![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
459 Cards in this Set
- Front
- Back
|
What are the normal renal changes expected in pregnancy? |
Increased RBF, size (1->1.5cm), volume (30%), GFR, Na+, K+ and water rentention |
|
|
What is the feedback effect of low plasma oestrogen concentration? |
No feedback effect, increased GnRH leading to increased FSH and LH and increased oestrogen |
|
|
What is Patau's Syndrome? |
Trisomy 13 - 1:10000 live births, 80% die in first year. Diagnosed by amniocentesis |
|
|
What is the relative potency of Estriol (E3)? |
10% |
|
|
What are the main effects of oestrogen? |
Breast development, uterus and external female sex organs, skeletal changes, skin changes, metabolic rate and fat deposition, sexual behaviour |
|
|
What does the connecting stalk (attached to the secondary yolk sac) eventually become? |
Umbilical cord |
|
|
What is the amnion? |
Single layer of extraembryonic ectoderm lined with extraembryonic mesoderm - fluid surrounds embryo |
|
|
What mechanism prevents myometrial contractions before labour? |
cAMP --> PKA --> phosphorylates and inhibits MLCK. |
|
|
What controls foetal glucose levels? |
Maternal glucose (no hormones) |
|
|
When does the ductus venosus shut? |
Between 3 and 7 days |
|
|
What is the relative potency of β-Oestradiol (E2)? |
100% |
|
|
What is the relative potency of Estrone (E1)? |
1% |
|
|
What two layers make up the bilaminar disc (formed day 12)? |
Epiblast, hypoblast |
|
|
What is the chorion? |
Layer of trophoblast and extraembryonic mesoderm surrounding embryo |
|
|
Which hormonal/ chemical factors prevent myometrial contractions before labour? |
Progesterone (reduces number of gap junctions and PGF2 synthesis), Prostacyclin (PGI2), NO, relaxin |
|
|
How do glycogen stores in the foetal liver compare with that of an adult? |
Generally low. Low iron content (higher absorption) |
|
|
What is the function of the SRY gene? |
Binds to DNA and distorts its shape, thereby regulating genes that control the development of the testes |
|
|
What happens to most embryos that form from errors in meiosis? |
Spontaneously abort |
|
|
After ovulation, the luteal phase lasts 12-15 days. Which hormones do this phase depend on and which are secreted? |
Dependent on FSH and LH Secrete progesterone and oestrogen |
|
|
What is the most important form of progestin? |
17-α-hydroxyprogesterone |
|
|
What are the problems associated with a cervical ectopic pregnancy? |
Can cause severe haemorrhage of mesentery or placenta (placenta praevia - obstructs cervix) |
|
|
What are the main features of the chorion? |
Villi (1o, 2o, 3o) protrude from chorionic plate. Eventually forms placenta (foetal component) |
|
|
What cervical changes (ripening) prelude the onset of labour? |
Increased softening and distensibility, effacement (shortnening) and early dilatation |
|
|
What % of foetal body weight is fat at term? |
15% - lower in preterm babies |
|
|
What are examples of common puerperal complications? |
Perineum, micturition, bowel problems, mastitis, backache, psychological |
|
|
What is a non-disjunction error in meiosis? |
Failure of homologous chromosomes or chromatids to separate |
|
|
Pre-ovulatory follicles survive for approximately 37 hours. What hormones are they dependent on and what do they secrete? |
Dependent on LH surge Secrete large amount of oestrogen |
|
|
What are the main effects of progesterone? |
Secretory changes in uterine endometrium, increased secretions of fallopian tube wall, stimulates breasts and ducts within to grow |
|
|
What are the features of a tubal ectopic pregnancy? |
Associated with endometriosis and pelvic inflammatory disease, mostly in ampulla, can also be isthmic, fimbrial |
|
|
What are the common tests during pregnancy for abnormalities? |
Chorionic villi biopsy - 9-12 weeks, immediate response, can ofer early termination. Amniocentesis - 15-19 weeks, delay in results, can offer late termination |
|
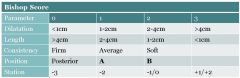
What position is the cervix in at bishop score 2 (label B on table)? |
Anterior |
|
|
Why aren't lipids directly transported to the foetus? |
Insoluble - transported as FAs bound to albumin/ lipoproteins |
|
|
What are postnatal blues? |
Emotional lability, tearfulness, sadness in 50% of women 3-5 days post birth. Requires reassurance and support |
|
|
What happens during the Diakinesis ('moving through') stage of prophase I? |
4 points of tetrads visible, chiasmata entangle, overlap. Closely resembles mitotic prometaphase, nuclear membrane disintegrates into vesicles, mitotic spindle starts to form |
|
|
Antral follicles live for 8-14 days. What hormones are they dependent on and what do they secrete? |
Dependent on FSH and LH, secrete oestrogen |
|
|
What is the two cell theory of steroidogenesis? |
Theca cells secrete testosterone and androstenedione in response to LH. Granulosa cells release aromatase in response to FSH which converts these into oestrogen |
|
|
What are the locations for ectopic pregnancy? |
Tubal (most common), ovarian, abdominal, cervical (all rarer) |
|
|
Where does implantation normally occur? |
Posterior wall of the uterine cavity |
|
|
What are the main prostaglandins that affect the cervix? |
PGE2, PGI2, PGF2a. PGE2 plays major role. Often used in obstetrics to induce labour |
|
|
Why aren't lipids used much by the foetus as a substrate for oxidative metabolism? |
Move slowly across the membrane |
|
|
What is postnatal depression? |
Anhedonia, worthlessness and guilt, lack of cern for self and baby during the first postnatal year. Affects 10-15% women. Requires counselling, antidepressants or psychotherapy |
|
|
What happens during the Diplotene ('two threads') stage of prophase I? |
Homologous chromosomes separate a little, uncoil to allow DNA transcription. Lightly bound at chiasma until severed at anaphase I. Oocytes develop at this stage, arrest before birth |
|
|
Primordial follicles survive for just under 50 years. Pre-antral follicles survive for 85 days (2-3 cycles). Are they dependent on hormones? |
They are independent of hormones |
|
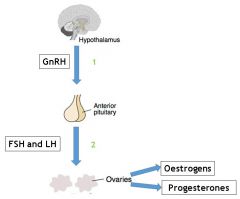
What type of feedback is taking place at labels 1 and 2 on this image of the Hypothalamic-Pituitary-Ovarian axis? |
Positive |
|
|
How is implantation completed (days 9-12)? |
Formation of extraembryonic mesoderm, uterine lining repaired, interstitial implantation (embryo below lining), maternal blood begins to flow through lacunae |
|
|
When does the bilaminar disc become the trilaminar embryo and what is this process called? |
3rd week - gastrulation |
|
|
What is the effect of oestrogen on the cervix? |
Induction of prostaglandin synthesis |
|
|
What are the three sources of amino acids for the foetus and how do levels in the foetus compare to that in the mother? |
Maternal, placental, foetal sources. Levels higher in the foetus |
|
|
What is postnatal psychosis? |
Denial of pregnancy/ baby, delusions, hallucinations starting 3-7 days post birth. Affects 1 in 1000 births, requires hospitalisation, ECT, lithium, anti-psychotics |
|
|
What happens during the Pachytene ('thick threads') stage of prophase I? |
Tetrad of chromosomes forms, known as bivalent. Crossing over occurs, no gaps. Sex chromosomes exchange only over small region. Chiasmata forms at points of crossing over |
|
|
In relation to ovulation, when are oestrogen and progesterone dominant? |
Oestrogen before, progesterone after |
|
|
What is GnRH in terms of protein and how is it released? |
Decapeptide, short pulses every ~90 minutes from arcuate nucleus of hypothalamus |
|
|
What is the decidual reaction (day 8)? |
Endometrium becomes decidua for nutritional support, restricts invasion. Prevents maternal immune response against foetus |
|
|
How is the primitive streak formed? |
Disc elongates at day 13 due to bilateral symmetry |
|
|
What are the effects of inflammatory mediators on the cervix? |
Accumulation of neutrophils and macrophages in stroma - release of pro-inflammatory cytokines (IL-1β, IL-6, IL-8, TNF) promotes cervical ripening |
|
|
How does the foetus receive immunological protection? |
IgG immunoglobulin transported across placenta by pinocytosis. IgM synthesised by foetal thyroid by 20 weeks |
|
|
What are the main NICE guidelines around postnatal care? |
Offer information to self-diagnose (signs and symptoms), encourage breastfeeding, give information on common health problems for babies, ask about emotional well being and support available |
|
|
What happens during the Zygotene ('paired threads') stage of prophase I? |
Chromosomes line up as homologous pairs. Synapsis (coming together) of homologous chromosomes |
|
|
What are the walls of the myometrium during the follicular phase of the menstrual cycle? |
Outer longitudinal, middle circular, inner longitudinal |
|
|
What determines the type of response (FSH or LH release) of the gonad to GnRH? |
