![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
101 Cards in this Set
- Front
- Back
|
Where do primary bone tumours usually occur? |
Metaphyseal area |
|
|
Where do metastatic bone tumours usually occur? |
Diaphyseal region |
|
|
Where do benign bone diseases usually occur? |
Anywhere |
|
|
Features of aggressive/malignant bone tumours |
Moth eaten or permeative appearance Poorly defined/ indistinct borders Cortical disruption (cortex not seen, thinned) Spiculated periosteal new bone formation Rapid rate of change Soft tissue mass |
|
|
Features of non-aggressive/benign bone tumours |
Localised area of lysis Well demarcated Short transition zone Smooth periosteal reaction Slow change Lack of soft tissue mass |
|
|
Aggressive 1° bone tumour osteosarcoma lymphoma haemangiosarcoma -changes in bone opacity - spiculated periosteal reaction |
|

|
Aggressive 1° bone tumour osteosarcoma - spreading - long transition zone - periosteal bone formation and destruction |
|

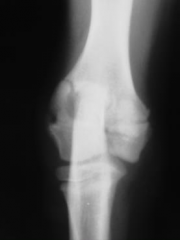
4yo dog |
Benign bone cyst - large area of radiolucency |
|
|
How do you tell the difference between a bone tumour and a bone infection? |
Both aggressive Look at signalment, history, physical findings - recent surgery, wound - chronic infection |
|
|
Causes of Fractures |
Trauma from external force Trauma from internal force - avulsions, eg biceps on supraglenoid Normal activity on diseased bone - pathological |
|

|
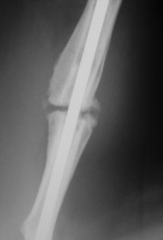
Long oblique fracture Periosteal new bone Change in bone opacities = Pathological frature Metastatic cancer |
|

|
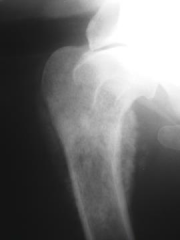
Fracture almost vertical down proximal humerus Periosteal new bone formation Changes in bone opacity = Pathological fracture Aggressive 1° bone tumour |
|

|
Epiphyseal avulsion bony remodelling |
|
|
Complications of fracture healing |
Malunion - abnormal position Delayed union - slow. Infection, instability Non-union - no evidence of healing. hypertrophic, atrophic Osteomyelitis Osteoporosis - weakening, incorrect use Joint complications Fracture induced sarcomas - rare, more likely with metal implants |
|

|
Atrophic non-union |
|
|
Hypertrophic non-union - new bone cant breach the gap - rotational instability - need to make more stable - may want to scarify to stimulate bone formation |
|
|
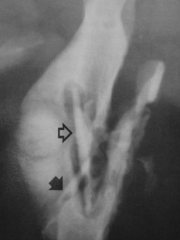
Sequestrum Fracture with infection Large pieces of bone within a pus filled cavity Need to go in and take sequestrum out Common in cows |
|
|
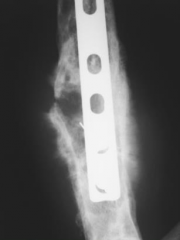
Post-fracture sarcoma Initially doing okay, leg swells Areas of radiolucency Spiculated bone Plate may be an irritant |
|
|
Degenerative joint disease Roughening of articular faces Altered thickness of joint space Subchondral bone changes Mineralisation of joint soft tissues Intra-articular calcified bodies Joint malformation |
|
|
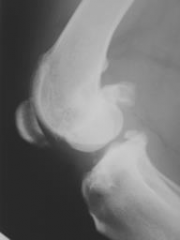
Degenerative joint disease Joint effusion - radio-opacity where fat pad should be (Cr to joint) |
|
|
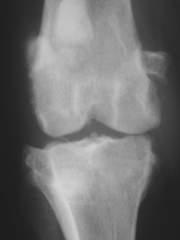
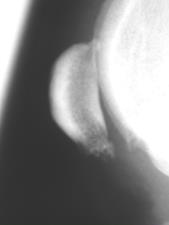
Degenerative joint disease Osteophyte formation on distal patella
|
|
|
Degenerative joint disease Joint effusion Osteophyte formation Enthesiophyte formation on tibial tuberosity |
|
|
Osteoarthritis |
DJD Weight-bearing joints Medium-large breeds 2° to developmental disorders or acquired |
|
|
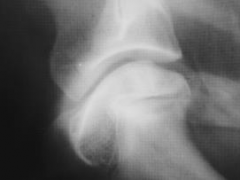
Pathological fracture Incomplete ossification of humeral condyles Physes not fused when they should have Fracture up the bone from the joint and across the condyle |
|
|
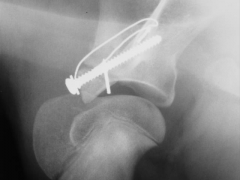
Reattachment of supraglenoid tubercle after avulsion fracture |
|
|
Osteochondrosis Joint surfaces should be smooth but are bumpy on the right |
|
|
Osteochondrosis Medial acpect (R) of humeral head - Not uncommon in this region |
|

