![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
117 Cards in this Set
- Front
- Back
|
A CBC is a quantitative evaluation of ? A qualitative evaluation of? |
QuaNtitative evaluation of Leukocytes, RBCs, Platelets and total protein QuaLitative evaluation of cell morphology |
|
|
From an analyzer, a Raw count of your Leukocytes contain all of what? How do you get accurate information if your total WBC is not in normal range? |
Raw count includes ALL nucleated cells (includes nRBCs if present) If you take your percentage of WBCs and get an absolute count, this will give you accurate information. (A % of WBC is only accurate if the total WBC is WNL) |
|
|
Describe the function of each of these cells in inflammation: Neutrophil Lymphocyte Monocyte Eosinophil Basophil |
N- first responder, phagocytes L- immune function M- phagocytosis, organize inflammation, produce cytokines, present antigens E- immune responses, allergies- secondary phagocyte, inactive mediators from mast cells B- not usually seen- hypersensitivity reactions, attract eosinophils |
|
|
Neutrophils take how long to respond to inflammation? Describe the three different pools of neutrophils in bone marrow |
Take 5-7 days Proliferative pool- increases cell numbers Maturation pool- increases cell maturity (band neutrophils and metamyelocytes are here) Storage pool- fully mature, segmented cells |
|
|
What species has the greatest storage pool of neutrophils? Which has the least? |
Dog- most Cow- least (cat, horse are in the middle) |
|
|
What is the function of neutrophils? What regulates this? |
Dynamic changes between circulation and marginating pools Change in these numbers depends on selectins |
|
|
What does a left shift mean? Leukemoid response? |
A left shift is seen when band neutrophils are present. This is caused when the storage pool of neutrophils is depleted due to increased demand. Marked neutrophil response is a leukemoid response. |
|
|
Define a "toxic" neutrophil |
This is due to hurried maturation of neutrophils, not actually a response to toxins. Look for Dohle Bodies, bits of rER left in the neutrophil |
|
|
Lymphocytes primarily circulate as what? Describe their circulation patterns |
They circulate as T lymphocytes They can circulate between the tissues and circulation. This circulation depends on the rate and the production |
|
|
What is the function of a lymphocyte? |
Variable functions. They are seen in long standing inflammation Reactive lymphocyte- stimulated T or B cells |
|
|
If there is lymphoproliferation in bone marrow, what disease is seen in animals? |
Leukemia |
|
|
The different causes of lymphopenia are what |
Increase inflammation (decreased recirculation rate) Glucocorticoid Depletion Hypoplasia Lymphoma |
|
|
Describe the changes seen on a CBC that would reflect a stress leukogram (mediated by epinephrine) |
Neutrophilia and Monocytosis- due to demargination Lymphocytosis- due to increased recirculation rate |
|
|
Describe the changes seen on a CBC that would reflect a glucocorticoid response? |
Increased Neutrophils, increased monocytes Decreased lymphocytes |
|
|
What are the different stages of bone marrow production for a monocyte |
Monoblast -> promonocyte -> into circulation Once in tissues -> macrophages |
|
|
When looking at a blood smear, what do you evaluate on 10x magnification? |
Estimate the numbers of WBC and RBC Look for platelet clumps |
|
|
When looking at a blood smear, what do you evaluate on oil Immersion (100x) magnification? |
