Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
14 Cards in this Set
- Front
- Back

After ORIF of long bone fx, at what time period should C-reactive protein start to decrease? 1-24 hrs; 2-48 hrs; 3-96 hrs; 4-7 dz; 5-12 dz
|

(CRP) should peak by 48 hrs p/ surgical fixation of bony orthopedic injuries, and decrease thereafter. an increasing CRP p/ 48 hrs is predictive for postop infection, and is more predictive in the first postoperative week than local erythema, persistent serous drainage, and increasing serial ESR.Ans2
|
|
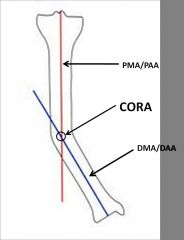
Which of the following is true regarding the center of rotation of angulation (CORA) as it refers to tibial diaphyseal angular deformity? 1-It is the point at which the prox mech axis and distal mech axis meet
2-It is the point at which the prox anatomical axis and prox mechanical axis meet; 3-It is always the point on the cortex at the most concave portion of the deformity; 4-It is the point at which the distal anatomical axis and distal mechanical axis meet 5-It is always the point on the cortex at the most convex portion of the deformity |
diaphyseal tibial deformity is defined as the intersection of the proximal mechanical(PMA) or anatomical axis(PAA), and the distal mechanical(DMA) or anatomical axis(DAA).Ans1
|
|

Hx:45yo F pedestrian is s/p MVA. xrays Fig A & B. What is the most important factor in determining between limb salvage and amputation? 1-Level of education; 2-Lack of plantar sensation; 3- Contralateral LE open fracture(s); 4-Severity of soft tissue injury; 5-Amount of tibial bone loss
|

clinical photo and radiograph are consistent with a Grade III open tibia fracture. The referenced study by the LEAP group reviews 527 patients with severe lower extremity fractures and found that the most important factor in determining the ability to salvage the extremity remains the severity of the soft tissue injury of that extremity. Bone loss has been shown to have no effect on the eventual outcome.Ans4
|
|

Hx:37yo M s/p closed injury figA. What technique can be utilized to avoid the characteristic deformity seen in this fracture pattern if an IM nail is used for Txt? 1- Med starting point; 2-Lat starting point; 3-Aiming the nail post in the prox segment; 4-Ant blocking screw in the prox segment; 5-Med blocking screw in the prox segment
|

characteristically is malreduced into valgus and apex ant (procurvatum) deformity, techniques to avoid these deformities are: provisional reduc w/ unicortical plates/clamps, semi-extended nailing, suprapatellar nailing, a more lat starting point, an external fixator or femoral distractor, blocking screws - posterior screw and/or a lateral screw in the prox segment, high rate of malalignment with nailing of this fracture pattern; 58% malalignment rate, 84% rate (>5 degrees in either coronal or sagittal planes).Ans2
|
|

Hx: 21yo M sustains the open injury Fig A, assoc w/ a 12 cm lac over the fx site. This lac is able to be closed during initial OR. What adjunct tx has been shown to improve outcomes when using an IM nail? 1-rhBMP-7
2-Adjunctive fx plating- 3-Ca phosphate; 4-Abx impregnated cement beads; 5-rhBMP-2 |
rhBMP-2 has been shown to have improved clinical outcomes in grade III open tibial fractures. rhBMP-2 is much more widely used clinically because it helps grow bone better than rhBMP-7 (OP1) and other BMPs, BMP-2 and BMP-7 are osteoinductive BMPs: they have been demonstrated to potently induce osteoblast differentiation in a variety of cell types. Ans5
|
|

Percutan placement of a lat prox tibial locking plate that extends down to the distl 1/3 of the leg is assoc w/ postop decr sensation of which of the following distributions? 1-Medial hindfoot; 2-Lat hindfoot; 3- First dorsal webspace; 4-Dorsal midfoot; 5- Plantar foot
|
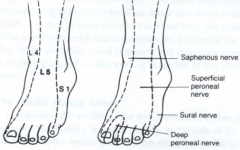
superficial peroneal nerve, sensory distribution to the dorsal foot. This risk is seen especially with percutaneous approaches, such as those used with the LISS plate.Ans4
|
|

Which of the following types of nonunions is most likely to achieve union following a reamed exchange
IM nailing only? 1-Dist fem nonunion w/ <10% bone loss; 2-Infected nonunion of the fem shaft; 3-Mid-diaphyseal humeral nonunion w/ <10% bone loss 4-Prox humeral shaft nonunion w/ <10% bone loss 5-Diaphyseal tibial shaft nonunion w/< 30% cortical bone loss |

