Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
48 Cards in this Set
- Front
- Back
|
Four basic x-ray densities
|
Air
Fat Water Metal (calcium) Dense objects as white, more easily penetrated as gray/black. |
|
|
Basic x-ray density descriptions
|
Radiopaque
Radiodense Radiolucent Opacity - white Lucency - black |
|
|
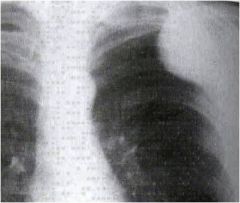
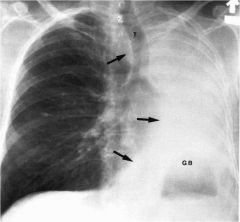
Penetration
|

Faint visualization of the intervertebral disc spaces of the thoracic spine
Discrete branching vessels can be identified through the cardiac shadow Images can be under or over penetrated. Shown: underpenetration |
|
|
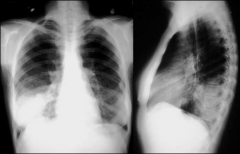
Rotation
|
There should be equal distance between clavicular heads and spinous processes.
If wider on one side, patient is rotated. Anterior structures move in the same direction as the patient is rotated and posterior structures move in the opposite direction. |
|
|
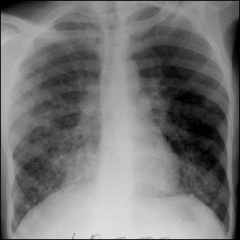
Inspiration
|
An appropriate deep inspiration in a normal individual is present when the apex of the right hemidiaphragm is visible below the 10th posterior rib.
- Count 8-10 ribs Poor inspiration can mimic infiltrates on lungs and be confused for pneumonia. |
|
|
Motion
|
The cardiac margin, diaphragms and pulmonary vessels should be sharply marginated in a completely still patient who has suspended respiration.
|
|
|
Where are the most commonly missed pathologies located?
|
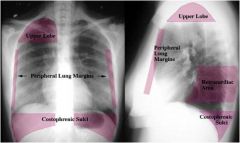
Right upper lobe
Other areas include retrocardiac, peripheral lung margins and posterior costophrenic sulci. Rib fractures - pleuritic pain PE - increased D dimer |
|
|
What is the best approach to take when reading an image?
|
A systematic approach
Look at various structures in a deliberate order, concentrating on the anatomy of each while excluding the superimposed shadows of other structures |
|
|
Lobes of the lungs
|
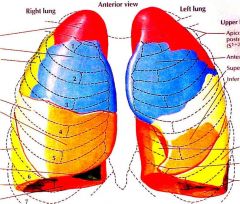
Right lung - 3 lobes
- RUL - 3 segments - RML - 2 segments - RLL - 5 segments Left lung - 2 lobes - LUL - 4 segments - LLL - 4 segments Lingula of left lung is analogous to RML. |
|
|
Lung fissures
|
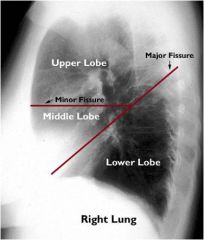
Fissures - best visualized on lateral
- Major separates upper from lower lobes - Minor separates RUL from RML - Azygos (0.5%), accessory |
|
|
Azygos fissure
|

Normal variant
Can resemble right apical mass |
|
|
Pseudotumors
|
Fluid in fissures that can be mistaken for tumors.
|
|
|
Frontal cardiac view
|

