Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
72 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Common dermatomal reference for back of head?
|
C2
|
|
|
|
Common dermatomal reference for nipples?
|
T4
|
|
|
|
Common dermatomal reference for thumb and index finger?
|
C6
|
|
|
|
Common dermatomal reference for umbilicus?
|
T10
|
|
|
|
Common dermatomal reference for kneecap?
|
L3
|
|
|
|
Common dermatomal reference for lateral foot?
|
S1
|
|
|
|
Through which openings do the vertebral arteries run?
|
Transverse foramina of C6-C1
|
|
|
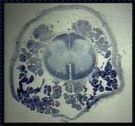
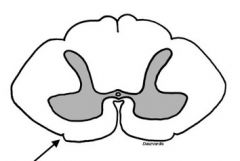
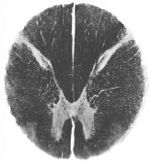
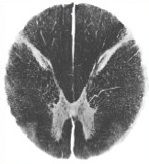
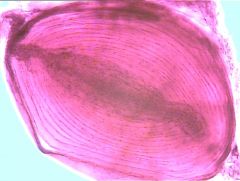
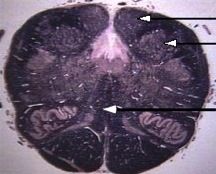
What level of the CNS does this image represent?
|
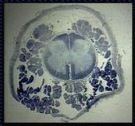
Sacral - note presence of spinal cord AND cauda equina.
|
Note presence of both spinal cord and cauda equina.
|
|
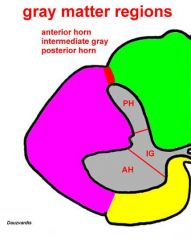
What information does the dorsal/posterior horn carry?
|
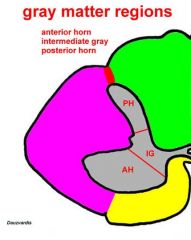
Sensory (GSA, GVA)
|
|
|
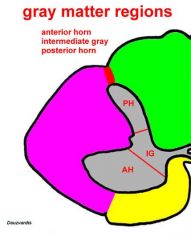
What information does the intermediate horn carry?
|
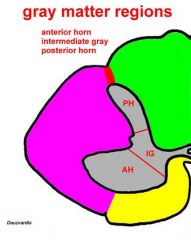
Both sensory and motor
|
|
|
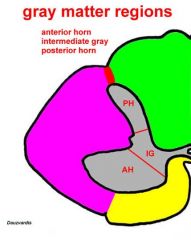
What information does the anterior (ventral) horn carry?
|
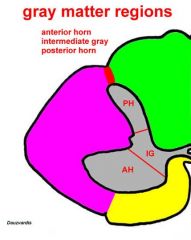
Motor (GVE, GSE)
|
|
|
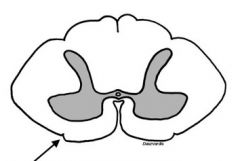
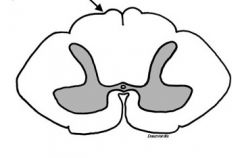
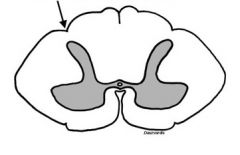
Identify structure at arrow.
|
Anterior/Ventral Commissure:
White matter connection b/t left and right spinal cord |
|
|
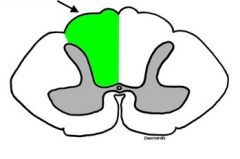
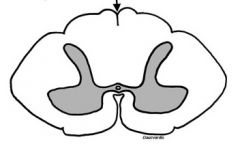
Identify structure at arrow.
|
Anterior Funiculus
|
|
|
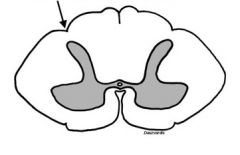
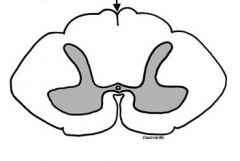
Identify structure at arrow.
|
Anterior Lateral Sulcus
|
|
|
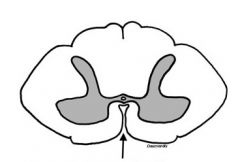
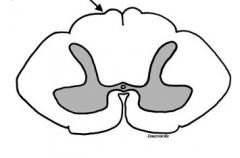
Identify structure at arrow.
|
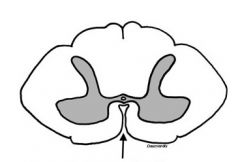
Anterior Median Fissure
|
|
|
Identify structure at arrow and describe its significance.
|
Dorsolateral Fasciculus (or Zone/Tract of Lissauer); contains axons originating in substancia gelatinosa, involved in sensory modulation
|
Zone of Lissauer
|
|
Identify structure at arrow.
|