Frequency of pulse. High (every 60-90 mins) = LH production. Low (every 120 mins) = FSH production |
|
|
How does the syncitiotrophoblast invade maternal blood vessels? |
By forming lacunae |
|
|
What happens during the embedding stage (days 7-8)? |
Inner cell mass forms, pre-embryo hatches (sheds zona pellucida) before implanting. Attaches to endometrium - posterior wall of uterine cavity |
|
|
What will the epiblasts of the primitive streak eventually form? |
Mesoderm and endoderm |
|
|
How do levels of nitric oxide change in the cevix at labour? |
L-arginine NO system up-regulated, NO metabolites increase |
|
|
How are vitamins transported across the foetal membrane? |
Fat soluble ones diffuse across lipid membranes. Water soluble ones require active transport, act as cofactors for enzymatic reactions |
|
|
During follicular development, what upregulates FSH receptors? |
Granulosa cells |
|
|
What happens during the Leptotene ('twin threads') stage of prophase I? |
Chromosomes become individualised, form visible strands in the nucleus. Short duration, progressive condensation and coiling of chromosome fibres take place |
|
|
What is the correct order of follicular development? |
Primary follicle, graafian follicle, ovulation, corpus luteum |
|
|
What would continuous administration of GnRH do to the ovarian cycle and why? |
Abolish the cycle. E.g. stress causing amenorrhoea. Reason is that pituitary gonadotropins inhibit further production of GnRH in healthy state |
|
|
What is pre-eclampsia? |
Pregnancy induced hypertension (>140/90 mmHg after 20 weeks) accompanied by proteinuria |
|
|
How is the primitive groove formed? |
Epiblast cells migrate by invagination and ingression through the primitive groove into the hypoblast |
|
|
Where does extraembryonic endoderm originate from and what does it give rise to? |
Hypoblast, give rise to yolk sac, source of nutrition for embryo |
|
|
What effect does relaxin have on the cervix? |
Increases collagenase activity via mitogenic effect on fibroblasts |
|
|
How are non-protein nitrogens (urea, uric acid, creatinine) transported across the foetal membrane? |
Excreted by foetus, diffuse across placenta. Note creatinine does not diffuse easily |
|
|
What is the effect of oestrogen on cervical mucus consistency? |
Gives it high water content |
|
|
What is crossing over (Chiasmata) and why is it important? |
Swapping of alleles between maternal and paternal chromosomes. Allows genetic diversity, referred to as recombination of genes |
|
|
What is follicular atresia? |
Complete degeneration and resorption occurs in primordial, primary and secondary follicles. Formation of hyaline scar tissue (corpus fibrosum) in tertiary follicles |
|
|
What type of molecules are FSH and LH and what do they act on? |
Glycoproteins, ovary and testes |
|
|
What do trophoblast cells differentiate into when they become invasive (5-6 days)? |
Cytotrophoblast (cellular inner layer) and Syncitiotrophoblast (syncitial epithelial layer) |
|
|
What does endoderm from the primitive streak give rise to (extraembryonic)? |
Allantois, functions in gas exchange and waste disposal for the embryo |
|
|
What are the effects of progesterone on the cervix? |
Inhibits collagenase, potent anti-inflammatory. Used in obstetrics, gynaecology and miscarriage/ TOP/ IUD |
|
|
Why are excretory products higher in the foetal circulation than maternal? |
Diffusion gradients required for transport |
|
|
Where does the axial skeleton develop from during human development? |
Sclerotome |
|
|
What covers chorionic villi in the term placenta? |
Layer of syncytiotrophoblast cells |
|
|
How is the process of cell division different in meiosis? |
No cycle, have G1, S and G2 phases for first division (2 divisions to produce 4 daughter cells) |
|
|
At what stage of follicular development can follicular atresia (degeneration) occur? |
Throughout follicular development |
|
|
What is the feedback effect of low plasma oestrogen concentration? |
Throughout follicular development |
|
|
What is the feedback effect of low plasma oestrogen concentration? |
No feedback effect, increased GnRH leading to increased FSH and LH and increased oestrogen |
|
|
How can conjoined twins be formed? |
When inner cells mass does not completely separate |
|
|
Which visceral organs does embryonic endoderm from the primitive streak give rise to? |
Gut tube, abdominal organs (liver/ pancreas), trachea and lungs, auditory system, urinary system |
|
|
What are the three theories for what initiates labour? |
Foetal cortisol levels, decline in progesterone sensitivity, corticotropin-releasing hormone (CRH) rise |
|
|
What is bilirubin and how is it excreted? |
Breakdown product of haemoglobin. Unconjugated form broken down by maternal liver. Becomes conjugated in bile then reabsorbed/ secreted when it reaches the gut |
|
|
How can the pelvic cavity be described in the female pelvis? |
Shallow |
|
|
What happens during G2 phase of interphase? |
Continued cell growth (4 hours), production of proteins for cell division |
|
|
What are the functions of exocrine category sertoli cells? |
Production of fluid to move immobile sperm out of testes, production of ABP, determination of rate of spermiation |
|
|
What is the feedback effect of moderate plasma oestrogen concentration? |
Negative feedback - reduced GnRH therefore reduced FSH and LH and reduced oestrogen |
|
|
How can monozygotic (identical) twins be formed? |
2 cell pre-embryo splits (two placentas, chorions, amnions) or inner cell mass splits - common trophoblast/ placenta and chorion. Can also have splitting of bilaminar embryo after implantation |
|
|
What does extraembryonic mesoderm from the primitive streak give rise to? |
Yolk sac, amnion, chorion |
|
|
Where is oxytocin secreted from and what are its main features? |
Posterior pituitary (maternal and foetal). Induces uterine contraction in response to cervical dilatation. Increased strength and frequency of contractions. Stimulates prostaglandin synthesis |
|
|
Why are babies commonly jaundiced? |
Liver functions poorly first week of life, incapable of unconjugating significant quantities of bilirubin. Treated by phototherapy |
|
|
What type of epithelium is found in the upper respiratory tract? |
Pseudostratified |
|
|
What happens during the S phase of interphase? |
Replication of DNA (8 hours). Chromatids joined at centromeres |
|
|
What do theca externa and fibroblasts produce to stop hormone production? |
Collagen |
|
|
What enhances the negative feedback effect of oestrogen on FSH and LH? |
Progesterone |
|
|
In the morula, which cells differentiate at blastocyst stage? |
Inner cells become inner cell mass, outer cells become trophoblast cells |
|
|
What does embryonic mesoderm from the primitive streak give rise to? |
Notochord, adult tissues: endothelium, bone, cartilage, skeletal/ smooth muscle, blood, lymph, heart, kidneys, spleen, reproductive system, limbs |
|
|
What substance is commonly used to induce/ augment labour? |
Synthetic oxytocin (Syntocinon) |
|
|
How does plasma volume change during pregnancy? |
Increased 40% |
|
|
What happens to the uterus during pregnancy? |
Size, shape and position change, volume increases from 4ml to 5L. Weight increases from 50-60g to 1kg |
|
|
What does each corpus luteum contain? |
Central blood clot |
|
|
What is the hormone profile of menopause? |
Reduced oestrogen levels, therefore increased FSH and LH levels |
|
|
What is the blastocyst composed of? |
32+ Blastomere cells - inner cell mass (becomes foetus) and trophoblast cells (become placenta). Also blastocoele (cavity) |
|
|
What are the features of ectoderm? |
Derived from epiblast, induced to form neural plate by the notochord. Gives rise to nervous system and sensory organs (neural ectoderm), also gives rise to epidermis (surface ectoderm) |
|
|
What is the mechanism for preterm labour? |
Maternal HPA axis activation in maternal/ foetal stress --> placenta/ decidua/ foetal membrane produce CRH (--> prostaglandin release) and oestrogen (--> activates myometrium) |
|
|
How does RBC volume change during pregnancy? |
Increased 20% (w/o iron) Increased 30% (w/ iron) |
|
|
What happens during the G0 stage of interphase? |
Cell exits cycle, known as post-mitotic. E.g. neurones |
|
|
What happens to theca interna cells for them to become theca lutein cells and what do they secrete? |
They change shape in the corpus luteum, secrete progesterone |
|
|
What is the feedback effect of prolonged (>48 hours) high plasma oestrogen concentration? |
Positive feedback - increased GnRH leading to increased FSH and LH - ovulation |
|
|
What is the term for human development at 4 days and when is it implanted? |
Blastocyst, 5-7 days |
|
|
What is the neural crest? |
Clinically important cells populations from neuro-ectoderm. Classified at cranial or cardiac |
|
|
What factor accounts for 20-40% of spontaneous preterm labours? |
