![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
|
What is the most common gynecologic malignancy in the US? |
Endometrial (uterine) cancer |
|
|
What is the most common gynecological malignancy worldwide? |
Cervical cancer |
|
|
What type of cells make up the exocervix?
What type of cells make up the endocervix?
What is the junction between the two called? |
Exocervix → squamous epithelium
Endocervix → glandular/columnar epithelium
Junction → transformation zone (where dysplasia/malignancy develops) |
|
|
How is HPV usually eradicated? |
Infection is usually eradicated by the immune system -see more aggressive disease in women with a compromised immune system → these patients need to be more aggressively treated and have closer follow up |
|
|
What is a risk of persistent HPV infection? |
Leads to increased risk for cervical dysplasia (CIN) and cervical cancer
Risk of transformation depends on type of HPV |
|
|
What types of HPV leads to condyloma (typically not a premalignant condition)?
What types of HPV lead to dysplasia/malignancy? |
Low risk types: HPV 6, 11
High risk types: HPV 16, 18, 33 |
|
|
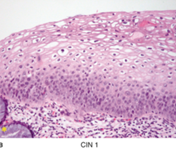
What are the characteristics of CIN (Cervical, Intraepithelial Neoplasia)? |
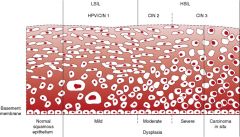
Koilocytic change, disordered cell maturation, nuclear atypia and increased mitotic activity within the cervical epithelium
Divided into grades based on extent of epithelial involvement by immature, dysplastic cells
CIN classically progresses in a stepwise fashion to CIS/invasive disease
The higher the grade of dysplasia, the more likely it is to progress, and the less likely it is to regress |
|
|
What is the origin of the uterine artery? |
Anterior division of the internal iliac |
|
|
What are the risk factors for cervical carcinoma? |
HPV infection → so anything that increases the risk for HPV infection (i.e. early age of sexual debut, multiple sexual partners, etc.)
Tobacco use |
|
|
What are the two techniques for HPV screening?When should screening be performed? |
PAP → cytological evaluation, not sensitive or specific but it works because it is done so frequently (disease transforms slowly enough that you catch it)
HPV testing → if HPV is present, a type can be identified
Screening begins at 21, initially performed yearly, >30 can be performed less frequently |
|
|
What types of HPV are covered by the qudrivalent and bivalent vaccines? When are these vaccines ideally administered? |
Quad: 6, 11, 16, 18
Bivalent: 16, 18
Ideally administer before sexual debut |
|
|
What hormone drives proliferation of the endometrium? What hormone prepares the endometrium for implantation?
What is a consequence of unopposed proliferation? |
Proliferation is estrogen driven
Preparation for implantation is progesterone driven
Endometrial hyperplasia/malignancy develops as a consequence of unopposed proliferation (estrogen) |
|
|
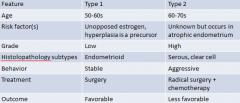
What are the features of type 1 and type 2 endometrial cancer? |
|
|
|
What are the risk factors for type 1 endometrial cancer? |
Increasing age Unopposed estrogen therapy (must add progesterone if giving HRT to a patient with a uterus) Tamoxifen therapy (commonly prescribed for the treatment and prevention of breast cancer, estrogen antagonist in the breast but estrogen agonist in the endometrium) Early menarche Late menopause (after age 55) Nulliparity PCOS (chronic anovulaiton) Obesity DM Estrogen secreting tumor Lynch syndrome Cowden syndrome Family history of endometrial/ovarian/breast/colon cancer |
|
|
What is Lynch syndrome? |
Hereditary nonpolyposis colorectal cancer
An inherited cancer due to a defect in mismatch repair genes and proteins
Mismatch is recognized by the defective machinery can't repair the mismatch → incorporated into new strand → malignancy
