![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
47 Cards in this Set
- Front
- Back
|
functions of the kidney |
regulation of body fluid osmolality + volumes, regulation of electrolyte balance (Na+, K+, Pi, Ca2+, Mg2+, HCO3-, Cl-; regulation of acid base balance, excretion of metabolic wastes, and foreign substances (urea, uric acid, creatinine, drugs), production of hormones (renin, erythropoietin, calcitriol) |
|
|
fluid compartments |

intracellular fluid is 40% of body weight; extracellular fluid is 20% body weight 3/4 of the extracellular is the interstitial, and 1/4 of the extracellular is the plasma the more muscular an individual is the greater the percentage of body water; increases in fat reduce total body water; women have a layer of subcutaneous fat, that reduces their pertanged of total body water to about 50-55%, infants have high water content (70%) & the elderly have lower water content |
|
|
osmolarity |
number of particles / volume of solution |
|
|
tonicity |
behavior property of the cell (shape change) |
|
|
volume and osmolarity disturbances |
rule 1: ECF (osm vol) is always distributed first rule 2: start with equal osmolarity, end with equal osmolarity
the basic principle governing water movement between the ECF and the ICF is that the osmolality of each must be equal, if not water moves to equalize the osmolality
disturbances are represented by Dannet-Yarrow diagrams |
|
|
hypotonic expansion |
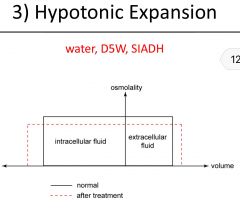
water typically water is not given in IV, because the osmolality of the plasma is lowered causing cells to swell and bust D5W isotonic glucose (5g/100ml) intravenously administered is osmotically equivalent to drinking water; ingested water enter ECF increasing the volume, and decreasing ECF osmolality, water then enters cells via osmosis
SIADH(syndrome of inappropriate ADH release) ADH release is unregulated causing water retention in the body results in ECF fluid increases and decreases ICF osmolality |
|
|
isotonic expansion |
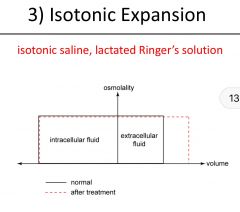
isotonic saline (0.9% NaCl ~300 mOsm/kg) or lactated ringer's solution (contains Na+, Cl-, K, Ca2+, HCO3-) both solutions contain the same osmolality as plasma, ringer's is more similar to ECF than isotonic saline results in ECF fluid volume increases, does not change ECF osmolality, therefore ICF volume and osmolality does not change |
|
|
hypertonic expansion |
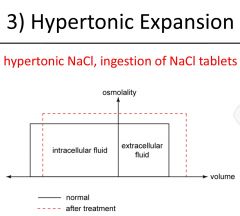
hypertonic saline IV cause both the ECF volume and osmolality to increase, the latter will cause water to leave the osmosis, thereby decreasing ICF and increasing ICF osmolality ingestion of NaCl tablet initially increases ECF osmolality but not ECF volume and an increase in ICF osmolality, ultimately will increase ECF volume |
|
|
hypotonic contraction |
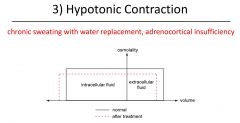
sodium chloride depletion sweat is a hypotonic NaCl solution, depletion results in low plasma NaCl concentration will decrease ECF osmolality which reduces ADH causing increased excretion of dilute urine; only way to fix this is to restore salt levels, the decrease in ECF osmolality causes water to enter cells increasing ICF volume reducing ICF osmolality adrenocortical insufficiency the hormone aldosterone is not produced causing a lack of NaCl retention and increased elimination of NaCl via urine |
|
|
isotonic contraction |
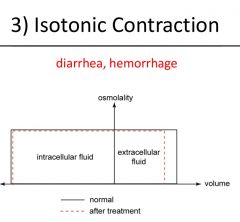
diarrhea fluid loss is isotonic→ no change in osmolality but ECF volume decreases→ no osmotic gradient is generated across the cell membrane and no net net water movement occurs→ ICF volume and osmolality is therefore unchanged hemorrhage whole blood is lost during hemorrhage without affecting the osmolality of ECF and ICF, there is no change in ICF volume, ECF volume decreases due to plasma loss results in ECF volume decrease |
|
|
hypertonic contraction
|
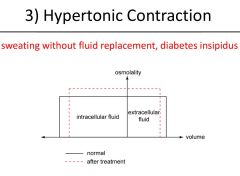
sweat without fluid replacement sweat is hypotonic (dilute NaCl solution) ICF volume decreases and osmolality increases diabetes insipidus excessive production of dilute urine and excessive thirst due to decreased production of ADH at the level of the brain or insensitivity of ADH at the level of kidneys result ECF volume decreases |