Infection/ inflammation --> cytokine activation which produces prostaglandins, leukotrienes, proteases in membranes, myometrium and cervix |
|
|
How do haemoglobin levels change during pregnancy? |
Overall amount the same but lower % of RBCs - called haemodilution |
|
|
What are the three parts of the broad ligament? |
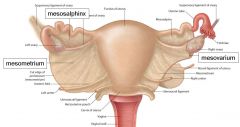
Mesometrium, mesosalphinx, mesovarium |
|
|
What separates the oocyte and the antrum in the tertiary follicle? |
Cumulus oopherus (granulosa cells) |
|
|
Inhibins and activins are dimers that are secreted by granulosa cells. They are not specific to the ovaries. What is the function of inhibins? |
They are stimulated by FSH/LH. They inhibit FSH production |
|
|
What is the term for the collection of 16 cells at 3 days human development? |
Morula |
|
|
What is neural induction (18-19 days)? |
Notochord becomes elongated, induces overlying ectoderm to become neural plate by releasing molecular signals |
|
|
What are the risks and options for treating a delay during the third stage of labour? |
Haemorrhage risk - oxytocin and CCT. Delay if >30 minutes to deliver placenta and foetal membranes |
|
|
How does white blood cell count change during pregnancy? |
Increased 8% |
|
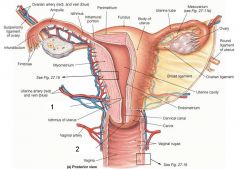
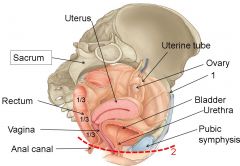
What are denoted by labels 1 and 2 on this image of the female reproductive system? |
Internal and external os |
|
|
At puberty, approximately how many additional follicles are stimulated to develop and what happens to them? |
40 - undergo atresia (closure) after granulosa cell division and appearance of zona pellucida |
|
|
Inhibins and activins are dimers that are secreted by granulosa cells. They are not specific to the ovaries. What is the function of activins? |
Stimulate FSH production, inhibit androgen production. However also stimulate conversion of androgens to oestrogens |
|
|
What happens during the cleavage stage of human development? |
2 --> 8 blastomeres. 5+ days removal of zona pellucida (hatching) to allow implantation |
|
|
How is the neural tube formed (15-28 days)? |
Lateral edges of neural plates become elevated, results in formation of neural folds. Neural folds meet and fuse |
|
|
What are the results of uterine distension? |
Restricted normal uterine expansion - polyhydramnios, multiple pregnancy, uterine abnormalities |
|
|
What happens to plasma albumin during pregnancy and why is this significant? |
Decreases - reduces oncotic pressure leading to peripheral oedema |
|
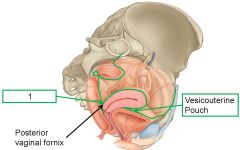
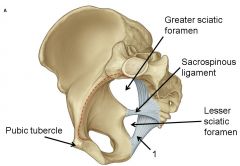
What is denoted by label 1 on this sagittal view of the female pelvic viscera? |
Rectouterine Pouch (of Douglas) |
|
|
What structures are formed by stromal cell condensation in the secondary follicle? |
Theca interna and theca externa |
|
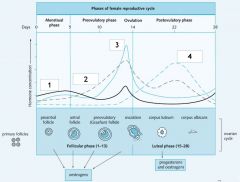
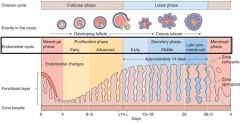
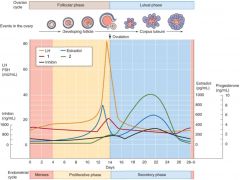
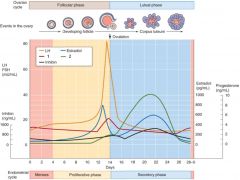
Which hormone is responsible for the line labelled 1 on this graph of the female reproductive cycle? |
FSH |
|
|
How are oocytes ensured to remain haploid until pronuclei combine? |
Polar bodies - formed by uneven cell division in meiosis |
|
|
When the neural tube is formed, what do neural crest cells migrate away to become? |
PNS, Schwann cells, melanocytes, endocrine cells, craniofacial structures, cardiovascular structures |
|
|
What are the results of stretching of myometrium and foetal membranes in preterm labour? |
Myometrial activation, enhanced gap junction formation, increase in oxytocin receptors, increased prostaglandin synthesis |
|
|
How do blood clotting components change during pregnancy and why is this significant? |
(Reduced platlet count) Reduced fibrinolytic activity, increased fibrinogen and pro-coagulant factors. Prevents bleeding to death during delivery but increases risk of thromboembolism |
|
What is denoted by label 2 on this sagittal view of the female pelvic viscera? |
Perineum |
|
|
How are cystic spaces formed in the adult ovary? |
Epithelial cells secrete fluid |
|
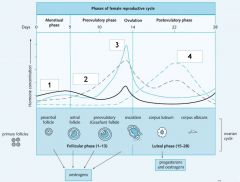
Which hormone is responsible for the line labelled 2 on this graph of the female reproductive cycle? |
Oestrogen |
|
|
What are the results of sperm entry? |
1st and 2nd polar bodies formed from meiotic divisions Formation of male and female pornucleus Pronuclei disolve and release genetic material First cleavage division |
|
|
What can genetic defects in neural crest cells cause? |
Craniofacial and cardiac defects |
|
|
What is the cause of rhesus haemolytic disease of the newborn? |
Lack of anti D antibodies from parents - leads to jaundice, anaemia |
|
|
How does the size of the heart change during pregnancy and why? |
Enlarges by 12% - increased diastolic filling, cardiac muscle hypertrophy |
|
|
How do insulin levels change during the puerperium? |
Response returns within 2 days, glucose response remains as in pregnancy for longer. Both normal by 6 weeks |
|
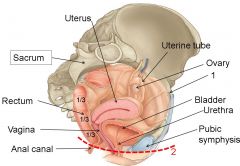
What is denoted by label 1 on this sagittal view of the female pelvic viscera? |
Round ligament |
|
|
Blood vessels, nerves and lymphatic enter the ovary through the hilum of the ovary. Where does follicular development and maturation occur in the adult ovary? |
Stroma of the outer cortex |
|
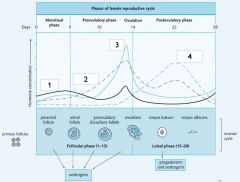
Which hormone is responsible for the line labelled 3 on this graph of the female reproductive cycle? |
LH |
|
|
What are examples of teratogens? |
Radiation, alcohol, thalidomide, lithium (CV), valium, infectious agents e.g. rubella (effects of time dependent) |
|
|
What three subdivisions does mesoderm differentiate into when the neural tube is formed? |
Paraxial, intermediate and lateral plate mesoderm |
|
|
Which infectious diseases are tested for during antenatal care? |
HIV, Hep B, Rubella, Syphilis, Chlamydia, Asymptomatic bacteriuria |
|
|
Other than size, what other changes happen to the heart during pregnancy? |
Apex beat moves upwards, laterally due to diaphragm displacing the heart. Systolic murmur develops |
|
|
How do thyroid hormones such as Thyroxine Binding Globulin (TBG) change during the puerperium? |
TBG returns over 6 weeks, T3 and T4 return slowly. Cortisol raised in labour, returns in 1 week |
|

What is denoted by label 1 on this image of the female pelvic viscera? |
Cervix |
|
|
In the embryonic ovary, what are primordial germ cells surrounded by? |
Mesenchymal stroma |
|
|
Which hormone is responsible for the line labelled 4 on this graph of the female reproductive cycle? |
Progesterone |
|
|
At what phase of human development do genetic defects become apparent? |
Embryo phase |
|
|
What does paraxial mesoderm later become? |
Bone, cartilage, tendons, ligaments, skeletal muscle, dermis of skin |
|
|
How is Down's Syndrome normally tested for? |
Combined nuchal translucency and blood test, serum screening 15-20 weeks. Targeted to high risk group |
|
|
How does cardiac Output change during pregnancy? |
Increases 35-40% in first trimester (4.5L/min --> 6-7L/min). Both HR and SV increase |
|
|
How do hCG and hCS change during the puerperium? |
Undetectable 10 days following delivery |
|
|
Why is folate supplementation need to prevent neural tube defects (genetic basis)? |
Common genetic variant - MTHFR667. Changes GCC Alanine to GTG Valine - increased thermolability, reduced function |
|
|
What is the fifth stage of foetal delivery? |
Anterior shoulder descends below symphysis. Anterior shoulder birthed first then posterior |
|
|
What are other terms for a mature follicle? |
Tertiary/ Graafian |
|
|
When are the 28 days of the menstrual cycle calculated from? |
First day of menstrual bleed |
|
|
What is the difference between totipotency and pluripotency? |
Totipotency means cells with potential for form any cell type/ tissue in the body. Pluripotency excludes the placenta |
|
|
What does intermediate mesoderm later become? |
Kidneys, lower urinary tract, reproductive system |
|
|
What are the ethical issues associated with Down's Syndrome? |
High rate of spontaneous abortion, structural congenital abnormalities (e.g. cardiac), mental retardation, other medical problems (e.g. leukaemia, hyperthyroidism, epilepsy, Alzheimer's) |
|
|
How does blood pressure change during pregnancy? |
Decreases during 2nd trimester by 10-20mHg due to peripheral vasodilation. Rises to pre-pregnancy levels during 3rd trimester |
|
|
How do FSH and LH levels change during the puerperium? |
Remain low until 10 days, increase dependent on lactation. FSH returns faster than LH |
|
|
What is aetiology? |
Why an illness/ condition happens |
|
|
What is the fourth stage of foetal delivery? |
Head realigns with shoulders (restitution) which then rotate to lateral position |
|
|
What is the normal duration of life for the corpus luteum (assuming no pregnancy) and why is this clinically relevant? |