Within the optimal zone, look at the number, size, color, shape, inclusions and cell interactions of platelets, RBC, white cells |
|
|
Describe how you do a manual differential count with a blood smear What are the cells that you will see and how do you tell the difference between them? |
Count every intact WBC and classify it based on its characteristics. Then count until you have a total of 100 WBCs Neutrophils- most common, Monocyte- open chromatin, Eosinophil- red granules, lymphocytes |
|
|
How do you calculate the number of platelets in a blood smear? |
Count how many you see in a 100x field and then multiply that number by 15,000 |
|
|
The cytokine regulator of erythropoiesis is what? Where is it made? When is production stimulated? |
Erythropoietin Made in kidneys Production stimulated by hypoxia |
|
|
Name 5 things that erythrocyte concentration is dictated by |
Hydration Hemorrhage Destruction Production Spleen contraction |
|
|
When hemoglobin is degraded, what happens to each of the components? |
Globin parts are recycled as amino acids Heme group turned into bilirubin Iron is recycled (stored as hemosiderin) |
|
|
If you have decreased Hct, [Hgb], and [RBC] what do you call it. Increased? |
Decreased- anemia Increased- erythrocytosis |
|
|
When looking at plasma in a microhematocrit tube, what do you look at it for? |
If it is pink, you have free Hgb or hemolysis If it is yellow, you have icterus If it is lipemia, you have free triglycerides and it looks creamy |
|
|
How do you calculate Hct? |
(MCV) x [RBC]) / 10 |
|
|
[Hgb] is what? Units? Measured after what? |
Blood hemoglobin concentration (g/dL) Measured after RBC lysis in the analyzer |
|
|
[RBC] is what? Units? |
Concentration of RBC #/microliter |
|
|
MCV stands for what? What is its unit? |
Mean Cell volume fL |
|
|
What is MCHC? Units? If cell swells, what happens to MCHC? How do you calculate it? What is the normal MCHC level in a healthy animal? |
Mean Cell Hemoglobin concentration (g/dL) Cell swelling, MCHC decreases MCHC = ([Hgb] x 100) / Hct Should be about 1/3 of the Hct in a healthy animal |
|
|
What is MCH? How do you calculate it? If the cell swells, what happens to MCH? |
Mean cell Hgb (MASS) MCH = ([Hgb] x 10) / [RBC] If the cell swells, the MCH doesn't change |
|
|
What is CHCM? Is this a number available on all analyzers? Measured by? |
Cell hemoglobin concentration mean This is an advia analyzer # only Measured directly by light scatter |
|
|
Which is more reliable, MCHC or CHCM? |
CHCM |
|
|
What is RDW? This is a measurement of what? |
Red cell distribution width Variation of erythrocyte volumes (anisocytosis) |
|
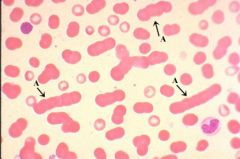
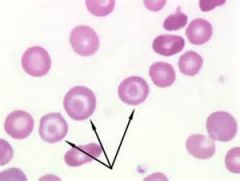
What general RBC feature is seen in this image? What causes it? |
Rouleaux Caused by an increase in plasma globulins due to inflammation, dehydration, multiple myelomas |
|
What general RBC feature is seen in this image? What causes it? What parameters on the CBC will this affect? |
Agglutination Caused by immunoglobulins bridging cells together (most likely found in IMHA) Will ruin all CBC parameters but the Hct and the Hgb concentration QA |
|
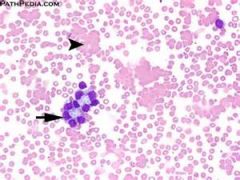
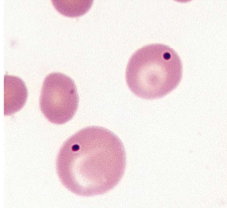
The two cells in the middle with the darker nuclei are what? What are the two different classifications of this condition? What will this affect on the CBC? |