Lateral funiculus
|
|
|
Identify structure at arrow.
|
Posterior funiculus
|
|
|
Identify structure at arrow.
|
Posterior Intermediate Sulcus
|
|
|
Identify structure at arrow.
|
Posterior Lateral Sulcus
|
|
|
Identify structure at arrow.
|
Posterior Median Sulcus
|
|
|
|
Definition of nucleus?
|
A group of neurons with a common function or modality. Ex: hypoglossal nucleus = motor to the tongue (GSE)
|
|
|
|
GSA?
|
General Somatic Afferent
*Innervates skin, muscle spindles, tendons, and joints *Exteroception (touch, temp, pain, itch, vibration) *Proprioception (limb position and movement) |
|
|
|
GSE?
|
General Somatic Efferent; motor to "common" skeletal muscle.
-Innervates skeletal muscle derived from myotomes |
|
|
|
GVA?
|
General Visceral Afferents
*From "guts" *Innervates viscera (heart, GI tract, etc.) *Interoception (GI tract and bladder stretch, pH in blood) |
|
|
|
GVE?
|
General Visceral Efferents; preganglionic autonomic fibers to guts, glands, and blood vessels.
-Innervates smooth and cardiac muscle and glands |
|
|
|
SSA?
|
Special Sensory Afferents
*From "external" special sense organs *Teloception (vision, audition, balance) |
|
|
|
SVA?
|
Special Visceral Afferents
*From "internal" special sense organs (taste, olfaction) |
|
|
|
SVE?
|
Special Visceral Efferents; motor to "gill" muscles.
-Innervates skeletal muscle derived from branchial arches |
|
|
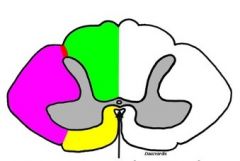
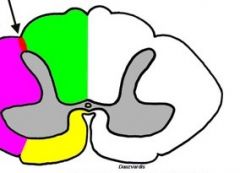
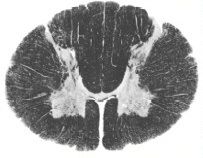
What level of the CNS does this image represent?
|
C2
|
|
|
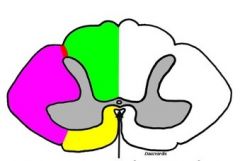
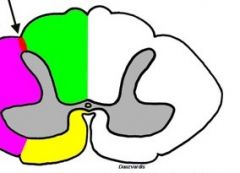
What level of the CNS does this image represent?
|
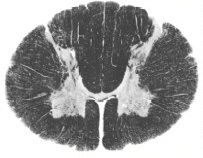
C8
|
|
|

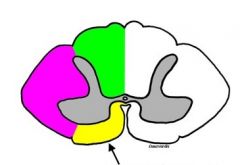
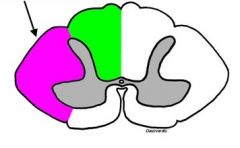
What level of the CNS does this image represent?
|

L3
|
|
|

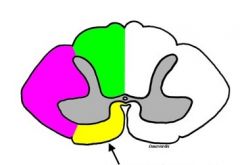
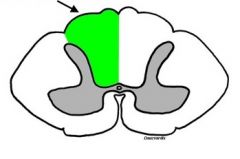
What level of the CNS does this image represent?
|