14 days - produces progesterone to support implantation. Shortened luteal phase typically leads to infertility |
|
|
What muscle layers comprise the female genital tract? |
Outermost and innermost (longitudinal SM) and middle (circular SM) |
|
|
What is gravidity and parity? |
Gravidity is number of pregnancies, parity is number of births >24 weeks (inc. stillbirth) |
|
|
What does lateral plate mesoderm later become? |
Smooth muscle, blood, lymph, adipose, heart, spleen, limbs, endothelium |
|
|
What is the cause of supine hypertension in pregnancy and why is it dangerous? |
From 20 weeks uterus compresses IVC and abdominal aorta, lowering CO by 30%. Can result in loss of consciousness, cause foetal demise |
|
|
How do levels of prolactin change during the puerperium? |
Levels depend on lactation, fluctuate |
|
|
What is the third stage of foetal delivery? |
Occiput clears pubic symphysis, head extends to deliver (sits on maternal perineum) |
|
|
What happens to the haploid oocyte and first polar body after fertilisation/ meiosis II? |
Second polar body formed, first polar body undergoes meiosis II to form 3rd polar body |
|
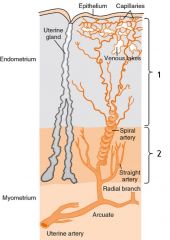
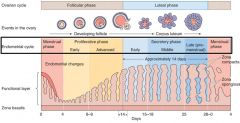
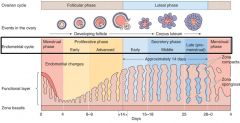
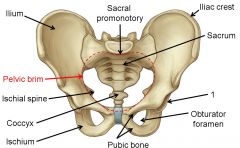
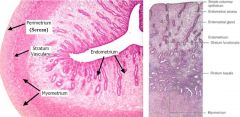
What is denoted by label 1 on this image? |
Functional zone |
|
|
Why is pregnancy calculated as 40 weeks instead of the 38 for human development? |
Time of last period is two weeks before ovulation, therefore 2 weeks before development begins. Easier to remember time of last period as opposed to time of fertilisation |
|
|
What is cell fate (e.g. mesoderm to bone) regulated by? |
Gradients of signalling factors/ their inhibitors (morphogen inhibitors) produced by distance from source and presence of inhibitors |
|
|
What is pre-eclampsia? |
Pregnancy induced hypertension (>140/90 mmHg after 20 weeks) accompanied by proteinuria |
|
|
How do levels of oestrogen and progesterone change during the puerperium? |
Decrease to non-pregnant levels by 72 hours |
|
|
What cardiovascular test readings would be expected during pregnancy? |
Flattened T-wave, depressed ST segment of ECG, cardiac muscle hypertrophy on echo |
|
|
What is the second stage of foetal delivery? |
Occiput rotates and reaches levator ani (gutter of pelvic floor) |
|
|
What is a polar body? |
Small cytoplasmic exclusion body which contains the excess DNA formed during meiosis of oocyte |
|
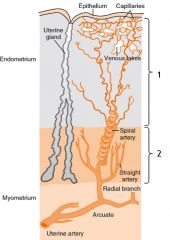
What is denoted by label 2 on this image? |
Basal zone |
|
|
What are the probabilities of fertilisation during fertile window for each frequency of intercourse? |
Every day - 37% Every two days - 33% Once - 15% |
|
|
Where are signalling factors released from in embryology? |
Node/ notochord. E.g. Ectoderm to neural: BMP4 (inhibited by noggin). Mesoderm mediated by MBP, FGFs |
|
|
What additional factors lead to pre-eclampsia being labelled as severe? |
Symptoms (headache, epigastric pain), severe maternal hypertension, biochemical/ haematological abnormalities, severe foetal growth retardation |
|
|
How are clotting factors affected during the puerperium and why is this dangerous? |
Increased clotting factors (esp. fibrinogen) first 10 days. Platelets fall after delivery then increase markedly. Hypercoagulable state remains for 6-7 weeks - increased risk of deep vein thrombosis, pulmonary embolism |
|
|
What is the first stage of foetal delivery? |
Head flexes as uterus contracts. Head descends and engages pelvis, appears side on |
|
|
What action completes oogenesis? |
Sperm entry to complete second meiotic division |
|
What happens during the proliferative phase of the menstrual cycle and what hormone is primarily responsible? |
Functional layer develops, basal layer unchanged. Endometrium doubles in size, glands change from straight to coiled, packed. Oestrogen is responsible |
|
|
How long can sperm survive in the female genital tract? |
5 days |
|
|
What does paraxial mesoderm differentiate at day 19? |
Sclerotome, dermomyotome |
|
|
How does progesterone promote quiescence? |
Reduced numbers of gap junctions, reduced prostaglandin synthesis |
|
|
What are the consequences of increased GFR during pregnancy? |
Increased excretion of urate, glucose, bicarbonate and creatinine - causes mild glycosuria and proteinuria |
|
|
How does plasma volume change during the puerperium? |
Remains elevated for 72 hours then returns to normal in 7-9 days |
|
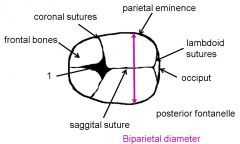
What is denoted by label 1 on this image of the foetal skull? |
Anterior fontanelle |
|
|
What happens to the corpus luteum if pregnancy does not occur? |
No hCG produced, corpus luteum degenerates to form corpus albicans |
|
What happens to cell nuclei and vacuoles during the secretory phase of the menstrual cycle? |
Switch places so nuclei sit near basement membrane, vacuoles near lumen to deposit contents. Known as basal --> subnuclear vacuolation |
|
|
What is the zona reaction associated with the slow block reaction of preventing polyspermy? |
Prevention of sperm binding to zona pellucida through structural changes |
|
|
Where does intraembryonic coelom form? |
Within lateral plate mesoderm |
|
|
How does oestrogen help to initiate labour? |
Increased number of gap junctions, prostaglandin synthesis, oxytocin receptors and local oxytocin production |
|
|
During pregnancy renal pelvises and calyces become dilated. What are the consequences of this? |
Urinary stasis, UTI. Can lead to pyelonephritis (kidney infection) |
|
|
How does the heart change structurally during the puerperium? |
Changes resolve by 2 weeks (size, murmur) |
|
|
What is the purpose of the puborectalis muscle? |
Maintains anal continence by forming puborectal sling |
|
|
What happens to the corpus luteum if pregnancy occurs? |
Placenta formation stimulated, hCG produced by syncytiotrophoblast cells. Corpus luteum produces hormones for 8 weeks until placenta can take over |
|
What happens during the early secretory phase of the menstrual cycle? |
Straight simple glands become irregular, corkscrew shaped. Basal vacuolation |
|
|
What is the cortical reaction associated with the slow block reaction of preventing polyspermy? |
Formation of impenetrable oocyte membrane |
|
|
How does the neural tube close? |
Head to tail direction. Anterior neuropore internalised by day 24/25, posterior by 27-29. Intracembryonic coelom creates horseshoe shape |
|
|
What are the features of the first stage of labour? |
Latent and active phases, 'show', ruptured membranes |
|
|
What are the main position changes of the respiratory system during pregnancy? |
Thoracic cage circumference increases 5cm, diaphragm rises 4cm. Breathing changes from costal to diaphragmatic |
|
|
How does cardiac output change during the puerperium? |
Remains elevated for 48 hours then returns to normal within 10 days |
|
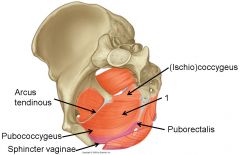
What is shown by label 1 on this image of the pelvic floor? |
Iliococcygeus |
|
|
What happens to granulosa and theca cells in the corpus luteum after ovulation? |
They acquire lutein, produce large amounts of progesterone, small amount of oestrogen |
|
|
What happens during the middle secretory phase of the menstrual cycle? |
Glands become convoluted, saw-tooth like. Decidualisation of stroma occurs |
|
|
What is the slow block reaction of preventing polyspermy? |
Oocyte secreting lyzozymes from cortical granules |
|
|
What condition is caused by failure of the anterior neuropore to close? |
Anencephaly |
|
|
What are the features of the second stage of labour? |
Passive descent for 1-2 hours, then push. Normal stages of passenger through pelvis |
|
|
What is lochia alba? |
Slightly white vaginal discharge 4-8 weeks post delivery. Contains few RBC, mainly WBC, fat and mucus |
|
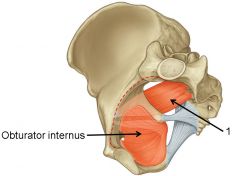
What is denoted by label 1 on this image of the pelvic walls? |
Piriformis |
|
|
What happens to the empty follicle (corpus luteum) after ovulation? |
Antral cavity fills with blood from damaged vessels. RBCs and debris removed by macrophages, fibroblasts fill cavity. |
|
|
What happens during the late secretory phase of the menstrual cycle? |
Saw-tooth appearance, copious thick glycogen and glycoprotein rich secretions (subnuclear vacuolation). Decidualisation continues |
|
|
What is the fast block reaction of preventing polyspermy? |
2-3 seconds after fusion, electrical depolarisation of ovum plasma membrane through Na+ channels. Prevents other sperm adhering to membrane, lasts <5mins |
|
|
What condition is caused by failure of the posterior neuropore? |
Spina bifida |
|
|
What are the features of the third stage of labour? |
Myometrium contracts, placenta is incompressible and sits below the plane of cleavage. Placenta shears away from the uterus, delivered vaginally. |
|
|
Why does tidal volume increase during pregnancy? |