Rubricytes (immature, nRBC) Appropriate- marrow is responding to erythropoietin Inappropriate- no marrow response seen This will alter the WBC count, you will need to correct all WBC parameters |
|
|
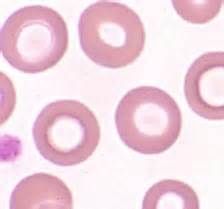
Central pallor is a normal phenomenon seen in which animal species (from order of most seen to least seen) |
Dogs Cattle Cats, Horses |
|
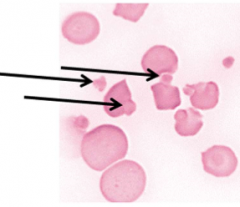
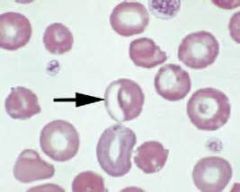
The three cells with the very fine pink perimeter are called what? What causes this condition? |
Ghost cells Caused by the leakage of Hgb out of the cells, commonly seen in IMHA |
|
|
What are the two things seen on a blood smear that helps you determine if IMHA is the diagnosis? |
RBC agglutination Ghost cells |
|
|
Hypochromic RBCs are cells with increased central pallor. What causes this condition? How does this condition reflect on a CBC? |
Iron deficiency anemia Decreased MCV, MCHC, MCH |
|
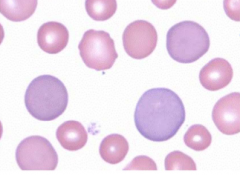
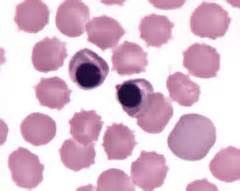
The darker purple cells are called what? This is a type of what? |
Polychromatophil An immature RBC, a type of reticulocyte |
|
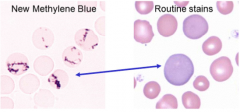
If you saw a polychromatophil that stained like this with NMB stain, what cell would you have? What is this best evidence of? |
This is a reticulocyte The stain with NMB is the RNA remaining in the RBC. This is best evidence for accelerated erythropoiesis (in all species but horses) |
|
|
How do you calculate a corrected WBC count? |
= [WBC] x 100 / (100+ nRBC per 100WBC) |
|
|
How soon after blood loss would you expect to see Reticulocytes? |
3-4 days |
|
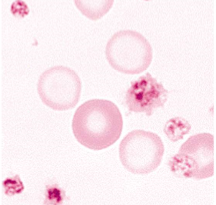
This is an example of what organism? What species would you see this in? |
Anaplasma marginale *note intracellular organism on the periphery of the cell Seen in cattle |
|

The organism seen in these RBCs are what species? |
Babesia Canis This is a protozoa, that affects many species |
|
The organism seen in these RBCs is what? |
Babesia Gibsoni |
|
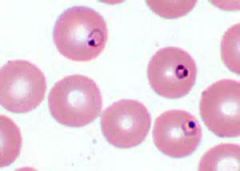
The organism seen in these RBCs is most likely what? What species can this affect? |
Mycoplasm *note that these live on the outside surface of the RBCs and form rings on the RBC Affect cows, dogs, cats and pigs |
|
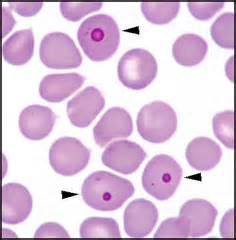
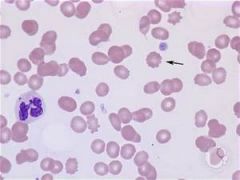
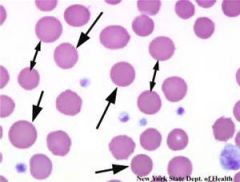
The arrows are pointing to what inclusion? What causes this? What can this lead to? |
Heinz bodies Caused by denatured hemoglobin from oxidative damage May lead to hemolytic anemia but, if they are found in a healthy cat that is normal |
|
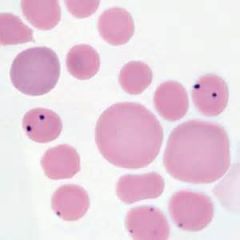
The inclusion seen in these RBCs are what? What causes this? How are these usually gotten rid of in a healthy animal? |
Howell-Jolly Bodies The dots are nuclear remnants left over from mitosis. Some of the causes of this include increased erythropoiesis, decreased splenic function, a splenectomy and certain drugs. These are usually removed by the spleen |
|
|
Define Anisocytosis. What CBC parameter will this change? |
Variation in volume/diameter of the RBCs Leads to an increased RDW |
|
|
Having macrocytes/microcytes will change what parameter on a CBC? What causes each of these different types of cells? |
MCV will be increased with Macrocytes and decreased with microcytes Macrocytes occur after increased erythropoiesis Microcytes are from iron deficiency and hepatic diseases |