Increased risk of type 1 endometrial cancer |
|
|
What is endometrial hyperplasia? How does it normally present? |
Proliferation of endometrial glands relative to stroma
Classically presents as postmenopausal bleeding
Classified histologically based on architectural growth pattern (simple/complex) and presence/absence of cellular atypia
Risk of progression of hyperplasia to invasive adenocarcinoma correlates with degree of hyperplasia ("penny, nickel, dime, quarter") |
|
|
What is endometrial cancer? How does it present? What dictates therapy? |
Malignant proliferation of endometrial glands
Presents as postmenopausal/abnormal uterine bleeding
Diagnosed by endometrial biopsy
Stage determines prognosis and therapy -type 2 often requires chemotherapy after surgery
|
|
|
What are two common types of type 2 endometrial cancer? |
UPSC (uterine papillary serous carcinoma → most common type of type 2)
Clear cell carcinoma |
|
|
What is a leiomyosarcoma? What are its defining histological features? |
Malignant proliferation of smooth muscle arising from the myometrium
Do not arise from leiomyomas (fibroid, most common benign proliferation of a myometrium)
Histological features (need all three): increased mitotic activity (>10 mitoses/HPF), cellular atypia, and necrosis
Often diagnosed incidentally after hysterectomy for "fibroids"
Rare
Aggressive prognosis |
|
|
If a patient has a BRCA 1 gene mutation, which of the following malignancies is she NOT at increased risk of developing?
1) breast cancer 2) ovarian cancer 3) primary peritoneal cancer 4) pancreatic cancer 5) colon cancer |
Colon cancer |
|
|
Hemorrhage into a corpus luteum can result in ____________
Degeneration of follicles results in ___________ |
Hemorrhagic cyst
Follicular cysts |
|
|
What types of ovarian surface epithelium-stroma are benign and which are malignant? |
Benign or malignant: serous and mucinous
Malignant: endometrial, clear cell, transitional cell |
|
|
Germ cell tumors are all benign/malignant? |
malignant |
|
|
What gene mutation puts women at an increased risk for serous ovarian/tubular cancer? |
BRCA mutation |
|
|
What is a serous cystadenocarcinoma? |
Malignant tumor
Most common form of epithelial ovarian cancer/ovarian cancer in general
Complex cysts
Atypical serous cells form sheets
Most commonly arise in postmenopausal women |
|
|
What are the features of type 1 ovarian cancer? |
Clinically indolent
Present at an early stage
Exhibit shared lineage between benign neoplasms and corresponding carcinoma through an intermediate (borderline tumor) step
Include low grade serous, low grade endometrioid, clear cell, and mucinous carcinomas
Chemotherapy less effective (slow growing tumors) |
|
|
What are the features of type 2 ovarian cancer? |
Highly aggressive
Present at an advanced stage
Represent 75% of all ovarian cancers
Include high grade serous, endometrioid, and undifferentiated carcinomas
Originate from distal fallopian tube |
|
|
What is the result of a BRCA mutation (cellularly)? |
BRCA: tumor suppressor genes on chromosomes 17 (BRCA 1) and 13 (BRCA 2)
Most mutations result in truncated protein product
Proclivity for breast/ovarian cancer may be related to hormonal interactions
Function: repairs faulty DNA via homologous recombination -if mutated → tumorgenesis due to genomic instability
Mutations in BRCA1 more prevalent than mutations in BRCA2 |
|
|
What are some strategies for risk reduction of cancer development in patients with known BRCA mutations? |
Screening - least effective
Chemoprevention - OCP really lowers risk of developing ovarian cancer
Surgery - main thing that can lower risk, standard is removing both ovaries and fallopian tubes (starting to offer just removal of fallopian tubes) |
|
|
What is the most reliable predictor of epithelial ovarian cancer? |
Internal mass architecture -surgical intervention is recommended for suspicious masses (don't usually do biopsies) |