Progesterone sensitises medulla oblongata. Can lead to over breathing (respiratory alkalosis) |
|
|
What is lochia serosa? |
Brownish/ pink thinner vaginal discharge up to 10 days post delivery. Contains RBC, WBC, cervical mucus |
|
|
How does the female pelvis differ from the male? |
Circular pelvic inlet (heart) Larger angle at 80-85 degrees (50-60) Everted ischial spines (inverted) Flat sacrum (concave) Male equivalent in brackets |
|
|
What happens to the follicle during ovulation? |
Wall swells rapidly, protrudes (stigma). Fluid oozes from protrusion, follicle ruptures. Follicular fluid carries oocyte-cumulus complex |
|
|
What is decidualisation of stroma? |
Response to implantation, involved endometrial stroma transforming into enlarged, glycogen filled decidual cells that serve to inhibit migration of implanting embryo |
|
|
Out of the up to 1x10^6 sperm per ejaculate, how many reach the ampulla of the uterine tube? |
200-300 - first step in preventing polyspermy |
|
|
What do the anterior and posterior neuropores of the neural tube become? |
Anterior - pericardial and pleural cavities. Posterior - peritoneal cavity |
|
|
What is the average estimated blood loss during labour? |
500ml |
|
|
What are the main GI changes during pregnancy? |
Increased appetite, thirst, nausea, vomiting, bile production (cholestasis). Risk of rectal haemorrhoids. Reduced motility of small and large intestine (can cause constipation). Also heartburn, reflux oesophagitis |
|
|
What may the persistence of lochia rubra indicate? |
Presence of retained placental tissues or foetal membranes |
|
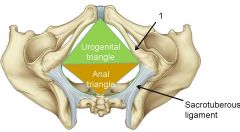
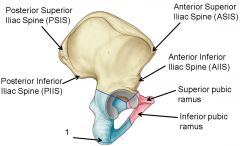
What is denoted by label 1 on this inferior image of the female pelvis? |
Inferior pubic ramus |
|
|
When the dominant follicle arrests during the second meiotic division during metaphase II, what is formed? |
Haploid oocyte, first polar body |
|
What hormone is denoted by label 1 on this graph? |
FSH |
|
|
What is polyspermy and what is the result? |
Multiple sperm fertilising a single egg - results in inviable zygote due to multiple chromosome copies |
|
|
What are neural tube defects (NTDs)? |
Abnormal neural tube closure, mostly in lumbar region (posterior neuropore, e.g. spina bifida) |
|
|
How can the third stage of labour be actively managed? |
Oxytocin (syntocinon) and continuous cord traction (CCT) - suprapubic pressure, gentle continuous traction |
|
|
What are the main changes to the skin during pregnancy? |
Increased pigmentation, stretch marks (collagen), spider naevi, palmar erythema, cell cycle growth changes (great hair then hair loss), gum bleeding (pregnancy gingivitis) |
|
|
What is lochia rubra? |
Red, thick vaginal discharge 3-5 days post delivery. Consists of fresh blood and decidual debris |
|
What is denoted by label 1 on this medial image of the female pelvis? |
Sacrotuberous ligament |
|
|
What happens to the dominant follicle during the pre-ovulatory phase (follicular)? |
Increase in follicular volume, responds to LH surge by completing 2nd meiotic division - arrests in metaphase II |
|
What hormone is denoted by label 2 on this graph? |
Progesterone |
|
|
What sort of change is activation in terms of fertilsation and what is its purpose? |
Morphological (as opposed to biochemical) - irreversible. Allows sperm to successfully penetrate and fuse with egg |
|
|
Why does the trilaminar embryo fold at the start of the 4th week? |
Neural tube proliferates at a faster rate than the rest of the disc |
|
|
What are the main problems associated with prematurity? |
Cerebral palsy, blindness, chronic lung disease (surfactant only produced from 32 weeks), disability |
|
|
What are the common musculoskeletal changes during pregnancy? |
Softening and relaxation of joints in the lower back and pelvis. Exaggerated lumbar lordosis leads to typical gait of late pregnancy |
|
|
What happens to the cervix and vagina during the puerperium? |
Cervix can be damaged, vaginal involution takes up to 8 weeks. Vaginal epithelium is thinner if lactating (hypo-oestrogenic) |
|
What is denoted by label 1 on this lateral image of the female pelvis? |
Ischial tuberosity |
|
|
What happens to the oocyte during the pre-ovulatory phase (follicular)? |
Cumulus oopherus neck breaks down, oocyte becomes free floating |
|
|
What effect does oestrogen have on the cervix? |
Makes mucus thin and watery, full of electrolytes. Results in high spinbarkeit (stretchable) as strands align |
|
|
What is activation in terms of fertilisation? |
Acrosome reaction in uterine tubes in vicinity/ contact with oocyte Release of hydrolytic enzymes, fusion between plasma membrane and acrosome |
|
|
Why does the embryo become C-shaped at the end of the 4th week? |
Longitudinal folding - heart and diaphragm now inside the embryo |
|
|
What treatments are given to premature babies/ women at high risk? |
Steroids (foetal lung maturation), tocolytic drugs (atosiban - oxytocin inhibitor) and magnesium sulphate (neuro protection) |
|
|
There is a positive correlation between weight gain during pregnancy and birth weight. How does maternal weight change during pregnancy? |
Average gain 12.5kg. 0.3kg/wk (0-18) 0.45kg/wk (18-28) 0.36/0.41kg/wk (28-term). |
|
|
What happens to the endometrium during the puerperium? |
Regenerates within 6 weeks if no lactation |
|
What is denoted by label 1 on this anterior image of the female pelvis? |
Acetabulum |
|
|
How is an oocyte formed before the ovarian cycle? |
Germ cell --> mitosis to oogonium --> meiosis to primary oocyte. Arrests during 1st meiotic division (diplotene) |
|
|
What effect does progesterone have on the cervix? |
Makes mucus thick and viscid. Results in low spinbarkeit (strands cross over) to create a barrier |
|
|
What type of change is capacitation? |
Biochemical (as opposed to morphological). Reversible by exposure to prostatic secretions |
|
|
What is exstrophy? |
Failure in folding and incorporation of mesoderm during develoment - external bladder |
|
|
What three classes are delays in labour put into? |
Powers, Passenger Pelvis |
|
|
What are the maternal/ foetal consequences to an extreme maternal BMI? |
<17 increases risk of foetal growth retardation and perinatal mortality. >30 increases risk of developing gestational diabetes and hypertesion |
|
|
How does the uterus recover during the puerperium? |
Weight reduces from 1kg to 50-60g. Reduces by 50% in first 7 days. Uterine muscle fibres undergo autolysis and atrophy |
|
|
What do the ovaries secrete? |
Large amounts of oestrogens, small amounts of androgens. Progesterone to prepare uterus for pregnancy. Relaxin to loose ligaments in pubic symphysis, soften cervix to facilitate delivery |
|
|
How is the antrum formed at the antral phase? |
Follicular fluid released by granulosa cells form small pockets in follicle which eventually coalesce |
|
|
What is the mechanism of action of the progesterone-only contraceptive pill? |
Affects cervical mucus, forms mechanical barrier. No effect on ovulation |
|
|
What is capacitation? |
Post-ejaculatory conditioning process. Interaction with female tract mucosa. Takes 7 hours. Removal of glycoproteins and sterol groups from plasma membrane of motile sperm. |
|
|
The placenta is a compound organ. What is it derived from? |
Villus chorion (foetal) and decidua from endometrium (maternal) |
|
|
What are the options for treating a delay during the first stage of labour? |
Powers: augment contractions (amniotomy, give oxytocin). Can't affect passenger/ pelvis |
|
|
What is the normal pattern of weight loss following pregnancy? |
Rapid loss first 4-10 days, then more gradual. Women tend to retain ~3kg for a long time |
|
|
What is the puerperium? |
The 6 week (42 day) period following delivery of a baby where the physiological adaptations of pregnancy return to a non-pregnancy state |
|
|
What do the testes secrete? |
Large amounts of androgens, small amounts of oestrogens |
|
|
What happens to granulosa cells during the antral phase? |
Develop FSH receptors, do not produce ovarian hormones at this stage |
|
|
What is the fertility awareness method (FAM) of contraception? |
Training women to be aware of fertility signs such as increased basal body temperature (0.5 degrees at ovulation). Allows planning of intercourse |
|
|
What two processes are essential for fertilisation? |
Capacitation and activation |
|
|
What is secondary villus present at the development of the placenta (day 17)? |
Villus containing both cytotrophoblast and extraembryonic mesoderm |
|
|
What are the options for treating a delay during the second stage of labour (>1 hour active pushing)? |
Powers: encouragement, amniotomy (+/- syntocinon), instrumental delivery. Passenger: Malpositioning, malpresenting. Can't affect pelvis |
|
|
What happens to the fallopian tubes and ovaries during pregnancy? |
Enlarge and elongate, cessation of ovulation |
|
|
What is the cause of constipation in pregnancy? |
