![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
41 Cards in this Set
- Front
- Back
|
What are the functions of the GI System? |
Ingestion Peristalsis (propulsion) Digestion (chemical and mechanical) Absorption Defecation The GI tract provides inorganic and organic substances to meet metabolic needs. Nutrients are extracted and absorbed; the residues are removed in the feces. The GI tract also has immunologic and otherprotective activities. |
|
|
The GI System is like a machine. Describe this parallels and how it relates to the GI function. |
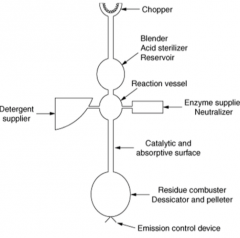
The GI system is a machine that carries out digestive,absorptive, immune, and excretory functions. |
|
|
Describe the general function of the: oral cavity, pharynx, esophagus, stomach, small intestines, and large intestines. |

|
|
|
How is fluid balanced in the GI tract and what are the possible contents? Where does the fluid come from? |
2 L water ingested + 7 L GI secretions 8.5 L reabsorbed in small intestine 500 ml enters colon +100ml excreted
Contents: Water Mucus Digestive enzymes Organic substances Protective substances Electrolytes The amount of material handled by the intestine is considerably greater than thevolume ingested.. Secretion occurs all along the GI tract. Water is secreted in the upper portion of the tract and reabsorbed inthe lower portion. Another major contributor is mucus, which serves a protective function for theepithelial surface all along the tract. Most of the mucus and some neutralizingfluids are secreted by cells or glands in the epithelial surface itself. |
|
|
Where are carbs, lipids, and proteins absorbed? Where is calcium, iron and folate absorbed? Where are bile acids and cobalamin absorbed? |

Duodenum is themain site ofdigestion oflipids, whilejejunum is themain site of lipidabsorption |
|
|
How are carbs, fats and proteins absorbed in the GI lumen? How are they digested? |