|
|
urinary system |
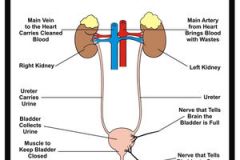
composed of kidneys ureters bladder and urethra, each kidney has a million nephrons which filter the blood |
|
|
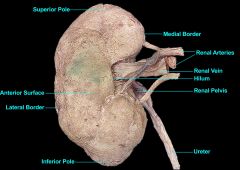
kidney surface anatomy |
|
|
|
nephron structure |
superficial or mid-cortical nephrons are 85% these nephrons do not have a thin ascending limb of the loop of Henle, juxtamedullary nephrons are 15% which are found deep within the medulla and are used to build the medullary osmotic gradient |
|
|
bowman's capsule |
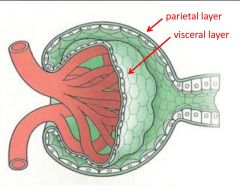
glomerulus aka bowman's capsule, is doubled walled, parietal layer is made epithelial cells no involved in filtration; visceral layer is made of specialized epithelial cells called podocytes that wrap around the glomerular capillaries, podocytes form filtration slits |
|
|
glomerular basement membrane |
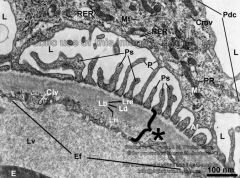
endothelial layer of the glomerular capillaries are fenestrated with pores that are much larger than other capillaries, blood solutes pass thru the slits of the podocytes excluding the proteins, basement membrane has a negative (-) charge, ultrafiltrate (isotonic) enters the bowman's space which the space between the parietal and visceral layers of the bowman's capsule |
|
|
flow in the kidney |
renal arteries → interlobar artery → arcuate arteries → interlobular arteries → afferent arterioles→glomerular capillaries → efferent arterioles (portal vessels) → vasa recta (branches off the efferent arterioles of the juxtaglomerular and connect again with the venule) or peritubular capillaries (branch off the efferent arterioles of the superficial or mid cortical nephrons) |
|
|
cells of kidney |
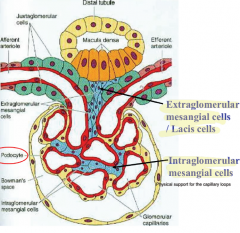
macula densa found where the macula densa is found where the thick ascending limb of the loop of henle meets the distal convoluted tubule, juxtaglomerular apparatus (JGA) found in the walls of the afferent arteriole and some in the afferent arteriole and some in efferent arteriole, synthesize renin; extraglomerular mesangial cells modified smooth muscle cells that play a role in autoregulation of blood flow
intraglomerular mesangial cells, found among the glomerular capillaries and may regular blow and hence GFR, and may have phagocytic role |
|
|
the fates of the solutes which pass the basement membrane |
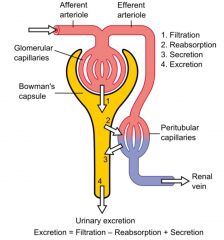
filtration is the movement of ultrafiltrate of plasma into Bowman's space (1 liter a minute); reabsorption is the movement of water solutes from the tubules to peritubular capillaries; secretion is the movement of water and solutes from the peritubular fluid to the tubules; excretion is the removal of substances from the body in (1 -1.5 liters a day) filtration = filtration - absorption + secretion |
|
|
Tubular Transport |

transcellular transport: the transport of solutes through a cell, may be passive or active paracellular transport is always passive and involves the passage of solutes via the tight junction; always prevents the lateral movement of integral proteins; divide the cell into luminal and basolateral domains |
|
|
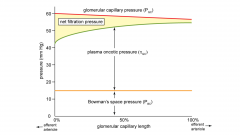
Glomerular filtration rate (GFR) |
GFR = Kf x Pf Pf= (Pg- Pb) - (πg - πb) rate at which substances move from glomerular capillary blood into Bowman's space; filtration barrier has a negative surface prevents large blood proteins (albumin) from crossing; two factors: the balance of starling forcing (Pf net filtration pressure NFP) filtration coefficient (Kf a combination of glomerular permeability and filtration area)
|
|
|
filtration fraction |
GFR divided by RPF (renal plasma flow) ~20 percent |
|
|
resistance & GFR + Renal blood flow |
GFR is controlled by Pgc, which is modulated by blood pressure & afferent + efferent resistance; neural & hormonal input affects afferent + efferent arterioles increase afferent arteriole resistance ⇒ decrease in GFR due to a fall in Pgc; FF does not change GFR and RPF fall together increase efferent arteriole resistance ⇒ increases FF because GFR rises (due to an increase in Pgc) and RPF falls; increased FF increases πgc |
|
|
kidney autoregulation |
GFR and RPF remain relatively constant over a range of MAP's; normal MAP is about 93 mmHg |