|
|
What are all of the RBC changes you would see with iron deficiency? |
Microcytes Hypochromasia Keratocytes Schizocytes Codocytes |
|
|
What are all of the RBC changes you would see after oxidative damage? |
Heinz bodies Eccentrocytes |
|
|
Define Poikilocyte |
Abnormally shaped erythrocyte (use more specific terms though) |
|
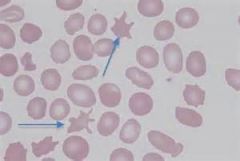
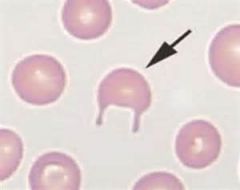
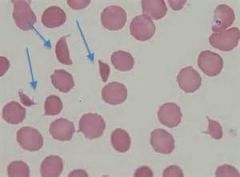
The arrows are pointing to what type of RBC shape change? What causes this change? |
Acanthocyte Splenic infiltrates and hemangiosarcoma causes this abnormal membrane |
|
The arrows are pointing to what type of RBC shape change? What causes this change? |
Eccentrocyte Oxidative damage |
|
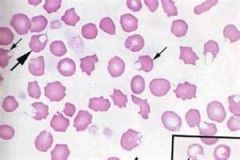
The arrows are pointing to what type of RBC shape change? What causes this change? |
Echinocyte Most often an artifact but can also be caused by dehydration, some drugs and rattlesnake bites |
|
The arrows are pointing to what type of RBC shape change? What causes this change? |
Keratocyte or "horn cell" Turbulence, angiopathy and iron deficiency cause these |
|
The arrows are pointing to what type of RBC shape change? |
Pre-keratocytes |
|
The arrows are pointing to what type of RBC shape change? What causes this change? |
Schizocyte or "fragment" Trauma, fibrin strands, intravascular coagulation, vasculitis, hemangiosarcoma, iron deficiency |
|
|
What are all the changes you would expect to see on a blood smear with an animal that had IMHA? |
Agglutination Ghost cells Spherocytes |
|
|
What are some causes of rubricytosis? |
Marrow damage Extramedullary hematopoiesis Splenic contraction Splenectomy Lead poisoning |
|
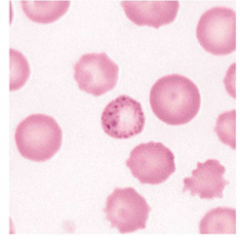
What Inclusion change is seen in this RBC? What causes this? |
Basophilic stippling (aggregated ribosomes) Regenerative anemia Lead poisoning |
|
The arrows are pointing to what type of RBC shape change? What causes this change? |
Spherocytes IMHA from the loss of part of the membrane by macrophages |
|
The arrows are pointing to what type of RBC shape change? What causes this change? |
Torocytes Drying artifact, not usually pathologic |
|
|
Anemia causes what things to be lowered on a CBC? What are the three general classifications of anemia? |
Hct [Hgb] [RBC] Blood loss, hemolysis, decreased production |
|
|
If an anemia is regenerative, what is present on a blood smear? If an anemia is regenerative, what catetogy/ies of anemia is most likely the cause? What if it is non-regenerative? |
Reticulocytes Regenerative- most likely blood loss or hemolysis Non-regenerative- most likely to do decreased/absent production of RBCs |
|
|
What are some of the causes of reduced erythropoiesis? |
Inflammatory diseases Renal disease Disease causing marrow hypoplasia/aplasia such as infectious agents, toxicosis and marrow neoplasia Disease causing selective erythroid hypoplasia/aplasia such as pure red cell aplasia, FeLV induced erythroid hypoplasia, endocrine disease, liver disease/failure |
|
|
What are some of the causes of defective erythropoiesis? |
Iron Deficiency IMHA FeLV-induced erythroid neoplasia |
|
|
On a CBC, what does MCV tell you about the animal's anemia? MCHC/CHCM? |
MCV- macro/microcytic anemia MCHC/CHCM- hypo/hyperchromic anemia (*note, hyperchromicshould be ignored, it is most often an artifact) |
|
|
What are the two pathophysiologic ways that blood loss anemia can occur? |
