Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
40 Cards in this Set
- Front
- Back
|
What are some common causes of Hallux Abducto valgus?
|
Hypermobile 1st ray
Rheumatic inflammatory disease Neuromuscular disease Post-surgical malfunction Metarsus primus adductus Long First Ray Excessive pronation Gastroc Equinus Flexible forefoot valgus Limb length discrepancies Ehlers Danos Syndrome Pes Planus foot types |
|
|
When evaluating a patient History of CC concerning HAV, it is important to note what specific factors relating to pain?
|
Onset
Duration Progression Location |
|
|
In evaluating a runner w/ who presents w/ HAV, what other deformity is also likely to be present in hallux?
|
Hallux Limitus
|
|
|
If you are unsure of the vascular status of the patient, what exam would your order to have a definitive evaluation?
|
Arterial Doppler Exam
which provides ABIs Toe Pressures Segmental Pressures |
|
|
Normal 1st Ray position is how many degrees upon testing it for movement?
|
10 degrees
5 degrees up 5 degrees down |
|
|
How many degrees is the hallux sitting down in a plantarflexed 1st ray?
|
7 degrees
|
|
|
How does one test for transverse plane mobility?
|
Straighten out the hallux, and see if you can push the bump in.
In people who are very flexible/ or have a soft tissue deformity, the bump will go in. In an osseus deformity, the bump will not move. |
|
|
Metatarsal Cuneiform mobility is indicated for patients with severe HAV along with what foot type?
|
Flexible feet
|
|
|
Crepitus
|
Cartilage is destroyed
Bone is rubbing on bone |
|
|
Trackbound
|
Lateral soft tissue contracture & increase in the PASA
|
|
|
People with medial bunions generally have underlying ______________________
|
Metatarsus Adductus
|
|
|
Pinched tyloma's occur as a result of_________________________
|
Medial Bunions
|
|
|
How does one develop a tyloma under sub-met 1?
|
Pinched tylomas usually develop as a result of a biomechanical deformity.
If the tyloma is under the met head, then it is a result of a plantar flexed metatarsal. |
|
|
Name 5 reasons one can develop a tyloma (sub met 2)
|
Usually a structural abnormality of 1st ray
-Hallux limitus/rigidus -Hypermobile 1st ray -Hammertoe 2nd met, leading to functionally PF position -Contracted 2nd digit -Short 1st met -Long 1st met -Loss of hallux purchase |
|
|
Keller bunionectomies lead to what possible complication in regards to the hallux and its relationship to the ground?
|
Loss of hallux purchase to due instability of the intrinsic muscles
|
|
|
Other deformities seen with HAV deformities...include.....
|
Hallux IPJ deformity - causes the foot to look like it still has a bunion
EHL contracture - use lengthening procedure (Open Z) to correct this Bursa's |
|
|
In a patient with a bunion, when doing a WB exam, you notice when they stand their abductors fire causing the hallux to straighten out, what note would you want to make pre-op?
|
Slightly under correct otherwise this patient may go into hallux varus.
|
|
|
Normal passive DF of the 1st MPJ is_____________
|
20-30 degrees
|
|
|
The standard views for radiographic evaluation include:
|
AP, Lateral, MO, Ses Axial
|
|

Describe this bunion
|
There is increase in soft tissue density and volume along the medial aspect of the 1st MPJ
|
|
|
When evaluating a bunion radiographically, what 3 items should be described?
|
Soft tissue
Joints Angles |
|

Name this angle and how you derive it.
|

Standard Met Adductus Angle
Normal is < 15* Take the base of the medial cuneiform and draw a line to the base of the midpoint of the cuboid. Bisect the 2nd ray, and bisect the tarsus from that point. |
|

What angle is this?
And how do you derive it? |

Engles Angle.
Bisect the 2nd cuneiform & bisect the 2nd met. Normal is < /= to 24* Anything greater means they have met adductus!! |
|

What angle is this?
What's normal for this? |

Classic IM angle.
Normal is </= to 8* |
|

TRUE IM angle is calculated how?
and why? |

Calculated by taking the
(IM angle + Met adduct. angle) - 15* Indicated because IM angle alone does not account for underlying adductus |
|

What angle is this?
How do you calculate it? What is normal? |

Proximal Articular Set Angle
Normal PASA is 8*. Bisect the 1st met. Draw a line from medial to lateral across the effective articular cartilage. Angle is found by measuring the angle formed by the transverse articular cartilage line VERSUS a line perpendicular to the longitudinal bisection line. |
|

What angle is this?
What is normal? |

DASA
Normal is 8* or less. Formed by taking a longitudinal bisection of the proximal phalanx, and then drawing a line from medial to lateral for the transverse articular cartilage, and then.. MEASURING the angle by drawing a line perpendicular to the transverse articular cartilage line & the existing bisection of the prox phalanx. |
|

What angle is this?
What is normal? How do you measure it? |

Hallux abductus IP angle.
Normal is 10* or less. Measure by bisecting the prox phalanx and bisecting the dist phalanx. The degree of abduction of the distal phalanx from the prox phalanx is recorded as the HAIP angle. |
|
|
If the PASA +DASA = HAA, then it is what kind of foot deformity?
|
Structural Foot Deformity.
The joint status in this case is congruent. |
|
|
If the PASA+DASA<HAA, the it is what kind of foot deformity?
(HINT: NORMAL PASA/DASA) |
Functional Foot deformity.
The joint status in this case is deviated/subluxed. |
|
|
If the PASA+DASA<HAA, then it is what kind of foot deformity?
HINT: PASA/DASA ARE ABNORMAL!! |
It is a combination foot deformity, it is both structural & functional foot deformity.
The joint status in this case is deviated/subluxed. |
|

What is radiograph displaying?
|
The Met Protrusion distance.
Normal is +/- 2mm. |
|
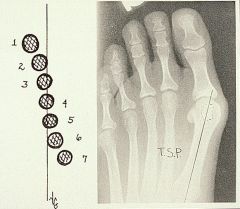
Explain how to use this to evaluate sesamoids.
What is considered normal? |
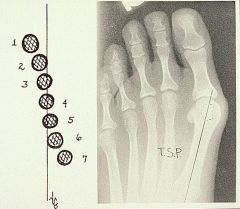
Bisect the 1st Met, and look for the tibial sesamoid.
Normal position is 1 to 3. Anything else is abnormal. Positions 4-7 indicate LATERAL tracking of the medial sesamoid. |
|

How would you evaluate 1st MPJ position?
|

A normal 1st MPJ position would be evaluated by looking at the position of the sesamoid and seeing that it is proximal to the metatarsal joint line.
|
|

A congruous joint is one in which the lines are ______________
|
A congruous joint is one in which the lines are running PARALLEL.
|
|
|
A deviated joint is one in which
the joint lines ____________________ |
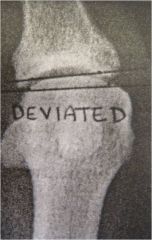
Intersect outside the joint!
|
|

Normal joint width is ?
|
2mm width is considered normal joint width
|
|

This is an example of a _______________
|
Subchondral bone cyst
|
|

The angle being displayed is measuring ______________
|
The first met declination.
Normal is up to 15* |
|

The shape of the 1st-met cuneiform jt shown here is round- which indicates you will need to do what kind of reduction?
|
Soft tissue reduction since ROUND 1st-Met Cuneiform Jts are soft tissue in nature.
Square/oblique require an osseus procedure. |