|
|
myogenic response |
rapid protection of glomeruli from short term fluctuations in blood pressure; lead to the constriction of afferent arteriole smooth muscle ⇒ minimal ↑ renal blood flow & ↑ GFR ↑ MAP ⇒ ↑afferent arteriole stretch ⇒mechanically gated Na+ & K+ channels open ⇒Na+ influx and K+ efflux ⇒ depolarization ⇒ voltage gated Ca2+ channels open ⇒Ca2+ influx, binds to calmodulin activates MLCK ⇒muscle contracts |
|
|
tubuloglomerular feedback |
may occur up in up to a minute to help maintain an appropriate filtered load of solutes; an increase in MAP causes an increased GFR therefore an increase in Na+ and Cl- delivery to the macula densa, which causes an increase in ATP (P2) release and adenosine (A1) release; A1 & P2 stimulation causes a rise in Ca2+ levels in extraglomerular mesangial cells which increases Ca2+ in juxtaglomerular cells(secret renin) & in the afferent arteriole smooth muscle (vasoconstriction) lead to the constriction of afferent arteriole smooth muscle ⇒ minimal ↑ renal blood flow & ↑ GFR |
|
|
sympathetic nervous system stimulation of kidney |
when MAP falls below 85 mmHg, autoregulation ceases and the sympathetic nervous system overrides it; constricts both the afferent and efferent arterioles to decrease RPF but produces no change in Pgc, therefore the filtration fraction increases severe sympathetic nervous system activity causes a reduction in Pgc and RPF, acute renal failure may result after 10 days hyperkalemia may result and subsequent death |
|
|
Atrial (ANP) & brain (BNP) natriuretic peptides |
are released when blood pressure is high (increased vascular volume)
cause decreased Na+ reabsorption in the deep medullary convoluted tubule; afferent arteriole dilation and efferent arteriole constriction inhibit renin, aldosterone, and ADH release overall there is an increase in Pgc, GFR, Na+ excretion (helps bring water volume down), & RPF |
|
|
Clearance |
volume of blood cleared of the substance and excreted into urine per unit time Cx=(Ux X V) / Px if a substance is reabsorbed and not secreted it's clearance equals zero (eg glucose) if a substance is slightly reabsorbed clearance of this substance is less than GFR and RPF if the kidney removes all of a substance from the blood in one pass through the kidney, the volume of plasma cleared equals RPF; if secreted the clearance will be greater than GFR, and if the substance is only filtered clearance equals GFR |
|
|
Inulin |
freely filtered, not reabsorbed or secreted; amount of inulin filtered equals the amount of inulin excreted, rarely used to calculate GFR |
|
|
Creatinine |
freely filtered not reabsorbed, slightly secreted in the proximal convoluted tubule, clearance is greater than GFR, less than RPF, indicator of renal function; with progressive renal failure GFR decreases and serum creatinine increases: GFR gets halved so the serum creatinine doubles, inverse relationship |
|
|
Para-amino hippuric (PAH) |
is freely filtered and not reabsorbed, but is secreted into the PCT; clearance of PAH becomes the renal plasma flow |
|
|
carrier mediated reabsorption or secretion |
limited by the transport maximum (Tm); glucose is an example |
|
|
Na+ Filtration and Reabsorption |
Na+ is freely filtered at the glomerulus, almost entirely (99.5) reabsorbed and not secreted; largely occurs at the PCT, ascending Loop of Henle, early Distal Collecting, and the CT. Na+ is reabsorbed on the apical (luminal) side of the tubular epithelium down its concentration gradient and against the concentration gradient via the Na+/K+ pump on the basolateral side |
|
|
Na+ at the proximal convoluted tubule (PCT) |

Na+ reabsorption begins on the luminal membrane via secondary active transporters; diffuses down its concentration gradient to drive Tm dependent substances (glucose, amino acids, lactate, & HPO4 + H2O {keeps tonicity}) against their concentration gradients;the concentration gradient is established on the basolateral membrane via Na+/K+ pump; hydrogen is transported out via secondary active antiport stimulated by hormone angiotensin II |
|
|
Na+ at the Thick ascending Loop of Henle |
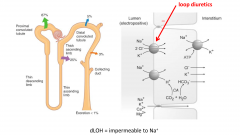