External- through the urinary or alimentary tract Internal- into the peritoneal and pleural spaces |
|
|
What are the two pathophysiologic ways that Hemolytic anemia can occur? What does each of them cause as far as other abnormalities in the blood? |
Extravascular- RBC destruction in the tissues ~Causes icterus and hyperbilirubinemia Intravascular- RBC destruction in the vasculature ~Causes Plasma hemolysis and hemoglobinuria |
|
What shape change is seen in these RBCS? That commonly causes this? |
Codocyte Shape caused by excess membrane These cells are seen in regenerative anemia, portosystemic shunts, lipid disorders and Iron Deficiency |
|
|
Describe some of the ways you can distinguish between a band and a segmented neutrophil on a blood smear |
If there is focal narrowing anywhere on the nucleus, it is a segmented neutrophil. If there is a smooth nucleus with no constriction or if it is a gradual nuclear narrowing, look at the chromatin. If the chromatin is dense, it is a segmented neutrophil. If it is less dense, it is a band neutrophil. |
|
|
With severe hemolysis, what two CBC parameters are unreliable? Why? |
MCHC and MCH Free Hgb that is in the vasculature is measured as Hgb that is in the RBCs. |
|
|
What are the four general categories of hemolytic disorders and what are some of the more specific causes of each? |
Immune- Idiopathic, drugs, neonatal infections Infections- Mycoplasma, Anaplasma, Leptospira, Clostridium, Babesia Metabolic defects- Oxidative injury, Defective ATP generation Erythrocyte Fragmentation- Turbulence, hemangiosarcoma |
|
|
Explain the pathophysiology behind: Anemia due to Inflammation |
Ex. Chronic pneumonia -> Release of inflammatory cytokines -> production of hepcidin in the liver -> Ferroportin is internalized in bone marrow and epithelium in the Small intestine -> Fe is sequestered, decreasing the uptake of Fe from the gut -> Erythropoiesis is decreased -> anemia |
|
|
How does anemia from inflammation usually look when evaluating the anemia for indices? |
Normochromic Normocytic |
|
|
What direct effect can inflammatory cytokines have on erythropoiesis? |
Inflammatory cytokines can directly decrease erythropoietin production from the kidneys, leading to decreased erythropoiesis |
|
|
Explain the pathophysiology behind: Anemia due to Renal failure |
Decreased functional renal mass -> decreased erythropoietin -> decreased erythropoiesis Decreased functional renal mass also -> decreases the clearance of hepcidin -> decreasing the Fe available -> decreasing erythropoiesis |
|
|
Explain the pathophysiology behind: Spherocytes -> anemia |
Macrophages partially or fully phagocytize RBCs -> Hgb leaks out of holes placed by the MAC complex -> RBCs are fragile -> RBC lysis -> anemia |
|
|
Explain the pathophysiology behind: Plasma hemolysis leading to hemoglobinuria |
MAC Complex attacks RBCs, leading to ghost cells -> Haptoglobin binds to cell to get recycled -> liver -> Fe is recycled, haptoglobin is used up. Not enough haptoglobin + too many ghost cells -> dimers appear in urine -> hemoglobinuria |
|
|
Complete the statement: __________ + ______________ = intravascular hemolysis |
Pink urine + hemoglobinuria |
|
|
Explain the pathophysiology behind: Hemolytic anemia -> Reticulocytosis |
Anemia -> renal hypoxia -> increased Epo -> Reticulocytosis |
|
|
Explain the pathophysiology behind: Anemia -> Rubricytosis |