|
|
What is a reliable symptom in predicting epithelial ovarian cancer? |
Changes in bladder habits |
|
|
What are the three most common metastatic tumors to the ovary? |
Breast
Colon
Endometrium |
|
|
A patient presents with new onset abdominal bleeding. CT scan reveals a pelvic mass. Serum LDH, AFP, and hCG are all in the normal range. What is the most likely diangosis? |
Immature teratoma |
|
|
What are the three reliable markers for germ cell tumors? |
LDH
AFP
b-hCG |
|
|
What is a mature cystic teratoma ("dermoid")? Presence of what type of tissue indicates malignancy? |
Most common GCT
Cystic tumor composed of fetal tissue derived from 2 or 3 embryologic layers (skin, hair, bone, cartilage, thyroid)
Benign
Presence of immature tissue (i.e. neural) indicates malignany → immature teratoma |
|
|
What is dysgerminoma? |
Most common malignant GCT
Tumor composed of large cells with clear cytoplasm and central nuclei
Serum LDH may be elevated
|
|
|
What are the serum markers for the following germ cell and sex cord stromal tumors:
a) Dysgerminoma
b) Choriocarcinoma
c) Endodermal sinus (i.e. yolk sac tumor)
d) Immature teratoma
e) granulosa cell (sex cord-stromal tumors) |
a) LDH
b) hCG
c) AFP
d) none (don't normally have elevated tumor markers)
e) Inhibin |
|
|
An 8 year old female presents with an ovarian mass and recent history of development of breast buds and menses. What is the most likely diagnosis? |
Granulosa cell tumor |
|
|
What is a granulosa cell tumor? What is the characteristic histological finding in these tumors? |
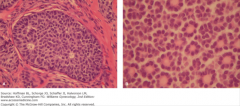
Neoplastic proliferation of granulosa and theca cells
Often produces estrogen and presents with signs of estrogen excess
Call-Exner bodies are identified by their rosette appearance
Malignant; treatment = surgery + chemo
Prognosis is more favorable than epithelial ovarian cancer |
|
|
Biopsy of a vulvar lesion showing S-100(+) cells is a sign of.... |
Vulvar melanoma (the second most common type of vulvar tumor) |
|
|
What is a condyloma? What commonly causes them? What characterizes them histologically? |
Warty neoplasm of vulvar skin, often large
Most commonly due to HPV 6 and 11
Benign process
Characterized by koilocytes (hallmark of HPV infected cells) -koilocytes = nuclear enlargement and peri-nuclear halos
Rarely progress to invasive cancer |
|
|
What is lichen sclerosis? |
Thinning of epidermis and fibrosis of the epidermis
Presents as a white patch with parchment like skin
Must be biopsied to confirm diagnosis (and make sure there's not squamous cell carcinoma in the lesion)
Most common in postmenopausal women
Autoimmune etiology
Benign; slightly increased risk for SCC
Treatment = topical steroids |
|
|
What is Paget's disease? |
Malignant epithelial cells in epidermis of vulva
Erythematous, pruritic vulvar skin
Represents CIS (carcinoma in situ) usually with no underlying carcinoma
Occasionally associated with adenocarcinoma
Treatment = wide local excision |
|
|
What is vulvar carcinoma? |
Etiology may be HPV or non-HPV related (50/50)
Arises from VIN (vulvar intraepithelial neoplasm), a dysplastic pre-cursor lesion
Generally seen in elderly women (HPV related variant can be seen in younger women, i.e. 30s)
Diagnosed by biopsy
Treatment = radical vulvectomy + groin LND |
|
|
What is a hydatidiform mole? |
Abnormal conception characterized by swollen and edematous villi with proliferation of trophoblasts
Uterus expands as if normal pregnancy is present → but uterus is much larger and beta-hCG is much higher than expected for date of gestation
Classified as partial or complete
Classic gray and white "snowstorm appearance" on ultrasound Treatment is suction curettage |
|
|
What are the features of partial and complete moles? |
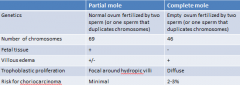
|