Na+ reabsorption occurs via a Na+/H+ antiporter; Na+/K+/2Cl- symporter on the luminal membrane; moves down it's concentration gradient from tubular lumen to tubular epithelium, which allows secondary active H+ Cl- & K+; concentration gradient is due to Na+/K+ pump on basolateral membrane (became hypertonic at the lowest point between ascending and descending; which then loses it's salt and contains it's water and becomes hypotonic) |
|
|
Loop Diuretics |
inhibits the Na+/K+/2Cl- symporter preventing water reabsorption in the ascending loop of henle due to osmosis; there are potassium leak channels on both luminal and basolateral membranes; produces more urine, water remains un-reabsorbed because the salt wasn't removed at the thick ascending loop of Henle; glucose acts as an osmotic particle as well resulting in increasing urine production as well |
|
|
Na+ at the Distal Convoluted Tubule |
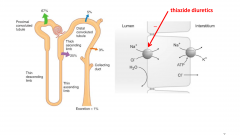
Na+ reabsorption occurs via a Na+/Cl- symporter that transports Na+ across the basolateral membrane; water does not follow (diluting) |
|
|
Thiazide-like Diuretics |
inhibits the Na+/Cl- symporter stimulating the renin-angiotensin-aldosterone system |
|
|
Na+ at the Convoluted Tubule (& late dct) |

the action of aldosterone (principle cells), will allow Na+ reabsorption stimulating luminal Na+ channels and basolateral Na+/K+ pumps, also increases K+ secretion into the tubular fluid by stimulating luminal K+ channels; water permeability is dependent on ADH |
|
|
Potassium Sparing Diuretics |
blocks Na+ channels or block aldosterone receptor; indirectly inhibits K+ secretion and excretion; generally used in combination with loop & thiazide-like diuretics |
|
|
RAAS pathway (renin angiotensin aldosterone system) |
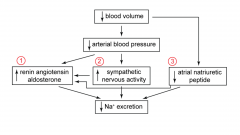
blood volume or pressure decreases, RAAS pathway is activated, sympathetic is stimulated, ANP levels decrease |
|
|
Renin |
released from the juxtaglomerular cells & part of RAAS pathway; release is stimulated by decreased stretch of afferent arterioles (low blood pressure or volume); decreased Na+ and Cl- delivery to macula densa (due to decrease filtration); hydrolyzes angiotensin (produced in the liver) to angiotensin I; which is converted to angiotensin II by angiotensin converting enzyme |
|
|
Angiotensin II (ang II) |
actions binds to g-protein linked receptor on smooth muscle activating phospholipase C is activated cleaving PIP2 into IP3 and DAG; IP3 binds to its receptor on the endoplasmic reticulum to cause the release of Ca2+ into the cytoplasm leading to smooth muscle contraction; stimulates H+ ATPase activity of a-intercalated cells in the CT, increases K+ secretion by stimulating the activity of luminal K+ channels of the principal cells in the CT, increasing Na+ reabsorption by stimulating the activity of luminal Na+ channels and basolateral Na+/K+ pumps on the principle cells of the CT effects increases blood pressure (vasoconstriction of peripheral vessels) thirst sensation desire to consume salt, increases aldosterone (zona glomerulosa adrenal cortex) & ADH (posterior pituitary) release, increases activity of the Na+/H+ antiporter in the PCT and TAL, decreases GFR and resists renal blood flow; causes the desire to drink water |
|
|
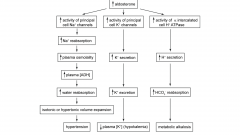
aldosterone |
aldosterone may be stimulated by increased plasma K+ levels and decreased ANP or BNP; increasing Na+ reabsorption stimulating luminal Na+ channels and basolateral Na+/K+ pumps in the CT, increasing K+ secretion by stimulating luminal K+ channels in the CT, stimulating H+ ATPase activity of a-intercalated cells in the CT |
|
|
regulation of Na+ excretion sympathetic nervous system |
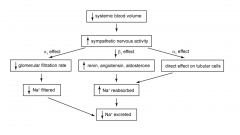
a1 receptor activation: vasoconstriction of afferent and efferent arterioles decreases, and Na+ reabsorption in the PCT, decreasing in GFR and Na+ filtration b1 receptor activation: renin release from the juxtaglomerular cells Na+ reabsorption is increased |
|
|
Conn's Syndrome |
hyperaldosteronism, aldosterone producing adenoma, high concentrations of circulating aldosterone, increased Na+ reabsorption (⇒ hypertension), increased ADH release, increased K+ and secretion leads to hypokalemia, increased H+ ATPase activity increases H+ secretion and HCO3- reabsorption leading in to metabolic alkalosis |