Progesterone-induced SM relaxation |
|
|
The pO2 of maternal blood in placental sinuses is 50mmHg but the pO2 of foetal blood following oxygenation is nly 30mmHg. How can the foetus obtain sufficient oxygen? |
Foetal haemoglobin has higher affinity for oxygen, no interaction with 2,3-DPG. Can bind oxygen at lower pO2 |
|
|
What happens to the theca in the antral phase? |
Splits into externa and interna, develop LH receptors to bind LH and produce androgens |
|
|
What is the effect of oestrogen on the vagina? |
Stimulates proliferation of vaginal epithelium, increased glycogen content |
|
|
What are the main stages of human development? |
Cleavage, blastocyst formation, implantation, placenta formation, beginning of uteroplacental circulation, gastrulation, formation of germ layers, formation of trilaminar disc, neural induction and neurulation, organogenesis |
|
|
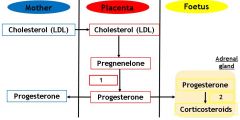
What is 3β-HSD and what is its function? |
Placenta-specific 3β-hydroxysteroid dehydrogenase. Converts pregnenelone to progesterone |
|
|
What are the risks and options for treating a delay during the third stage of labour? |
Haemorrhage risk - oxytocin and CCT. Delay if >30 minutes to deliver placenta and foetal membranes |
|
|
What happens to the cervix during pregnancy? |
Increased blood supply, remains 2.5cm throughout. Fills with mucus plug |
|
|
What is the cause of back ache in pregnancy? |
Oestrogen-induced ligament softening |
|
|
What are the clinical features of Cushing's syndrome? |
Weight gain (central), moon face (fat accumulation), atrophy of epidermis, hypertension, muscle weakness, osteoporosis, thirst/ polyuria (ADH inhibited) and psychological disturbances |
|
|
What is the antral phase (follicular) dependent on? |
FSH and LH - 15-20 follicles enter this phase, 1 becomes dominant |
|
|
What is the effect of progesterone on the vagina? |
Increased desquamation of epithelial cells |
|
|
What are examples of sperm with abnormal morphology? |
Condensed acrosome, small/ large head, double headed/ tailed, abnormal middle piece |
|
|
What is the amniochorion? |
Fusion of the amnion (faster growing) and the smooth chorion |
|
|
What are the complications associated with assisted vaginal delivery? |
Trauma (lacerations, damage to anal sphincter/ rectum)m, haemorrhage, infections, urinary retention/ bladder damage, shoulder dystocia |
|
|
What happens to the vagina during pregnancy? |
Increased blood supply, becomes more elastic to allow for dilation during delivery |
|
|
What is the cause of goitre in pregnancy? |
Raised serum TSH |
|
|
What are some of the areas that benefit from breastfeeding? |
IQ, immune system, nutrition/ metabolism, gut microbiome |
|
|
What causes Cushing's syndrome and how is Cushing's disease different? |
Chronic glucocorticoid (cortisol) excess. Commonly iatrogenic (caused by treatment). Spontaneous version can come from pit/adrenal abnormality or ectopic ACTH secretion. Cushing's disease is specifically as a result of a pituitary tumour |
|
|
The primordial follicle is an oocyte surrounded by flattened granulosa cells. What happens to the primordial follicle during the pre-antral (follicular phase)? |
Granulosa become cuboidal, zona pellucida forms, outer coat (theca) forms. Handful of these primordial follicles develop |
|
|
How do hormones regulate the female external genitalia? |
Health and function dependent on hormones. Structures of vulva show no marked changes during menstrual cycle |
|
|
What % of sperm have normal vitality? |
58% |
|
|
By what time is the placenta a major source of hormones and what are the main examples? |
8 weeks - steroids e.g. oestrogen/ progesterone, hCG, hCS, relaxin, prolactin |
|
|
What are the complications associated with C-section? |
Haemorrhage, infection, deep vein thrombosis, damage to other organs. Future pregnancy risk (scarred uterus) |
|
|
The pO2 of maternal blood in placental sinuses is 50mmHg but the pO2 of foetal blood following oxygenation is nly 30mmHg. How can the foetus obtain sufficient oxygen? |
Foetal haemoglobin has higher affinity for oxygen, no interaction with 2,3-DPG. Can bind oxygen at lower pO2 |
|
|
What happens to the uterus during pregnancy? |
Size, shape and position change, volume increases from 4ml to 5L. Weight increases from 50-60g to 1kg |
|
|
What is the cause of morning sickness in pregnancy? |
hCG/ rising oestrogen levels |
|
|
What is the differential diagnosis for ectopic pregnancy? |
Acute abdominal (RLQ/ LLQ) pain in a woman of reproductive age |
|
|
Even though it is a glucocorticoid, cortisol has an appreciable affinity for another type of receptor. What is this receptor and why are cortisol's effects inhibited? |
Mineralocorticoid receptors - 11β-hydroxysteroid dehydrogenase in aldosterone responsive cells inhibits |
|
|
How many follicles are present at menarche (puberty) , atresia, growth and ovulation respectively? |
<300,000 / >270,000 / <30,000 / <500 dominant |
|
|
During the secretory phase of the menstrual cycle, what does the endometrium mainly consist of? |
Irregular corkscrew shaped glands |
|
|
What % of sperm have normal morphology? |
4% |
|
|
How can an accessory placenta form? |
Can form where blood supply remains good following formation of smooth chorion. Can cause post-partum haemorrhage in mother |
|
|
What is the risk of maternal death in the UK? |
1 in 10,000 |
|
|
How does the anterior pituitary change during pregnancy? |
Doubles in size, leading to increased corticotropin, prolactin and thyrotropin production. FSH and LH suppressed to to oestrogen/ progesterone negative feedback |
|
|
What is the cause of gestatoinal diabetes? |
Impaired glucose tolerance due to actions of cortisol |
|
|
What is the current incidence of ectopic pregnancy in the UK? |
1 in 90 |
|
|
During which two events is cortisol heavily synthesised? |
Circadian rhythm (early morning) and stress. Hypothalamus --> CRH --> Pituitary --> ACTH --> cortisol --> kidney |
|
|
Which physiological events occur due to the LH surge? |
Follicular pockets fuse, oocyte completes 1st meiotic division, begins 2nd. Oocyte becomes free from follicle |
|
|
What is the progressive motility of sperm? |
32% |
|
|
What happens to the placental decidua capsularis and decidua parietalis at 25 weeks? |
They fuse together completely, resulting in loss of uterine lumen |
|
|
What are the biggest causes of direct maternal deaths in the UK? |
Thromboembolism (36%), Sepsis (18%), Haemorrhage (17%) |
|
|
How does the iodine requirement (due to thyroid) change during pregnancy and why? |
Increases - mother needs to maintain thyroid function as well as transfer hormones to foetus. Transfer to foetus increases later in gestation. Also increased renal iodine clearance |
|
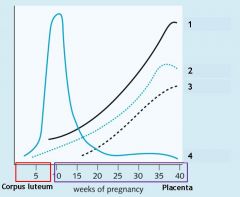
What is denoted by label 4 on this hormone profile of pregnancy? |
hCG |
|
|
What is the basis for a pregnancy test? |
hCG from the syncytiotrophoblast |
|
|
What are the general functions of glucocorticoids? |
Anti-inflammatory, immunosuppression - inhibit cytokine production (therefore T-cell proliferation) and inhibit prostaglandin and leukotriene production |
|
|
What are the acute metabolic actions of growth hormones (direct)? |
Release FAs from adipose tissue, enhance conversion to acetyl-CoA. reduce glucose metabolism and uptake into cells, increased gluconeogenesis, increased production of IGF-1 in the liver |
|
|
Which hormone signals to the corpus luteum to enlarge in the case of pregnancy? |
Human Chorionic Gonadotropin (hCG) |
|
|
What is the total motility of sperm (progressive and non-progressive)? |
40% |
|
|
What are the features of the term placenta? |
Maternal blood enters via uterine spiral arteries, filters down past villous chorion |
|
|
What are the biggest causes of indirect maternal deaths in the UK? |
Cardiac (30%), Neurological (18%) |
|
|
How are maternal glucose levels controlled during pregnancy? |
Mother produces enough insulin to counteract effect of hCS, glucagon, cortisol. Gestational diabetes = insulin resistance |
|
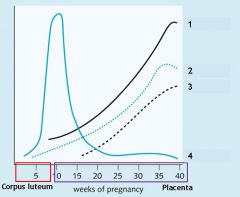
What is denoted by label 3 on this hormone profile of pregnancy? |
Oestrogen |
|
|
What is the incidence of ectopic pregnancy implantation in sites other than the uterine tube? |
2% |
|
|
Cortisol is a major glucocorticoid that is 90% bound to plasma proteins. What are its features and functions? |
Affects virtually all tissues through controlling gene transcription. E.g. stimulates hepatic gluconeogenesis, inhibits glucose uptake in muscle/ adipose, inhibits gonadal release of testosterone, oestrogen and progestins |
|
|
Growth hormone is another term for somatotropin, 191 amino acid peptide hormone synthesised by somatotrophs. What are the main features of growth hormone (HGH)? |
Released in response to GHRH, inhibited by somatostatin. Stimulates growth, cell reproduction and regeneration. Functions can be direct or indirect via insulin-like growth factor (IGF-1) |