T10 (look for lateral horn)
|
|
|

What level of the CNS does this image represent?
|

Sacral (note very small amount of white matter)
|
|
|
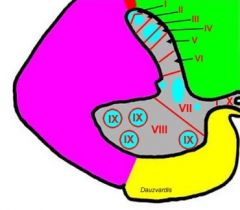
Rexed's Lamina I?
|
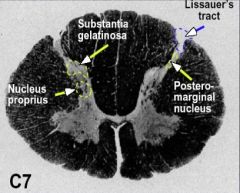
Posteromarginal Nucleus
*Present at all cord levels *Receives pain & temp inputs *Forms part of spinothalamic tract |
Posteromarginal Nucleus
|
|
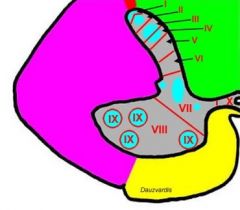
Rexed's Lamina II?
|
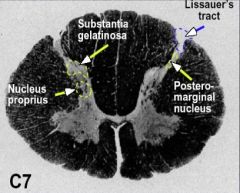
Substantia Gelatinosa
*Present at all cord levels *Receives dorsal root afferents *Filters/modifies sensory information by synapsing on dendrites of neurons in nucleus proprius *Axons ascend or descend 1-4 segments in Lissauer's Tract |
Substantia Gelatinosa
|
|
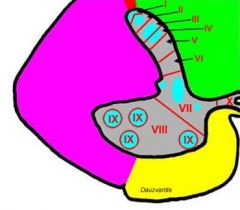
Rexed's Lamina III & IV?
|
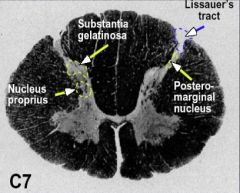
Nucleus Proprius ("Chief" or "Proper" Sensory Nucleus)
*Present at all cord levels *Receives many sensory/afferent inputs *Contains cells that project CONTRALATERALLY as part of spinothalamic tract |
|
|
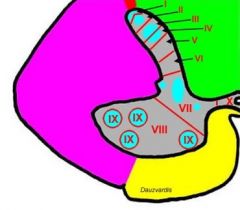
Rexed's Lamina VII?
|
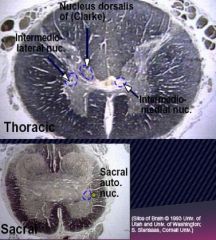
Nucleus Dorsalis (Clark's Nucleus)
*ONLY from C8-L3 *Receives muscle spindle afferents *Projects IPSILATERALLY to cerebellum as dorsal spinocerebellar tract Intermediolateral Nucleus (IML) *ONLY from T1-L3 *Origin of preganglionic cholinergic sympathetic efferents (GVE) Intermediomedial Nucleus (IMM) *All cord levels *Receives visceral afferents (GVA) Sacral Autonomic *S2-4 *Origin of cholinergic preganglionic parasympathetic efferents |
|
|
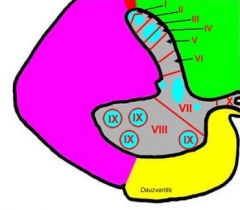
Rexed's Lamina IX?
|
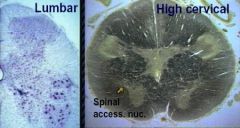
Motor neurons
*Large alpha motor neurons that innervate skeletal muscle *Gamma motor neurons that innervate muscle spindle fibers *Phrenic nucleus (innervates diaphragm) *Spinal accessory nucleus (innervates SCM & trap) *Origin of lower motor neuron pathway |
|
|
|
Caudal extent of spinal cord in newborn vs. adult?
|
Newborn: L3
Adult: L1, L2 |
|
|
|
Where is the lesion in a patient with a sensory loss corresponding to a dermatomal band just above the belly button?
|
A sensory loss over a dermatomal area often indicates a DORSAL ROOT lesion. The described sensory loss corresponds to T9.
|
|
|
|
Which meningeal layer continues as the epineurium surrounding peripheral nerves?
|
The epineurium is continuous with the spinal dura, which is a continuation of the meningeal layer of the cranial dura.
|
|
|
|
What nucleus is the upper limb equivalent of the nucleus dorsalis (of Clarke)?
|
The lateral or accessory cuneate nucleus, which gives rise to the cuneocerebellar tract, is equivalent to Clarke's nucleus.
|
|
|
|
What is the origin of sacral preganglionic parasympathetic efferents?
|
Sacral preganglionic parasympathetic efferents originate for the sacral autonomic nucleus (S2-S4).
|
|
|
|
Why is damage to high cervical spinal cord levels especially dangerous?
|
Injury at high SC levels is especially dangerous b/c of the possibility of involvement of the phrenic nucleus, which could lead to respiratory paralysis.
|
|
|
|