|
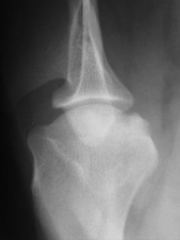
Osteochondrosis Concavity at the medial condyle |
|

|
Premature closing of the distal growth plate of the Ulna - radius continues to grow = bowed |
|
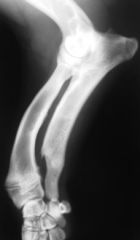
|
Premature closing of the distal growth plate of the Ulna - radius continues to grow = bowed - valgus deformity - humerus forced proximally (UAP) - elbow DJD |
|

|
Premature distal radial growth plate closure - shortened radius - ↑ humeroradial joint space - subluxation of semilunar notch - humerus gets pushed dowm - elbow DJD |
|

|
Retained cartilagenous core - radiolucency |
|

|
Elbow dysplasia Osteophytes along non-articular border of anconeal process Osteophytes on lateral epicondylar ridge Sclerosis of trochlear notch Displaced FCP |
|

|
Hip dysplasia Acute angle of hip Shallow acetabulum Opacity differences in bone Periosteal new bone |
|

|
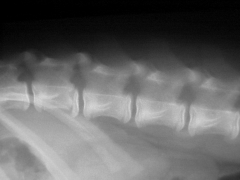
Panosteitis Radio-opacities in medulla of both bones |
|

|
Panosteitis Radio-opacities in medulla of both bones Pathological fractures due to bone brittleness |
|

|
Hypertrophic osteodystrophy Radiolucent areas New bone formationon both bones |
|

|
Nutritional secondary hyperparathyroidism Osteopenia - ↓ bone density, thin cortices Multiple pathological fractures |
|

|
Normal tympanic bullae Air filled thin walled (only 75% of dogs with otitis media show radiograph signs) |
|
|
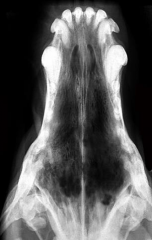
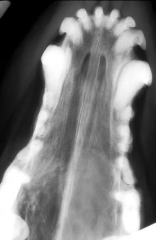
Destructive rhinitis Aspergillus fumigatus Turbinates destroyed, nasal discharge, bleeding |
|
|
Destructive rhinitis Aspergillus fumigatus Turbinates destroyed, nasal discharge, bleeding |
|

|
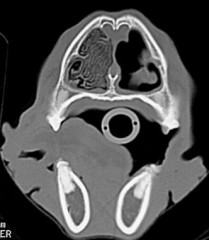
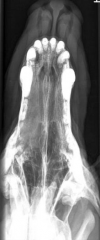
Feline nasal tumour Radio-opacity may be fluid or soft tissue mass Destruction of turbinates Bleeding nose, nasal discharge |
|

|
Malignant nasal tumour Soft tissue opacity Line definition - mass |
|
|
Malignant nasal tumour Soft tissue opacity May be destruction of turbinates |
|
|
Turbinate destruction Soft tissue opacity |
|
|
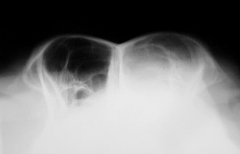
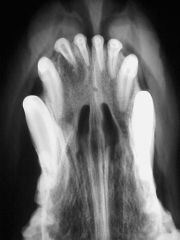
Aggressive nasal tumour Erosion of vomer bone (nasal septum) Soft tissue opacity |
|
|
Nasal tumour Periosteal bone formation May grow outward externally or through ethmoid turbinates into brain |
|

|
Mandibular fractures Near temporomandibular joint and in rostral third |
|
|
Tooth root abscess Must remove tooth |
|

|
Tooth root abscess Tooth removed |
|
|
Oral cavity neoplasias |
Fibromatous/ossifying epulis - dog, benign, no bone involvement Cats - 70% SCC Dogs - Malignant melanoma, SCC, fibrosarcoma, osteosarcoma 60-70% malignant tumours show bone involvement |
|

|
Giant cell granuloma Displacement of teeth Multiple radio-opacities - may be bone involvement |
|
|
Odontogenic malignant neoplasms |