|
|
What are the functions of the testes? |
Produce gametes, synthesise and secrete hormones |
|
|
What is the normal number of sperm per ejaculate? |
39x10^6 |
|
|
What are the features of tertiary villus and where is it located? |
Located in umbilical cord. Contains few cytotrophoblasts, more syncytiotrophoblasts (source of hCG) |
|
|
What are the biggest causes of late maternal death in the UK? |
Suicide (49%), cardiac (21%) |
|
|
What are the roles of the corpus luteum during pregnancy? |
Establishment of placenta, initiation of mammary gland development, inhibition of ovulation by negative feedback, increasing fat deposition |
|
|
By what time is the placenta a major source of hormones and what are the main examples? |
8 weeks - steroids e.g. oestrogen/ progesterone, hCG, hCS, relaxin, prolactin |
|
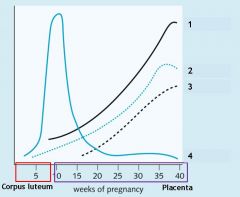
What is denoted by label 2 on this hormone profile of pregnancy? |
hPL and hCS |
|
|
What is the viability of ectopic pregnancies? |
Only intrauterine viable |
|
|
Why do the Zona Fasiculata and Zona Reticularis produce androgens and cortisol as opposed to aldosterone? |
Lack of CYP11B2 gene (P450aldo) |
|
|
How are hormone effects controlled? |
Modification (e.g. vit D, steroids), degradation, receptor down-regulation (e.g. adrenergic), termination of intracellular effects (e.g. phosphatases), negative feedback (by metabolite/ hormone itself/ trophic hormone) |
|
|
What is the function of the seminiferous tubules of the testes? |
Sperm production - takes 64 days |
|
|
What is the normal value for sperm concentration? |
15x10^6 /ml |
|
|
What is the relevance of syncytial knots/ sprouts? |
Detach and enter maternal circulation - accumulate in lungs (villous deportation). Increased number can be a sign of diabetes, hypertension, pre-eclampsia |
|
|
What are the underlying factors surrounding maternal death? |
Pre-existing condition, smoking, obesity, low socio-economic class, ethnicity, newly arrived immigrants, late booking/ no entenatal care, domestic abuse, child protection issues, substance misuse |
|
|
Why can the placenta be described as an impefect endocrine organ? |
Cannot manufacture adequate cholesterol (maternal supply as LDL) and lacks crucial enzymes for synthesis of estrone/ estradiol/ estriol (supplied by foetal adrenal gland, liver) |
|
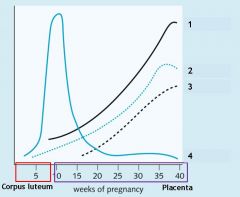
What is denoted by label 1 on this hormone profile of pregnancy? |
Progesterone |
|
|
What is protein suicide? |
Example is collagen - if any one strand in collagen triple helix is defective, whole strand is lost (severe osteogenesis imperfecta) |
|
|
What are some of the presenting features of a ruptured/ leaking ectopic pregnancy? |
Sudden severe pain, syncope and nausea, diarrhoea, shoulder pain |
|
|
At what point does neural tube closure take place? |
5-6 weeks pregnancy, 21-30 days development |
|
|
Aldosterone is a major mineralocorticoid that is 50-70% bound to albumin in plasma. What are its main features and functions? |
Acts on kidney/ colon/ salivary glands to maintain sodium concentration and ECF, upregulates ENaC and Na+/K+ ATPase |
|
|
Anterior pituitary hormones are released into systemic circulation. Release is controlled by hypothalamic hypophysiotropic hormones in portal hypophyseal vessels. What are the main examples of these hormones? |
TSH, FSH, LH, ACTH, GH, prolactin |
|
|
How long do sperm stay in the epididymis and why? |
11-14 days to mature and gain motility |
|
|
What volume of semen is produced per ejaculate? |
1.5ml |
|
|
What 4 regions is the uterus divided into? |
Fundus (dome shape similar to fallopian tubes), body, isthmus (lower uterine segment in pregnancy) and cervix (narrow opening into vagina) |
|
|
What are the features of the perimetrium/ serosa? |
Simple squamous and areolar connective tissue, forms broad ligaments laterally, utero-vesical pouch anteriorly, pouch of Douglas posteriorly |
|
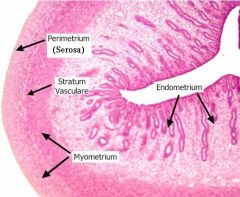
What are the main features of the myometrium of the uterus? |
Smooth muscle (myocytes) separated by connective tissue (collagen and elastin). Longituinal, circular and spiral orientations. Thickest at fundus, thinnest at cervix |
|
|
What are the main causes of stillbirth in the UK? |
Placenta (46%), congenital abnormality (21%) |
|
|
Which 3 enzymes does the foetus provide that the placenta lacks? |
3β-HSD, CYP17, CYP19 |
|
|
Where is relaxin produced and how do levels change throughout pregnancy? |
Secreted by placenta, CL, breasts, chorion. Peaks in 1st trimester and again at delivery |
|
|
During which period is folate supplementation recommended? |
One month before conception and in first trimester |
|
|
Why does the Zona Glomerulosa produce only aldosterone rather than androgens or cortisol? |
Lack of 17α-hydroxylase enzyme |
|
|
Posterior pituitary hormones are produced in the magnocellular neurones of the hypothalamus and stored in the posterior pituitary prior to release. What are the main examples of these hormones? |
Oxytocin (Uterine SM contraction, breast myoepithelial contraction) and ADH |
|
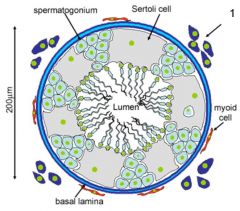
What is denoted by label 1 on this image of the interior of seminiferous tubules? |
Leydig cells |
|
|
What causes liquification of sperm? |
Fibrinolytic factors from the prostate |
|
What are the three main components of the endometrium? |
Simple columnar epithelium, underlying stroma (connective tissue) and endometrial glands (develop from epithelium, extend to myometrium) |
|
|
What factors increase the risk of stillbirth/ neonatal mortaility? |
Age (teenagers/ over 40s), social deprivation, ethnicity, prematurity, multiple pregnancy, substandard care |
|
|
What is 3β-HSD and what is its function? |
Placenta-specific 3β-hydroxysteroid dehydrogenase. Converts pregnenelone to progesterone |
|
|
What are the functions of relaxin? |
Mediates haemodynamic changes (increased CO, RBF) and relaxes pelvic ligaments |
|
|
Which test is normally used to identify possible spina bifida? |
Ultrasound at 18-21 weeks |
|
|
What percentage of the adrenal gland does the Medulla comprise of and what are its products? |
10-12%, epinephrine - highly specialised part of SNS |
|
|
What are the major functions of somatostatin? |
Inhibition of growth hormone, gastrin, VIP, glucagon and insulin release |
|
|
What is the spermatogenic cycle? |
Spermatogonia type A --> 4x mitosis --> Intermediate type spermatogonium --> Spermatogonia type B |
|
|
What are the main characteristics of human semen? |
>5% spermatozoa, 2/3 seminal vesicle secretions, 1/3 prostate, coagulates immediately after ejaculation, non-uniform composition |
|
|
What are the two layers of the endometrium? |
Stratum functionalis (lines cavity, sloughs off during menstruation) and stratum basalis (permanent, gives rise to new stratum functionalis) |
|
|
What is the mechanism of the foetal component of uteroplacental blood flow? |
Blood enters through spiral arteries in uteral wall, moves into intravillus space. Slow flow to allow adequate exchange, drains into larger maternal placental vein after bathing villi |
|
|
What is the function of CYP17? |
Converts progesterone to androgens (testosterone), glucocorticoids (cortisol) and mineralocorticoids (aldosterone) |
|
|
Where is prolactin secreted from and how do levels change during pregnancy? |
Secreted by placenta, pituitary, breasts and myometrium. Levels rise steadily from 5th week of pregnancy, levels are 10-20 times non-pregnant levels by birth |
|
|
What screening test is commonly used to indicate possible presence of a foetus with Down's Syndrome? |
Blood test plus nuchal translucency scan at 11-14 weeks |
|
|
What percentage of the adrenal cortex does the Zona Reticularis comprise of, where is it located and what are its products? |
10% (less lipids), inner layer, cortisol and androgens |
|
|
The hypothalamus releases hypophysiotropic homones into the portal circulation which act on the anterior pituitary. What are the main examples of these hormones? |
Thyrotropin-releasing hormone (stimulates TSH and prolactin), GnRH, Corticotropin-releasing hormone (stimulates ACTH and prolactin), GHRH, somatostatin, dopamine (inhibits prolactin) |
|
|
At what point can spermatogonia type A arrest during the spermatogenic cycle? |
Any point, for 16 days. Then start again at first mitotic division |
|
|
What is the full pathway of sperm? |
Seminiferous tubules Rete testis Efferent tubules Epididymis Vas deferens Seminal vesicle joins Ejaculatory duct Prostate gland |
|
|
What are the main differences between a non-pregnant uterus and one at term? |
Weight (50-->950g), length (7.5-->30cm), depth (2.5-->20cm) and shape (flattened pear --> ovoid and erect) |
|
|
What is the normal value for uterine blood flow during pregnancy? |
500ml/min |
|
|
What is the function of CYP19 (aromatase)? |
Converts androgens (testosterone) to oestrogens (oestradiol) |
|
|