Identify the correct dermatomal level for the back of the head, the thumb, and the kneecap.
|
C2 = back of head
C6 = thumb L3 = kneecap |
|
|
|
Which vessels comprise the anterior circulation, and which regions of the cerebral cortex are supplied?
|
Internal Carotids
Middle Cerebral *lateral aspect of the cerebral hemisphere Anterior Cerebral *medial surface of the frontal and parietal lobes |
|
|
|
Which vessels comprise the posterior circulation, and which regions of the cerebral cortex are supplied?
|
Vertebrals
Basilar Post Cerebral *Occipital lobe and inferior temporal lobe Post Inf Cerebellar Ant Inf Cerebellar Sup Cerebellar |
|
|
|
Follow the pathway of CSF circulation from formation to return to bloodstream.
|
1. Formation in choroid plexus of ventricles (mostly in laterals)
2. Through foramina of Monro (2) to 3rd ventricle 3. To 4th ventricle via cerebral aqueduct 4. Through foramina of Lushka (2 lateral) and foramen of Magendie (1 midline) into subarachnoid space 5. Through arachnoid villi into cerebral venous sinusus and returned to venous circulation |
|
|
|
What structures form the blood-brain barrier, and what determines whether substances cross it?
|
The blood-brain barrier is formed by tight junctions between brain capillary endothelial cells. While astrocytic foot processes induce formation of tight junctions, it is the junctions themselves that form the barrier.
A substance's ability to cross the blood-brain barrier is usually determined by its lipid solubility. Some lipid insoluble substances (ie: glucose) are actively transported in, while some lipid soluble substances are actively transported out. Other substances may pass by endothelial cell pinocytosis. |
|
|
|
Name the three meninges and describe each.
|
Dura mater:
*outermost layer *comprised of outer endosteal layer and inner meningeal layer *two layers separate to form dural venous sinuses, falx cerebri b/t hemispheres, and tentorium cerebelli b/t cerebrum and cerebellum Arachnoid: *intermediate layer *lines dura with no space in between *connects to pia via extensions called arachnoid trabeculae *separated from pia by the subarachnoid space, which is filled with CSF Pia mater: *innermost layer *adheres to brain surface, following gyri and sulci *blood vessels on surface of the brain lie on top of pia |
|
|
|
What are arachnoid villi?
|
One-way valves that penetrate the dural venous sinuses and allow CSF to pass from the subarachnoid space into venous circulation
|
|
|
|
Which vessels comprise the Circle of Willis (as opposed to Ant/Post circulation)?
|
Anterior Communicating a.
Posterior Communicating a. |
|
|
|
What vessels comprise the Circle of Willis?
|
Anterior Communicating
Anterior Cerebral Internal Carotid Posterior Cerebral Posterior Communicating |
|
|
|
What mechanisms are involved in maintaining stable cerebral blood flow?
|
A constant cerebral blood flow is maintained by autoregulation: the ability of cerebral vessels to constrict or relax in response to changes in blood pressure, arterial CO2 levels, blood pH, and perivascular K+ concentration.
|
|
|
|
Describe the encapsulation, adaptation, function, and distribution of free nerve endings (as receptors).
|