Tumour of tooth Rare, young animals Usually lytic, expansile with regular and well defined margins Commonly contain mineral opacities |
|

|
Ameloblastoma May affect one or more teeth May appear solid or cystic Expansile with bone destruction common Usually soft tissue mass |
|
|
Malignant non-odontogenic neoplasms |

Most originate from soft tissue (gingiva, palate) or from mandibular or maxillary bones (carcinomas, FSA, MM, acanthomatous epuils = basal cell carcinoma) |
|

|
Fibrosarcoma |
|
|
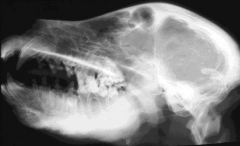
Craniomandibular osteopathy |

Benign self limiting periosteal proliferation Terriers most commonly affected WHWT : recessive autosomal transmission Clinical signs at 3-8 months Periosteal reaction usually stops at maturity |
|
|
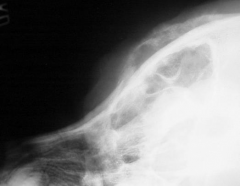
Craniomandibular osteopathy Thickening of cranial and mandibular cortices |
|

|
Cranial hyperostosis Similar to craniomandibular osteopathy but only frontal bones Thickening of cortex Keeps getting bigger May be uncomfortable |
|
|
Otitis media/interna |

Opacity in tympanic bullae Bone reaction - thickening of wall, sclerosis, osteolysis +/ periosteal reaction Expansion of bullae (less common) Sclerosis of petrous bone |
|

|
Otitis media Right bulla sclerotic, filled |
|

|
Otitis media Bone reaction - thickening of wall, sclerosis, osteolysis +/ periosteal reaction (Cats have two compartments to bullae) |
|

|
Normal changes Symmetrical sclerosis in petrous bone in old animals Symmetrical thickening of bullae Especially cats |
|
|
Primary bone tumours |
Similar to appendicular tumours Osteosarcoma most common - usually osteoblastic with irregular and ill-defined periosteal reaction Osteoma most common benign - smooth, well defined margin, sclerotic Multilobular oteochondroma Chondrosarcoma Fibrosarcoma |
|

|
1° bone tumour Chondrosarcoma Aggressive Marked soft tissue swelling Periosteal new bone |
|
|
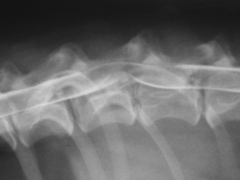
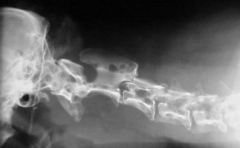
Physeal fracture of body of vertebra Lumbar spine Kicked displacement of caudal physis of second vertebra in |
|

|
Normal narrowing of disk space occurring between anticlinal vertebrae (T10 and T11) (Centred) |
|
|
Diaphragmatic crus attachment at L3 and L4 may get some bony remodelling at this position due to the attachment of the diaphragm |
|

|
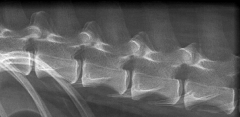
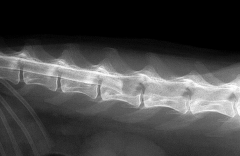
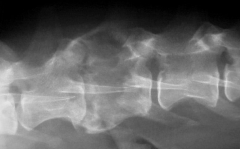
Spondylosis deformans New bone formation at bottom ends of vertebrae Degenerative wear and tear Normal in older animals May fuse No clinical signs (may make back stiff) |
|

|
Spondylosis deformans |
|
|
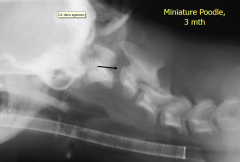
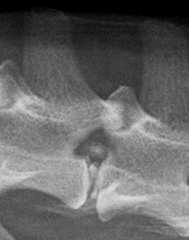
Agenesis of dens Huge gap between C1 and C2 Weak spot Luxation of C2 |
|

|
Atlantoaxial subluxation Atlantoaxial ligament deficient/absent When head moves, C1 moves but C2 does not - causes bend in spinal cord = painful Gap between dens and atlas too great |
|
|
Spinal cord compression |
|