What is the function of prolactin? |
Stimulates milk production in mammary glands, breast growth. Suppresses ovarian function, has a role in sexual gratification |
|
|
Why do pregnant women experience morning sickness? |
Increased levels of progesterone relaxes smooth muscle in stoIncreased levels of progesterone relaxes smooth muscle in stomach wallmach wall |
|
|
What percentage of the adrenal cortex does the Zona Fasiculata comprise of, where is it located and what are its products? |
75% (contains large lipids), middle, cortisol and androgens |
|
|
What are the features of the anterior pituitary? |
Consists of endocrine tissue, known as adenohypophysis |
|
|
What is a spermatogonium? |
Undifferentiated male germ cell |
|
|
How long does each cell division take in spermatogenesis? |
Mitosis of spermatogonia to primary spermatocytes: 16 days. First meiosis to secondary spermatocytes: 24 days. Second meiosis for engendering spermatids: few hours. Spermiogenesis up to completed sperm cells: 24 days |
|
|
How does the position of the uterus change between non-pregnancy and term? |
Goes from anteverted and anteflexed in pelvic cavity --> rotated to the right in abdominal cavity |
|
|
What is the mechanism of the foetal component of uteroplacental blood flow? |
Once blood has obtained oxygen and nutrients it flow back to foetus through umbilical vein (oxygenated). Umbilical arteries transport waste - 2 arteries 1 vein |
|
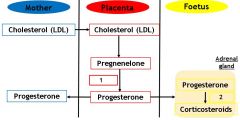
What is denoted by label 1 on this diagram of progesterone synthesis during pregnancy? |
3β-HSD |
|
|
Where are human Placental Lactogen (hPLK) and human Chorionic Sommatomammotropin (hCS) produced and how do their levels change through pregnancy? |
Produced by syncytiotrophoblast, produced from 5th week of pregnancy. Production increases with placental weight |
|
|
How do autocrine and paracrine cells communicate? |
Message diffuses in interstitial fluid - specificity depends on receptors |
|
|
What percentage of the adrenal cortex does the Zona Glomerulosa comprise of, where is it located and what are its products? |
15%, outer layer, aldosterone |
|
|
What are the features of the posterior pituitary? |
Neural origin, known as neurohypophysis. Consists of axons and nerve endings with cell bodies in the hypothalamus |
|
|
What is the purpose of the spermatogenic cycle? |
Process by which spermatogonia renew pool |
|
|
What is spermiogenesis? |
Maturation and motility of spermatozoa, involves dramatic cell repackaging |
|
|
What are the histological features of the cervix? |
Mainly collagen, some SM and elastin. Held together by connective tissue ground substance. SM concentrated near internal os (uteral-cervix border) |
|
|
How are amino acids, glucose and fatty acids transported to the foetus? |
Transporters (e.g. GLUTs, FATPs) expresed in both plasma membranes of the syncytiotrophoblast |
|
What is denoted by label 2 on this diagram of progesterone synthesis during pregnancy? |
CYP17 |
|
|
What is the structure and function of human Placental Lactogen (hPL) and human Chorionic Sommatomammotropin (hCS)? |
Similar structure and functions to hGH. Involved in breast development and lactation, anti-insulin effects, decreases maternal insulin sensitivity. Increases maternal free FA levels |
|
|
How much foetal lung fluid is present at birth? |
20ml/kg |
|
|
What does it mean if a receptor is high affinity? |
Hormones are effective at lower concentrations |
|
|
How do steroid hormones act on receptors? |
Bind to receptor, moving hinge region to expose DNA binding site - inhibitory protein complex leaves |
|
|
What are the three types of physiological response to hormones? |
Rapid (transporter protein activation/ inhibition) Short term (general metabolism, neurotransmitter synthesis/ release and receptor sensitivity) Long term (regulation of gene expression) |
|
|
What is spermatogenesis? |
Creation of a spermatozoa, meiotic division of spermatocytes to haploid spermatids |
|
|
What is spermiation? |
Release of spermatozoa from sertoli cells |
|
|
What are the main differences between a non-pregnant and a term cervix? |
Increase in mass, water content and vascularity (pink-->blue). Decreased elastin - deficient in incompetent cervix |
|
|
How are lipids transported from the mother to the foetus? |
Extracellular lipases release FAs from maternal lipoproteins, intracellular binding proteins (FABPs) guide FAs within the cytosol of the syncytiotrophoblast |
|
|
Progesterone stimulates most of the maternal adaptations to pregnancy. What are some examples? |
Reduces uterine contractability, stimulates breast secretory alveoli development, inhibits FSH and LH production, maintains endometrium, contributes to early embryo nutrition |
|
|
What produces human Choronic Gonadotropin (hCG) and how do levels change during pregnancy? |
Syncytiotrophoblast - first detectable 8-9 days after ovulation (pregnancy test). Rise first 8-10 weeks then fall to persistent levels at 20 weeks |
|
|
What are steroid hormones synthesised from? |
Cholesterol |
|
|
What are the main features of steroid hormones? |
Small hydrophobic molecules, released immediately, circulate in bound form, act on intracellular receptors, slow long lasting effects |
|
|
What are the features of amino acid hormones? |
Stored for instant release, different modes of action such as intracellular, cell-surface. Examples are thyroid hormone and epinephrine |
|
|
What is a spermatocyte? |
Type of germ cell |
|
|
What are the functions of endocrine category sertoli cells? |
Expression of hormone receptors, production of aromatase |
|
|
What are the ways in which myometrial contractions can be beneficial from a health perspective? |
Constrict placental bed blood vessels following delivery, expel secretions (reduces infections), and dangerous pregnancy tissue (intra-uterine death), ends pregnancy when mother at risk (pre-eclampsia, abruption, choramnionitis) |
|
|
What are the major determinants of gaseous exchange in pregnancy? |
Efficiency and flow of maternal and foetal circulation, surface area of placenta available for transfer, thickness of placental membrane |
|
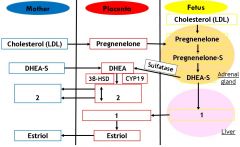
What is denoted by label 1 on this image of oestrogen synthesis during pregnancy? |
16OH DHEA-S |
|
|
What is the structure and function of human Chorionic Gonadotropin (hCG)? |
Structure/ function similar to LH. Prevents corpus luteum degradation, maintains decidual cells, responsible for morning sickness |
|
|
What are amino acid hormones synthesised from? |
Tyrosine |
|
|
What is the intermediate in the conversion of progesterone to aldosterone? |
Corticosterone |
|
|
What are the features of peptide hormones? |
3-332 amino acids long, synthesised as preprohormones, stored. Act on cell surface receptors then via 2nd messenger systems |
|
|
What is a spermatozoa? |
Motile haploid male gamete (sperm) |
|
|
What are the functions of exocrine category sertoli cells? |
Production of fluid to move immobile sperm out of testes, production of ABP, determination of rate of spermiation |
|
|
How does smooth muscle act differently in the myometrium? |
Actin filament interacts with entire length of myosin filament - in presence of Ca causes contraction or retraction (permanent shortening) |
|
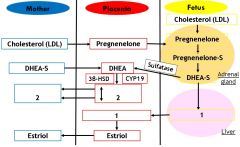
What two products are denoted by label 2 on this image of oestrogen synthesis during pregnancy? |
Estrone, estradiol |
|
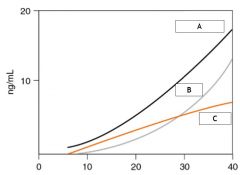
On this oestrogen hormone profile during pregnancy, which line represents estradiol? |
A |
|
|
What are the stages of cholesterol conversion to progesterone? |
Cholesterol --> 22α,22-Dihydroxycholesterol --> pregnenelone --> progesterone |
|
|
What substance is Oestradiol converted from? |
Testosterone |
|
|
What is Down's Syndrome? |
Trisomy 21 - 1:30 if mother >45, 1:1000 if 20-29. Overall risk 1:650. Usually screened by US and blood test at week 19/20. Ethical issues surrounding abortion |
|

What is denoted by label 1 on this image? |
Sertoli cell |
|
|
What are the functions of supportive/ nursing category sertoli cells? |
Junctions between sertoli cells, blood-testes barrier, phagocytosis, transfer of nutrients/ other substances |
|

At roughly how many weeks gestation would myometrial contractions produce the graph labelled C? |
36 |
|
|
What is the major substrate (90%) for oxidative metabolism in the foetus and why is this why is this % so high? |
Glucose - syncytiotrophoblast impermeable to disaccharides and sugar alcohols |
|
|
What is DHEA-S and where does it come from? |
Dehydroepiandrosterone sulfate - formed in adrenal gland. Also converted to 16OH version in foetal liver |
|
|
What are the functions of oestrogens during pregnancy? |
Stimulates SM growth of uterus by hypertrophy, stimulates proliferation of mammary ducts, inhibits FSH and LH, softens cervix and pelvic ligaments, stimulates synthesis of oxytocin receptors in uterus |