|
|
|
Digestion of Carbs |
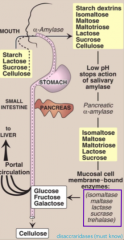
The principal sites of dietary carbohydratedigestion: mouth and intestinal lumen. The final products of carbohydrate digestion:monosaccharides: glucose, galactose andfructose, which are absorbed by cells of thesmall intestine. Salivary α-amylase acts briefly on dietarystarch and glycogen, hydrolyzing α(1-4)bonds. |
|
|
What is the function of glycosidase? |
to break glycosidic bonds |
|
|
We cannot digest cellulose. Why? |
beta 1,4 bonds |
|
|
What is Acarbose and what is its function? What are the key enzymes in digestion (generally) and what conditions can affect their secretion? |
-Used to treat type 2 diabetes -Slows down digestion of carbohydrates -Lengthens the time it takes for the digestion of carbohydrates -Keeps blood glucose from rising very high after meals Amylase activity in the gut is abundant and is not normally rate limiting forthe process of digestion. Alcohol-induced pancreatitis or surgical removal ofpart of the pancreas can decrease pancreatic secretion. |
|
|
What gene encodes alpha amylase? |
AMY1 gene that encodes for -amylase shows copy number variations High copy number of AMY1 gene correlate with regions which have high-starch diets (evolutionary adaption). |
|
|
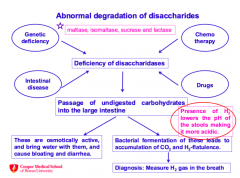
What are the main disaccharidases in the body? What causes a deficiency in disaccharidases? How does this effect the body (2 ways)? How can you measure abnormal degradation of disaccharides? |
|
|
|
Which ethnic groups present with lactose intolerance and what is the treatment? How does age affect the presence of lactase and what causes this? |
90% of adults of African or Asiandescent are lactase deficient. Adult hypolactasia: The age-dependent loss of lactase activityrepresents a reduction in the amountof enzyme rather than a modifiedinactive enzyme. It is thought to becaused by small variations in the DNAsequence of a region on chromosome2 that controls expression of the genefor lactase, also on chromosome 2. Reduce consumption of milk, or uselactase-treated products. |
|
|
Lactose is a disaccharide containing: |
Galactose and Glucose |
|
|
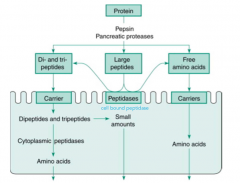
How is pepsinogen, a digestive protease, activated? Why does it need activation? What happens if pepsin is deficient? |
Pepsinogen is produced as a zymogen because it will break down everything if it is not inactive. Pepsin is produced by cleavage of 44 amino acid segment when the pH is below 5. Dietary molecules are digested by acid as well and 10-15% of proteins are digested by pepsin. If you have a pepsin deficiency, not significant. |
|
|
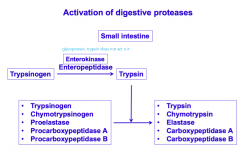
How is trypsinogen activated? What is the downstream affects of the activation? |
|
|
|
What is the fate of protein exposed to pepsin? |
|
|
|
How are amino acids absorbed? What cells are required? Be specific. |
Brush border • Amino acids are taken up by transporter facilitated passive diffusion and also bysodium coupled secondary active transport. • Di and tripeptides cotransport with H+ (powered by H+ gradient). H+ gradient ismaintained by Na-H exchanger. • Peptides appear to be absorbed faster and more efficiently. Basolateral • Either Na dependent or independent transpor |
|
|
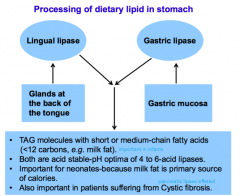
What happens to dietary lipids? What enzymes are involved and where are they located? In what disorder are these enzymes important and why? |
|
|
|
90% of dietary fat is _____________. |
90% of our dietary fat is TAG, remaining is cholesterol, cholesterol esters, phospholipids, unesterified (free) fatty acids. |
|
|
What is Orlistat? |
• Orlistat inhibits gastric and pancreatic lipases-decreasing fatabsorption and leading to weight loss. |
|
|
The majority of fat digestion occurs via_________. How are these enzymes unique, and in what disorder are they deficient. What products are formed by TAG metabolism? |
Majority of the digestion of the dietary fat occurs via the pancreatic lipase. TAGs are degraded by pancreatic lipase to 2-monoacylglycerol + two fatty acids • Pancreatic lipase is highly catalytically active and is present inhigh amount in pancreatic secretions, so unless there is adisorder such as CF, it is very efficient and ensures effectivedigestion of fat. |
|
|
How is fat emulsified? |
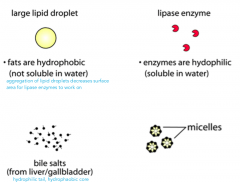
aggregation of lipid droplets decreases surface area for lipase enzymes to work on |
|
|
How is emulsified fat degraded? |
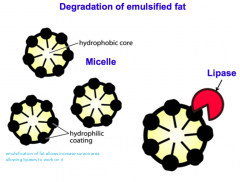
emulsification of fat allows increase surace area allowing lipases to work on it |
|
|
What is the importance of lipase? What about bile? How does fat in thee diet affect lymph flow? |

Majority of the fat in our diet (oreven in the milk for infants) istriacylglycerol (TAG). • Lipases are important for TAGdigestion. Bile is important for: Emulsification of fat Absorption of fatty acids Removing cholesterol from body Presence of fat in the diet wouldincrease the lymph flow from theintestine. |
|
|
How are fats absorbed? How does fat soluble vitamin fit in? |
|
|
|
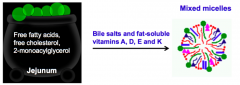
What is the function of mixed micelles? |
Mixed micelles can approach brush border membranes and releaselipid products, which enter cells by diffusion. |
|
|
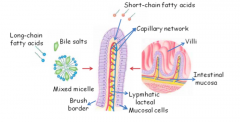
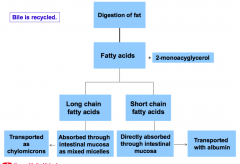
Describe the process of fat digestions and the fate of different types of Fatty acids. |
|
|
|
What happens to fat in the mucosal cells and what is the role of bile salt in fat absorption? Why is this important or fat soluble vitamins? |

Re-synthesis of triacylglycerols in intestinal mucosal cells Assembly and secretion of chylomicrons by intestinal mucosal cells Bile salt/mixed micelles mediated solubilization is important forthe absorption of fat soluble vitamins A, D, E and K. Fat digestion and absorption is thus important for absorption ofthese vitamins. Defect in fat absorption (for example,steatorrhea, fatty stools or bilary atresia) will result in deficiencyof these vitamins. |
|
|
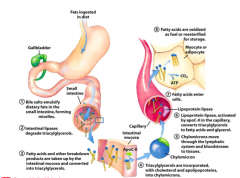
Describe the process of fat digestions in 8 steps, |
|
|
|
What is steatorrhea and what causes it? |