|
Spinal cord compression |
|
|
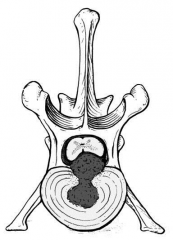
Hansen type 1 disc hernia |
|
|
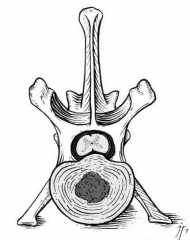
Hansen type 2 disc hernia |
|
|
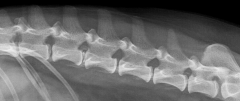
Disc mineralisation and herniation Mineralisation normal degeneration - loss of elasticity = herniation |
|
|
Disc mineralisation and herniation Mineralisation normal degeneration - loss of elasticity = herniation |
|

|
Disc mineralisation without herniation Mineralisation normal degeneration - loss of elasticity = herniation |
|
|
Spinal cord tumour Blockage of CSF so myelin cant move past |
|
|
Discospondylitis |
Infection of intervertebral disc and secondarily of adjacent endplates L7-S1 most commonly affected Large breed, male, mid age most common, rarely cats |
|
|
Discospondylitis - causes |
Haematogenous spread - Staph intermedius, Strep spp, E. coli Direct infection - penetrating wound, migrating FB Post-op complication |
|
|
Discospondylitis Infection of intervertebral disc and 2° of adjacent endplates |
|
|
Discospondylitis Infection of intervertebral disc and 2° of adjacent endplates |
|

|
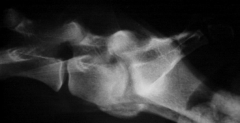
Discospondylitis Infection of intervertebral disc and 2° of adjacent endplates Common site Requires long period of antibiotic therapy |
|
|
Malignant 1° bone tumours |
Osteosarcoma Chondrosarcoma Fibrosarcoma Haemandiosarcoma Lymphoma etc. |
|

|
Spinal chondrosarcoma |
|
|
C2 mass Radiolucency Compression of spinal cord |
|
|
C2 mass Radiolucency Compression of spinal cord |
|
|
Bone metastasis to axial skeleton |
Carcinoma of the prostate, bladder, urethra, mammary gland, anal sac Appendicular OSA Multiple myeloma, lymphoma, malignant histiocytosis, HSA |
|

|
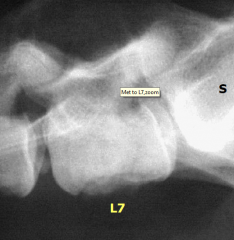
Metastasis from prostatic carcinoma Tumours in caudal abdomen Spondylitis of last vertebral body - direct metastatic spread |
|
|
Metastasis from prostatic carcinoma Tumours in caudal abdomen Spondylitis of last vertebral body - direct metastatic spread |
|
|
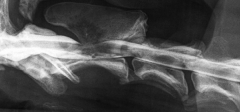
Malignant histiocytosis Lysis of bone Spondylosis (degenerative) |
|
|
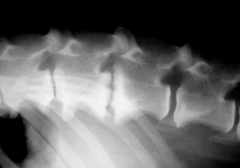
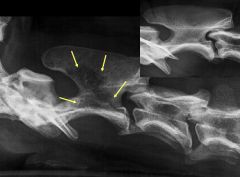
Multiple myeloma Swiss cheese appearance in multiple vertebral bodies - virtually pathognomonic |
|

|
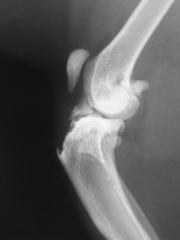
Partial tear ~1 month ago Joint effusion (loss of fat pad) Osteophytes |
|

|
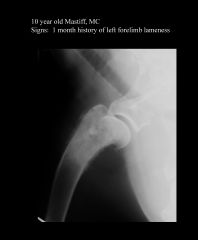
Hip dysplasia on left, Subluxation |
|

|
Pathological fracture - 1° bone tumour Moth eaten periosteal reaction Distal metaphyseal Horizontal, partially comminuted complete fracture Soft tissue swelling |
|

|
Hypertrophic metaphyseal lysis |
|
|
1° bone tumour Metaphyseal region Radio-opacity |
|

|
Right sided nasal carcinoma Opacity on right side Lysis of facial bone |
|

|
Migrating grass awn No bone destruction so not tumour Osteomyelitis Grass awn moves from lungs → pleural space → upper reach of pleural space (diaphragm attachment) where it irritates vertebral bodies |