Increase in Epo -> nRBC release -> appropriate rubricytosis Severe anemia -> marrow hypoxia -> damaged bone marrow -> inappropriate rubricytosis |
|
|
If you didn't have agglutination present, what test can you use to test for IMHA? What does this test detect? What other CBC characteristic is usually present with IMHA? |
Coomb's test, measures IgG, IgM on the RBCs A leukogram is common with IMHA |
|
|
Explain the pathophysiology behind: Anemia due to EIAV |
EIAV -> Immune complexes on the RBCs -> complement activation -> Extravascular and Intravascular hemolysis -> anemia -> Renal hypoxia -> Increased Epo -> Increased Erythropoiesis -> Macrocytosis |
|
|
Explain the pathophysiology behind: |
Immune complexes -> phagocytized by macrophages -> increased bilirubin as a byproduct -> Increased in unconjugated bilirubin= indirect hyperbilirubinemia -> conjugated in liver -> escapes into urine -> direct hyperbilirubemia *rate limiting step = excretion of conjugated bilirubin |
|
|
What are the other rule-outs for macrocytic anemia in horses? |
Regenerative anemia Cell swelling (artifact)- prolonged storage, hypernatremia Agglutination (artifact)- Immune mediated, heparin induced |
|
|
If you were trying to decide if an animal's anemia was hemolytic or due to blood loss, what are some of the things that would point you toward hemolytic? |
Regenerative anemia (unless it's pre-regenerative) No hypoproteinemia Hyperbilirubinemia and Bilirubinemia (without liver disease) Pink/Red Plasma/Serum Hemoglobinuria Blood Film Findings- organisms, heinz bodies, spherocytes, eccentrocytes |
|
|
Explain the pathophysiology behind: Anemia due to PK deficiency What test do you use to confirm this diagnosis? |
Decrease in PK -> Decrease in ATP -> decrease in cell viability -> Increase in EPO -> Reticulocytosis PCR |
|
|
Where is most of the iron found in the body? Of the Fe in the plasma, most of it is bound to what? On a chem profile, the Fe there is mostly what? Serum [Fe] is usually a good estimate of? |
1/2-2/3 of the Fe is in the RBCs, of the Fe in plasma, most of it is bound to transferrin Fe on a chem profile is mostly transferrin Fe (not a good estimate of total body Fe) The serum Fe is a good representation of the total body Fe |
|
|
What are some causes of Hyperferremia? Hypoferremia? |
Hyperferremia: Excess intake, hepatocyte damage, glucocorticoids Hypoferremia: Fe deficiency, inflammation, dexamethasone (cattle) |
|
|
Describe the pathophysiology behind erythrocytosis |
An increase in Hct -> Transient or EPO dependent reaction transient: a. physiologic erythrocytosis -> splenic contraction b. Hemoconcentration -> dehydration, endotoxic shock EPO dependent: a. Primary erythrocytosis- overproduction of RBC line only (neoplasia) b. Secondary erythrocytosis- ~with hypoxia- appropriate (cardiac disease, pulmonary disease, hyperthyroidism) ~without hypoxia- inappropriate (renal neoplasia, non-renal neoplasm that is making Epo, renal cyst) |
|
|
What clinical signs would you expect to see with Erythrocytosis? How would you test for it? |
Red mucous membranes Weakness (due to tissue hypoxia) Mucosal/Retinal bleeding Seizures Imaging and PE for CV disease, arterial blood gas to look for hypoxia |
|
|
Explain the pathophysiology behind Erthrocytosis leading to tissue hypoxia
|
Erythrocytosis -> increased blood viscosity -> Decreases blood flow -> decreases tissue oxygenation |
|
|
What is the cell lineage of a platelet? Eosinophil? Basophil? |
Platelets come from megakaryocyte Eosinophils and basophils from myeloblasts |