• Lipid malabsorption •Can be due to defects in bile secretion,pancreatic function or intestinal uptake oflipid. • Impacts on vitamin/essential fatty acid supply |
|
|
What is the role of TRPV-6 Ca2+ channel and calbindin? What is Vitamin D's role? How does calcium get out of the cells? |
Calcium entering the enterocytes through the TRPV-6 Ca2+ channel is bound by cytosolic calbindin. Transport out of the cell is via Ca2+ ATPase pumps and Na+ /Ca2+ exchangers. Vitamin D enhances Ca2+absorption by increasing calbindin production and Ca2+ pump activity. |
|
|
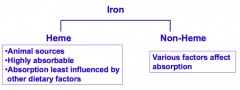
What is heme vs non-heme iron? |
|
|
|
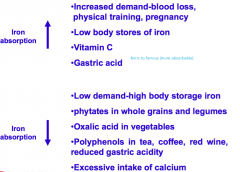
List 4 factors that increase or decrease iron absorption? |
|
|
|
How does iron absorption and distribution occur? |
|
|
|
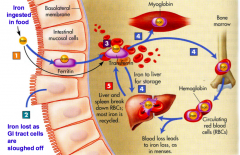
What is the role of ferritin and transferrin? How is iron absorbed, distributed, reused, and removed? |
1. Iron binds with a mucosal protein called ferritin in the intestinal cells. 2. If the intestinal cells are sloughed off before the iron is absorbed, the iron passes out of the body in feces. This sloughing allows the body to control the absorption of iron. 3. Iron that enters the bloodstream binds to transferrin. 4. Iron bound to transferrin is distributed to the liver, muscle,bone marrow and other body tissue. 5. The liver and spleen harvest iron from worn-out RBCs, thereby allowing most iron in the body to be reused. |
|
|
How is iron transported across brush border? What must occur to convert Fe3+ to Fe2+? How is iron exported and stored? |
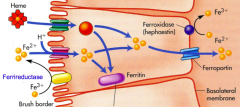
Heme iron is transported across brush border and enters the same pool as non-heme iron. Dietary non-heme iron (Fe3+)must be reduced for transport across the brush border by Ferrireductase. Ferroportin (along with transmembrane protein hephaestin)aids in export of iron out of theintestinal cell for incorporation intoserum transferrin. Some iron is used or stored within the enterocyte in ferritin and lost when the intestinal mucosa issloughed. |
|
|
Why is iron essential? |
Component of important proteins such as: •Hemoglobin-RBCs-carries oxygen to tissues •Myoglobin-muscles-controls oxygen uptake from RBCs •Cytochromes involved in release of energy from macronutrients to perform work Absence of which leads to fatigue-a major symptom of iron deficiency. |
|
|
What are the symptoms and signs of iron deficiency? |
•Fatigue •Sensation of feeling cold •Reduced work capacity and exercise tolerance •Affected neurotransmitter function, and immunologicand inflammatory defenses •Pica (compulsive eating of nonfood items) •Pagophagia (compulsive eating of ice) •Pallor, pale conjuctiva and spoon nails •Microcytic anemia (insufficient hemoglobinproduction, low numbers of new red blood cells) |
|
|
How is Vitamin B12 absorbed (mouth, stomach, small intestines, large intestines, etc)? Where is it absorbed and how is it transported? |
Absorption of vitamin B-12 is complex. • Mouth: Salivary glands produce R protein. • Stomach: HCL and pepsin release B-12 bound to protein in food. Free B-12binds to the R protein. Parietal cells release intrinsic factor. R protein (glycoprotein) protectsthe vitamin from acid degradation. • Small intestine: Trypsin releases R protein from B-12 and B-12 links with intrinsic factor (IF). This new complex is then absorbedby the epithelial cells of the ileum. • Ileum: Vitamin B-12 dissociates from IF and binds to transport protein transcobalamine II.The vitamin B-12-transcobalamine II complexenters the portal vein and is delivered to liver |
|
|
Defects in Vitamin B-12 absorption can be caused by different factors. List some of the main causes (i.e. molecular, immune, absorptive,) |
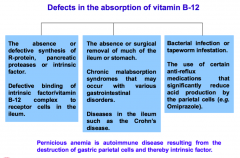
|