Right cardiac border - right atrium
Left cardiac border - left ventricle The SVC forms a right paramedian border |
|
|
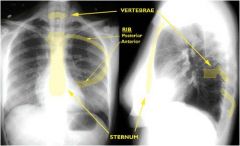
Lateral cardiac view
|
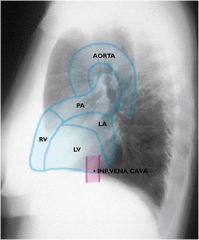
Anterior cardiac border - right ventricle
Posterior cardiac border - LV and LA The IVC is seen best on lateral projection. The posterior border is evident in contrast to the air-filled lungs. Left ventricular hypertrophy can be seen as enlargement on lateral view. |
|
|
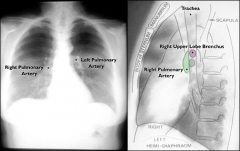
Hila
|
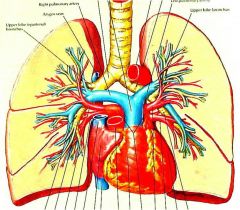
Pulmonary arteries, veins & airways
- Airways do not produce significant shadows therefore the majority of detectable structures are vascular. Left Pulmonary Artery - Courses over left upper lobe bronchus - Directed posterolaterally - On lateral, behind tracheal air column Right Pulmonary Artery - Courses beneath right upper lobe bronchus - Directed horizontally - On lateral, anterior to tracheal air column |
|
|
Hilar relationship
|
70% left hilum higher than right
30% hila equal Right NEVER higher than left |
|
|
Pulmonary veins
|

More horizontal
Best seen on lateral Don’t confuse with retrocardiac space or infiltrate |
|
|
Aortopulmonary window
|

A “space” located below the aortic arch and above the left pulmonary artery, bordered by aortic valve.
Normally contains fat An opacified window is a “red flag” If window not present, could indicate an aortic dissection or MI. |
|
|
Hilar lymphadenopathy
|

If right is higher than left, it can indicate a mediastinal lymphadenopathy.
|
|
|
Mediastinum anterior
|
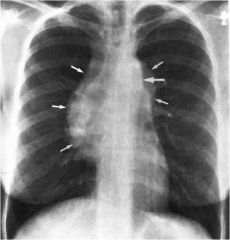
4 Ts
- terrible lymph nodes - thymus (thyoma) - thyroid (substernal goiter) - teratoma (shown) |
|
|
Mediastinum middle
|
Heart, vessels, lung root
- lymph nodes - congenital cysts - diaphragmatic hernias - vascular lesions |
|
|
Thymus
|

Sail sign may be present in pediatric patients.
|
|
|
Medistinum posterior
|
Esophagus, aorta
- neurogenic tumors - esophageal lesions - vertebral lesions - congenital cysts |
|
|
Diaphragm
|
Sharply marginated domes with the apex approximately mid-clavicular
Peripheral margins define the costophrenic sulci Right diaphragm higher than left due to position of the liver Always look below the diaphragm |
|
|
Costophrenic sulci
|
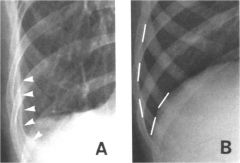
Sharp, costophrenic angles
- Rounded angles could indicate pleural effusion. |
|
|
Laterally dispaced diaphragm
|

Apex of diaphragm laterally displaced due to subpulmonic effusion.
|
|
|
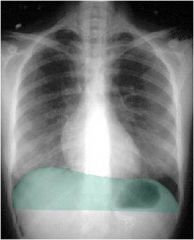
Air under diaphragm
|
Air under the diaphragm is an ominous sign that should not be overlooked.
Any gas should have an outline of visceral structure. Chilidi's sign - colonic interposition |
|
|
Diaphragmatic rupture
|

Traumatic diaphragmatic rupture (mimics a pleural effusion).
|
|
|
Trachea
|
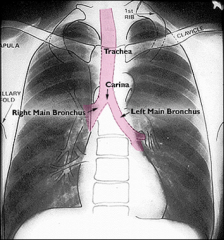
Look for deviations, may indicate pneumothorax.
|
|
|
Osseous structures
|
Bony structures
|
|
|
Metastatic disease
|

Ivory vertebral body
|
|
|
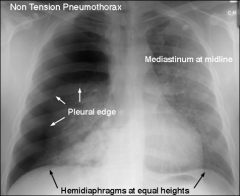
How to distinguish skin folds from abnormalities
|

