopramide increases the lower oesophageal sphincter tone but relaxes the pyloric sphincter
E. suxamethonium reduces the barrier pressure in most adults
|
D
Cimetidine: onset 1-2hrs, duration 4-8hrs;
Ranitidine: onset 1-2hrs, duration 10-12hrs (Morgan & Mikhail, clinical anaesthesia pg 244)
Anticholinergic drugs decrease acidity
Non-particulate antacids have a MORE rapid action and shorter duration than particulate antacids (Morgan & Mikhail pg 245)
Suxamethonium increases LOP pressure AND intragastric pressure such that barrier pressure is little affected. (Peck & Williams)
|
|
|
3. Haemophilia can cause
A. Henoch-Schonlein purpura
B. a prolonged skin bleeding time
C. a prolonged partial thromboplastin time
D. impaired clot retraction
E. afibrinogenaemia
|
C
Henoch-Schönlein purpura is a small-vessel vasculitis in which complexes of immunoglobulin A (IgA) and complement component 3 (C3) are deposited on arterioles, capillaries, and venules
Skin bleeding time is a measure of platelet function
Stoelting:
“Similar to the laboratory findings with hemophilia A, hemophilia B patients have a prolonged PTT and a normal PT”
Clot retraction is a measure of clot lysis
|
|
|
2. When anaesthetising a patient with an acute pericardial tamponade,
A. the patient may be safely induced with a dose of 3-5 mg.kg-1 of thiopentone
B. it is important to limit intravenous fluid infusion, to prevent further compression of the heart
C. it is important to reduce afterload
D. a slow heart rate allows time for optimal filling of the ventricle
E. awareness is a potential problem after release of the tamponade
|
|
|
|
1. Carotid endarterectomy for symptomatic carotid disease
A. has a peri-operative stroke rate of 8 to 10%
B. should be performed under regional anaesthesia in patients with ischaemic heart disease to reduce the incidence of myocardial infarction
C. may be performed under induced hypotension to reduce intra-operative blood loss
D. when performed under deep cervical plexus block is often associated with a phrenic nerve palsy
E. should be performed under regional anaesthesia in patients with a recent transient ischaemic attack to reduce the incidence of peri-operative stroke
|
D
BJA Review – Carotid Endarterectomy
“The pooled meta-analysis data discussed earlier rank myocardial infarction second to stroke as a complication of endarterectomy with rates of 3.4 and 2.2%, respectively”
No articles report MI being less common with regional anaesthesia
Anaesthesia techniques for carotid surgery A&IC 2007:
Deep cervical plexus block has phrenic nerve palsy rate of 60%, though is usually well tolerated
GALA trial – large RCT comparting regional vs GA:
No definite difference in outcomes with regional vs GA
|