Free nerve endings are:
*nonencapsulated *slow adapting *receptive to pain & temp *found in deep skin and viscera |
|
|
|
Describe the encapsulation, adaptation, function, and distribution of Merkel's Disk.
|

Merkel's Disks are:
*nonencapsulated *slow-adapting *sensitive to touch *found in epidermis: feet, hands, genitalia, and lips |
|
|
|
Describe the encapsulation, adaptation, function, and distribution of hair follicles (as receptors).
|
Hair follicles are:
*nonencapsulated *fast adapting *sensitive to touch *found anywhere there is hair |
|
|
|
Describe the encapsulation, adaptation, function, and distribution of Meissner's Corpuscles.
|

Meissner's Corpuscles are:
*encapsulated *fast-adapting *sensitive to 2-point discrimination *found in hairless skin, fingertips, joints, and ligaments |
|
|
|
Describe the encapsulation, adaptation, function, and distribution of Pacinian Corpuscles.
|
Pacinian Corpuscles are:
*encapsulated *fast adapting *sensitive to vibration, light pressure *found in fingers, toes, palms, mesenteries, and peritoneum |
|
|
|
Describe the encapsulation, adaptation, function, and distribution of the neuromuscular spindle (as a receptor).
|
Neuromuscular spindles are:
*encapsulated *slow-adapting *sensitive to muscle length (stretch) *found in muscles |
|
|
|
Describe the encapsulation, adaptation, function, and distribution of golgi tendon organs.
|
Golgi tendon organs are:
*encapsulated *slow adapting *sensitive to muscle tension *found at the muscle tendon junction |
|
|
|
Which receptors are nonencapsulated?
|
*Free nerve endings
*Hair follicle *Merkel's Disk |
|
|
|
Which receptors are encapsulated?
|
*Meissner's Corpuscle
*Pacinian Corpuscle *Neuromuscular spindle *Golgi tendon organs *Ruffini ending *Joint receptor |
|
|
|
With regards to the dorsal root afferents, how do the medial and lateral divisions differ?
|
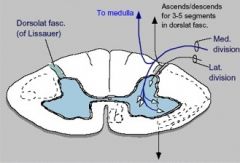
Medial:
*thick, heavily myelinated (m=medial=myelinated) *2-point touch, limb position, muscle stretch *sends collaterals to medulla Lateral: *thin, lightly myelinated (l=lateral=lightly myel.) *pain, temp, light touch, visceral afferents *asc/desc for 3-5 segments in dorslat. fasc. (Zone of Lissauer) |
|
|
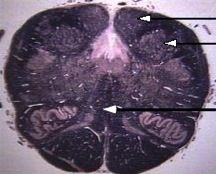
What level of the CNS does this section represent?
|
Medulla
*Note absence of "butterfly", thus not in spinal cord. *Note "fused baby feet" look (per Dr. D) *Note pyramids and inf. olivary nucleus *Arrows point to Nuc. Gracilis, Nuc. Cuneatus, and medial lemniscus (from top to bottom) |
|
|
|
What information is conveyed via the dorsal column pathway?
|
GSA:
*2 point discrimination (stereognosis) *vibration sense (tuning fork) *proprioception (position sense due to conscious perception of muscle spindle & golgi tendon receptors) |
|
|
|
Describe the Dorsal Column Pathway from start to finish.
|

*Information sensed at receptor
*Info travels along afferent fiber through DRG into Fasiculus Cuneatus (arm) or Gracilis (leg) *Fiber shoots straight up, synapsing in medulla at nucleus of same name (Nuc. Grac. or Cun.) *In medulla --> crosses midline as internal arcuate fibers *Travels upwards in medial lemniscus (white matter cord) *Second synapse in thalamus (ventral posterolateral nucleus or VPL) *Thalamus relays info to area 312 of cerebral cortex |
|
|
|
Which receptor types are involved in the dorsal column pathway?
|
*Meissner’s corpuscle for 2 point touch
*Pacinian corpuscle for vibration *Muscle spindle or golgi tendon for proprioception |
|
|
|
At what spinal cord level does fasiculus cuneatus begin?
|

Fasiculus cuneatus begins at T6. Afferents below T6 travel along the fasiculus gracilis. Above T6, both the fasiculus gracilis and fasiculus cuneatus carry fibers to the medulla.
|
|
|
|
Describe a positive Romberg sign and what it might indicate.
|

Romberg's test is a neurological test that is used to assess the dorsal columns of the spinal cord, which are essential for joint position sense (proprioception).
A positive Romberg sign occurs when the patient is able to stand steadily with feet together, but sways and breaks stance when the eyes are closed. The essential feature is that the patient is unsteadier with closed eyes than with open eyes. A positive Romberg sign indicates a problem with proprioception receptors or pathways, and could be due to a posterior column (or proprioceptive sensory nerve) lesion. |
|
|
|
A patient's MRI indicates that she has syringomyelia. If the cavity begins in the center of the cord and spreads laterally and to the right, what spinothalamic symptoms might she experience first?
|

Contralateral (left-sided) loss of pain and temperature in the upper body.
|
|