Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
20 Cards in this Set
- Front
- Back

Ophthalmia neonatorum
(Slide 57) |

Conjunctivitis in newborn
Neisseria gonorrhoeae (first week), Chlamydia trachomatis (second week) |
|

Bacterial conjunctivitis
(Slide 57) |

Purulent conjunctivitis. Pain but no blurry vision
Pathogens: Staphylococcus aureus (most common), Streptococcus pneumoniae, Hemophilus influenzae (aegyptius, pink eye) |
|
Viral conjunctivitis
(Slide 58) |
Watery exudate
Adenovirus: viral cause of pink eye, preauricular lymphadenopathy HSV-1: keratoconjunctivitis with dendritic ulcers noted with fluorescein staining |
|

Allergic conjunctivitis
(Slide 58) |

Seasonal itching of eyes
|
|
|
Acanthamoeba conjunctivitis
|
Severe keratoconjunctivitis in patients who do not clean their contact lenses properly
|
|

Stye (hordeolum)
(Slide 59) |

Infection of eyelid most commonly due to S. aureus
|
|

Chalazion
(Slide 59) |

Granulomatous inflammation involving the meibomian gland in the eyelid
|
|

Orbital cellulitis
(Slide 60) |

Periorbital redness and swelling that is often secondary to sinusitis (e.g., ethmoiditis in children)
Pathogens: S. pneumoniae, H. influenzae Clinical: fever, proptosis (eye bulges out), periorbital swelling, ophthalmoplegia (eye movement impaired), normal retinal exam In cavernous sinus thrombosis, CN III-VI are impaired and the retinal exam is abnormal (papilledema) |
|

Pterygium
(Slide 60) |

Raised, triangular encroachment of thickened conjunctiva on the nasal side of the conjunctiva
Due to excessive exposure to wind, sun, and sand |
|

Optic neuritis
(Slide 61) |
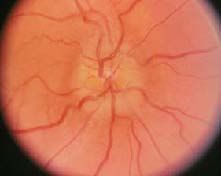
Inflammation of optic nerve
Pale disc Causes: multiple sclerosis (most common), methanol poisoning (see above discussion) Clinical: blurry vision or loss of vision, may cause optic atrophy |
|

Central retinal artery occlusion
(Slide 62) |

Causes: embolization of plaque material from ipsilateral carotid or ophthalmic artery; giant cell temporal arteritis involving the ophthalmic artery
Clinical: sudden, painless, complete loss of vision in one eye, pallor of optic disc, "boxcar" segmentation of blood in retinal veins |
|

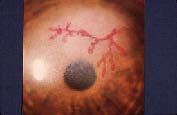
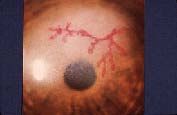
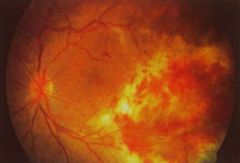
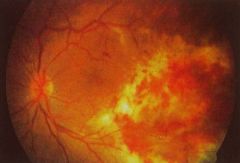
Central retinal vein occlusion
(Slide 62) |

Causes: hypercoagulable state (e.g., polycythemia vera)
Clinical: sudden, painless, unilateral loss of vision, swelling of optic disc, engorged retinal veins with hemorrhage |
|
Glaucoma
(Slide 63, 64, 65, 66, 67) |

Increased intraocular pressure
Chronic open angle type: decreased rate of aqueous outflow into the trabecular meshwork in the canal of Schlemm. Bilateral aching eyes. Pathologic cupping of optic disks. Night blindness and gradual loss of peripheral vision leading to tunnel vision and blindness. -blockers (e.g., timolol) decrease rate at which fluid flows into the eye. Acute angle-closure type: due to narrowing of anterior chamber angle causing decreased inflow of aqueous. Precipitated by mydriatic agent, uveitis, lens dislocation. Severe pain associated with photophobia and blurry vision. Red eye with a steamy cornea. Pupil fixed and non-reactive to light. Miotics (e.g., pilocarpine) increase the rate of fluid drainage from the eye. |
|

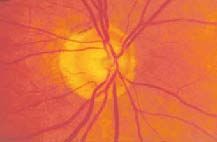
Optic nerve atrophy
(Slide 68) |

Pale optic disc
Most commonly due to optic neuritis or glaucoma |
|

Uveitis
(Slide 69) |

Inflammation of uveal tract (iris, ciliary body, choroid)
Causes: sarcoidosis, ulcerative colitis, ankylosing spondylitis Clinical: pain with blurry vision, miotic pupil, circumcorneal ciliary body vascular congestion, normal intraocular pressure, adhesions between iris and anterior lens capsule |
|
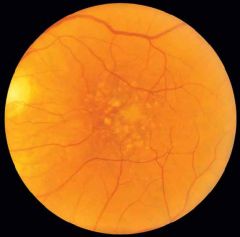
Macular degeneration
(Slide 70) |
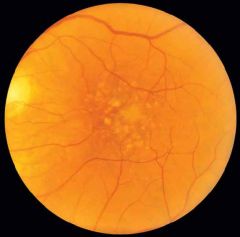
Most common cause of permanent visual loss in the elderly
Disruption of Bruch's membrane in the retina causing loss of central vision in one or both eyes Dry type (most common): begins with tiny deposits of a yellowish material known as "drusen" in the macula area; result in distortion, blurring of vision and gradual vision loss of varying degrees Wet type: severe progression of dry type; blood vessels from beneath the retina leak blood, pushing on the light receptor cells leading to damage of the macula Antioxidants decrease risk |
|
CMV retinitis
(Slide 71) |
Most common cause of blindness in AIDS. Usually occurs when CD4 T
Clinical: cotton wool exudates and retinal hemorrhages Rx: ganciclovir or foscarnet |
|

Cataracts
(Slide 72) |
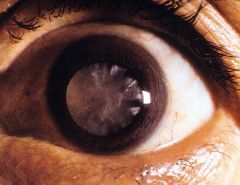
Opacity in the lens
Causes: advanced age (most common), diabetes mellitus (osmotic damage), infection (e.g., rubella), corticosteroids Common in congenital infections (e.g., CMV, rubella) |
|

Malignant tumors
(Slide 73) |

Retinoblastoma in children ("white eye reflex")
Malignant melanoma in adults CMV, cytomegalovirus; HSV, Herpes simplex virus; Rx, treatment. |
|
|
Methyl alcohol poisoning
|
methyl alcohol is present in window shield washer fluid, Sterno, and solvents for paints. It is converted into formic acid by alcohol dehydrogenase. This produces an increased anion gap metabolic acidosis due to the increase in formate anions. Bicarbonate is decreased because the H+ ions from formic acid are buffered by bicarbonate to form water and CO2. Formic acid damages the optic nerve causing optic neuritis and the potential for permanent blindness. IV infusion of ethanol decreases the metabolism of methyl alcohol, because alcohol dehydrogenase is preferentially metabolizing alcohol. Another treatment is the use of 4-methylpyrazole, which inhibits alcohol dehydrogenase.
|