Pneumothorax or skin fold?
- Second view – inspiratory/expiratory views - Hyperlucent lung – mastectomy may appear this way |
|
|
Silhouette sign
|

When two structures (opacities) of similar density abut one another, anatomical margins are lost.
|
|
|
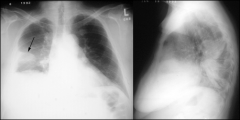
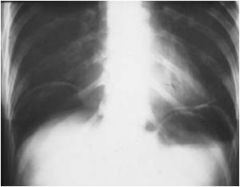
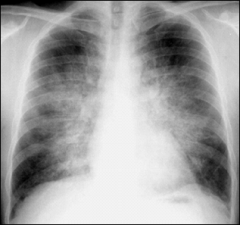
Air bronchogram
|

Indicates air space disease with fluid density outlining the air-filled bronchi.
Shown: right middle lobe pneumonia |
|
|
Extrapleural sign
|
A mass outside the pleural space has characteristic, smoothly sloped margins.
|
|
|
What should you examine when looking at lungs on an image?
|
Are they expanded to the periphery?
Symmetry Status Patterns of parenchymal opacity - air space (alveolar) - interstitial - atelectasis - nodule/mass |
|
|
Air space disease
|
Produced when air in terminal air spaces is replaced with “stuff”
Radiographic characteristics - lobar or segmental distribution - fluffy margins - tendency to coalesce - air bronchograms - rapidly changing over time - “bat wing” distribution Acute - blood - pus - fluid Chronic - lymphoma - TB - proteinosis |
|
|
Interstitial disease
|
Produced by processes that thicken the interstitial compartments
- water, blood, tumor, cells, infection, fibrosis Radiographic patterns - linear - reticular - reticulonodular - nodular - “ground glass” - curly B lines Acute - interstitial edema, viral/atypical Chronic - multitude (CHF) |
|
|
Atelectasis
|
Obstructive
- oxygen reabsorbed - mucus plug / F.B. / tumor Passive - mass effect / pleural - pleural effusion Compressive - mass effect / lung - bulla, tumor, abscess Cicatricial - scarring & retraction - TB, fibrosis Adhesive - surfactant deficiency - R.D.S. of Newborn |
|
|
Signs of volume loss
|
- movement of lobar fissures
- crowding of the lung markings - ribs more closely spaced - elevation of the hemidiaphragm - mediastinal shift - tracheal shift - consolidation |
|
|
Projectional phenomenom
|
Anterior objects appear larger
Can mimic congestive heart failure When you lie down, vessels compressed |
|
|
Pleural effusion
|
Fluid layering on film
|
|
|
Sulpulmonic effusion/mass
|
Diaphragm raised on one side
- Rule out phrenic nerve paralysis - Can be normal variant |
|
|
Consolidation
|
Very dense, masslike
Acute - Pneumonia - Blood - Atelactesis Chronic - Lymphoma - BAC (bronchioloalveolar carcinoma cell) Order follow up x-ray to see if consolidation has cleared |
|
|
Pulmonary edema
|
Hilum thickening
Interstitial thickening - Perpendicular lines can be seen – curly B lines - Also seen in CHF Fluid spills over and can be seen on periphery Can then develop a pleural effusion Cardiogenic – enlarged heart – CHF |
|
|
How do you distinguish between an atelectasis and pneumothorax?
|
Volume loss results from atelectasis
Subsegmental atelectasis - non-pathological How do you discern between atelectasis and another problem? - Volume loss - Trachea, mediastinum displace towards opacity |
|
|
Medistinal widening
|
With pain – CT to rule out aortic dissection
Use contrast to light up vessels - Pulmonary embolism - Any traumatic setting - Unless contraindicated |
|
|
Deep sulcus sign
|
Secondary sign of pneumothorax
|