Reamed exchange intramedullary nailing of diaphyseal tibial shaft fractures in which there is <30% of cortical bone loss can achieve union rates ranging between 76%-96%, Humerus nonunions, both diaphyseal and proximal locations, more readily achieve union with plate fixation and BG, use BG only when there is substantial bone loss, usually > 30% of the cortical diameter, distal femoral nonunions do not achieve union following exchange nailing. Ans5
|
|

What is the MC type of malalignment p/ IM nailing of dist 1/3 tibia fxs? 1-Varus; 2-Valgus; 3-Translational; 4-Rotational; 5-Apex anterior
|

tibial malrotation p/ reamed IM nail fixation as measured by CT. Malrotation = IR/ER deformity > 10 deg. (22%) of the tibia were malrotated > 10 deg and distal 1/3 fx.Ans4
|
|

Which is an advan of using blocking screws for tibial nailing? 1-< risk of nail breakage; 2-Eliminate use of interlocking screws; 3-Allow for larger nail use; 4- Enhance construct stiffness; 5-<torsional rigidity
|

Blocking screws can be used to help obtain and maintain reductions, increase construct stiffness, and neutralize translational forces, blocking screws, tibial healing was evident radiologically w/a decreased rate of malunions.Ans 4
|
|

What % of pts c/o of knee pain at the time of union of a tibial shaft fx treated with a reamed IM nail? 1. <10%; 2. 10-33%; 3. 33-50%; 4-50-75%; 5- >75%
|

67% of the transtendinous 71% of the paratendinous resulted in pts w/ postop ant knee pain, dropped down to 29% @ 8 yrs, but there was still no advantage of paratendinous over the transtendinous approach, knee pain was present in > 70%.Ans4
|
|

Hx:36yo M is s/p MVA. PE=deformed L LE w/ a 1-cm open wound over the anterolateral aspect of his leg. xrays Fig A & B. Which of the interventions decrease the occurrence of infection at the fx site? 1-Operative debridement w/in 6 hrs of injury; 2-Immediate prophylactic Abx; 3-Immediate stabilization w/ ORIF p/debrid; 4-Irrigating w/a saline solution that is mixed with an Abx; 5-Irrigating with high pressure pulsatile lavage p/surgical debrid
|

duration to beginning of antibiotic administration and adequate surgical debridement of all contamination are the only factors definitively shown to reduce infection and improve outcome. Traditional recommendations have suggested surgical debrid of open fx occur < 6 hrs of injury, However, there is NO literature to support this time window.Ans2
|
|

Hx: 56yo M sustains a Type IIIB open, comminuted tibial fx distal to a well-fixed TKA that is definitively tx w/ free flap & Ex fix 9 mths p/ fixator removal, c/o painful oligotrophic nonunion. Lab w/u for infection= (-) PROM =15 deg. What is the most appropriate tx for his nonunion? 1-Knee manip under anesthesia; 2- Cast immobilization & use of a bone stimulator; 3- Unilateral ex fix; 4-IM nailing; 5-Compression plating
|

At 9 months, observation is no longer an option, as the fracture is not healing and is adjacent to a arthrofibrotic joint. Plate osteosynthesis has been shown to be an effective method of treatment for patients who have had an open fracture of the tibia that has failed to unite after external fixation and/or immobilization in a cast.Ans5
|
|

Hx:54yo F s/p communited tibial shaft fx from an accident at work, s/p simultaneous ex fix and ORIF using minimally invasive plate osteosynthesis. p/ surgery, c/o numbness along the dorsum of her medial and lateral foot. In which location (labeled A - E) Figure A did percutaneous placement w/out careful dissection of a pin/screw likely cause her nerve injury? 1-A; 2-B; 3-C; 4-D; 5-E
|

post-op superficial peroneal nerve (SPN) palsy p/ ORIF of a tibial fx using both ex-fix and minimally invasive plate osteosynthesis (MIPO). The less invasive stabilization system (LISS) is a system which utlizes the MIPO technique. This minimally invasive technique can increase the risk of damage to the SPN w/out careful identification of the nerve distally due to its close proximity to LISS plate holes 11-13.Ans5
|
|

Which of the following techniques does not help prevent valgus angulation during IM nailing of prox 1/3 tibia fx? 1-Use of a blocking screw lat to midline in the prox segment; 2-Use of a blocking screw lat to midline in the distal segment; 3-Use of a lateral tibial nail starting point; 4-Use of supplementary plate and screw fix; 5-Use of a suprapatellar nailing portal
|

Several techniques are available to overcome this malalignment: proximal and lateral nail starting point, usage of a femoral distractor or temporary plating, suprapatellar nailing, and lateral parapatellar approaches, usage of blocking (Poller) screws - the referenced article by Ricci et al had 100% correction and maintenance of reduction with usage of blocking screws without other adjunct techniques. These should be placed in the lateral aspect of the proximal and distal fragments when needed.Ans5
|