|
|
Describe the Erythrocyte lineage |

Rubriblast -> Prorubricyte -> rubricyte -> metarubricyte -> polychromatophil -> RBC |
|
|
Describe the Neutrophil Lineage |

Myeloblast -> Promyelocyte -> myelocyte -> metamyelocytge -> bands -> segmented neutrophils |
|
|
B lymphocytes go where to mature? T lymphocytes? |
B- lymphoid tissue T- Thymus |
|
|
Why do we look at bone marrow? |
To explain persistent cytopenia, -cytoses, atypical cells in the blood, hyperglobinemia, hypercalcemia To look for metastatic neoplasias or other specific bone marrow diseases |
|
|
How do we collect bone marrow? |
1. Aspiration- good for cell detail, cell identification, dysplastic changes, other organisms 2. Core cutting- good for histology, better architecture for focal lesions or myelofibrosis |
|
|
Where do we commonly collect bone marrow for evaluation? |
Wing of ileum, crest of ileum, proximal humerus, sternum of small animals Also ribs in large animals |
|
|
The normal cellularity in the bone marrow should be what percentage? |
25-75% |
|
|
What are the 4 things you want to evaluate when looking at bone marrow? |
Megakaryocytes (number and maturity) M:E Ratio (should be 1:1 or 2:1) Look for abnormal cells, cell types or organisms Look for Fe presence (except in healthy cats where it should be absent) |
|
|
The myeloid cells are what lineages? Erythroid? |
Myeloid- granulocyte and monocyte Erythroid- ALL nucleated RBCs |
|
|
What are the three ways you can have hypercellular marrrow? |
Increased M:E- Increased myelocytes with or without a change in erythrocytes Decreased M:E- Increased Erythrocytes with or without a change in Myelocytes No change in M:E- Both Myelocyte and Erythrocyte hyperplasia |
|
|
What are the three ways you can have hypocellular marrow? |
Increased M:E- Decreased Erythrocytes with or without a change in Myelocytes Decreased M:E- Decreased Myelocytes with or without a change in erythrocytes No change in M:E- Myeloid and Erythrocyte hypoplasia |
|
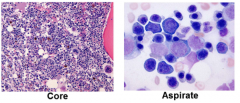
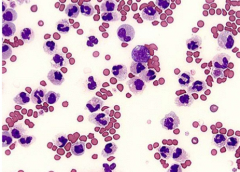
What is your interpretation of this bone marrow? what would your causes be? |
Erythroid Hyperplasia Effective- regenerative anemia Non-effective- Nonregenerative anemia (immune disorders or nutrition deficiencies) |
|
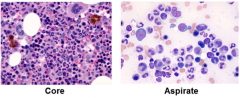
What is your interpretation of this bone marrow? what would your causes be? |
Granulocyte Hyperplasia Effective- Neutrophilia Ineffective- Neutropenia (immune disorders, drugs) |
|
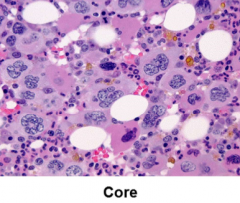
What is your interpretation of this bone marrow? what would your causes be? |
Megakaryocyte hyperplasia A response from thrombocytopenia |
|
|
If you had generalized hypoplasia in the bone marrow, what causes would you suspect? |
Infections Toxicosis Marrow replacement Idiopathic |
|
|
If you had selective erythroid hypoplasia in the bone marrow, what causes this? |
Chronic renal failure Inflammation PIMA |
|
|
If you had lymphocytosis in the bone marrow, what causes this? Myelofibrosis? |
Lymphocytosis- Inflammation Neoplasia (increase in lymphocytes or plasma cells) Myelofibrosis- PIMA |
|
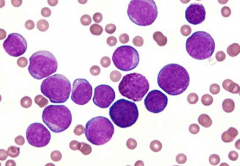
Classify and define how this change in the bone marrow occurs |
Acute leukemia Rapid proliferation of poorly differentiated cells |
|
Classify and define how this change in the bone marrow occurs |
Chronic leukemia Slow accumulation of well-differentiated cells |