![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
80 Cards in this Set
- Front
- Back
|
Causes of breast lumps |
mammart dysplasia 32% fibroadenoma 23% cancer 22% cysts 10% breast abscess/periareolar inflammation 2% |
|
|
Genetic predispositions to breast cancer |
BRCA1 and BRCA2 |
|
|
Dx a new lump |
75% of lumps are not cancer but need an aspiration biopsy TRIPLE TEST |
|
|
The triple test |
1. clinical examination 2. imaging (mammogram and U/S) 3. FNA +/- core biopsy |
|
|
Most common cancer in women is ___________ affecting 1 in ____ in AUS |
breast 1 in 11 |
|
|
the incidence of breast cancer with age |
increases steadily after 30 till 60 1/3 premenopausal 2/3 postmenopausal a dominant breast lump in an older women shoeld be regarded as malignant
|
|
|
History for a breast lump |
family hx breast cancer patients past hx (trauma, previous breast pain, details about pregnancies (lactation such as mastitis, nipple problems and milk retention) |
|
|
Red flags for lumps |
- hard and irregular lump - skin dimpling and puckering - skin oedema ('peau d'orange") - nipple discharge - nipple distortion - nipple eczema |
|
|
Bloodstained nipple discharge |
— intraduct papilloma (commonest) — intraduct carcinoma — mammary dysplasia |
|
|
Green-grey nipple discharge |
— mammary dysplasia — mammary duct ectasia |
|
|
Yellow nipple discharge |
— mammary dysplasia — intraduct carcinoma (serous) — breast abscess (pus) |
|
|
MIlky white discharge |
— lactation cysts — lactation — hyperprolactinaemia — drugs (e.g. chlorpromazine) |
|
|
Pagets disease of the nipple |
- ecezema of the nipple (dry scabby red rash, then ulceration, due to underlying malignancy) - middle aged and elderly women |
|
|
DDx Pagets to eczema |
pagets is unilateral, in older patients, with possible discharge, not pruritic, no pustules, deformity of the nipple, possible palpable lump |
|
|
Ideal time to exam a breast |
ideally 4 days after the end of a period |
|
|
Method for a breast exam |
1 Inspection: sitting—patient seated upright on side of couch in good light, arms by sides, facing the doctor, undressed to waist. a Note: • asymmetry of breasts or a visible lump • localised discolouration of the skin • nipples: — for retraction or ulceration — for variations in the level (e.g. elevation on one side) — or discharge (e.g. blood-stained, clear, yellow) • skin attachment or tethering → dimpling of skin (accentuate this sign by asking patient to raise her arms above her head) • appearance of small nodules of growth • visible veins (if unilateral they suggest a cancer) • peau d’orange due to dermal oedema b Raise arms above the head (renders variations in nipple level and skin tethering more obvious). Hands are pressed on the hips to contract pectoralis major to note if there is a deep attachment of the lump. 2 Examination of lymph glands in sitting position: patient with hands on hips. Examine axillary and supraclavicular glands from behind and front. Note: The draining lymphatic nodes are in the axillae, supraclavicular fossae and internal mammary chain. 3 Palpation: a Patient still seated: palpate breast with fl at of hand and then palpate the bulk of the breast between both hands. b In supine position: • patient lies supine on couch with arms above head • turn body (slight rotation) towards midline so breasts ‘sit’ as flat as possible on chest wall Method • Use the pulps of the fingers rather than the tips with the hand laid flat on the breast. • Move the hand in slow circular movements. • Examine up and down the breast in vertical strips beginning from the axillary tail (see Fig. 92.3). • Systematically cover the six areas of the breast (see Fig. 92.4): — the four quadrants — the axillary tail — the region deep to the nipple and areola 4 If a suspicious lump is present, inspect liver, lungs and spine. 5 Inspect the bra. Note possible pressure on breast tissue from underwiring of the bra, usually on the upper outer quadrant. Note: • Forty to fifty per cent of cancers occur in the upper outer quadrant |
|
|
assessing a solitary lump |
• position (breast quadrant and proximity to nipple) • size and shape • consistency (fi rm, hard, cystic, soft) • tenderness • mobility and fi xation • attachment to skin or underlying muscle |
|
|
Positive signs on mammogram |
irregular infiltrating mass focal spotty microcalcification |
|
|
Mammorgram uses |
• established benefit for women over 50 years • possible benefit for women in their 40s • follow-up in those with breast cancer, as 6% develop in the opposite breast • localisation of the lesion for fine-needle aspiration |
|
|
Breast ulrasound |
elucidate an area of breast density and is the best method of defining benign breast disease, especially with cystic changes. It is generally most useful in women less than 35 years old |
|
|
Breast ultrasound useful for |
• pregnant and lactating breast • differentiating between fluid-filled cysts and solid mass • palpable masses at periphery of breast tissue (not screened by mammography) • for more accurate localisation of lump during fineneedle aspiration |
|
|
Very young women—12 to 25 years LUMP |
Infl amed cysts or ducts, usually close to areola Fibroadenomata, often giant Hormonal thickening, not uncommon Malignancy rare Investigations: • mammography contraindicated • ultrasound helpful |
|
|
Young women—26 to 35 years |
Classic fibroadenomata Mammary dysplasia with or without discharge Cysts uncommon Malignancy uncommon Investigations: • mammography: breasts often very dense • ultrasound often diagnostic |
|
|
Women—36 to 50 years (premenopausal) |
Cysts Mammary dysplasia, discharges, duct papillomas Malignancy common Fibroadenomata occur but cannot assume Infl ammatory processes not uncommon Investigations: • mammography useful • ultrasound useful |
|
|
Women—over 50 years (postmenopausal) |
Any new discrete mass—malignant until proven otherwise Any new thickening—regard with suspicion Infl ammatory lesions—probably duct ectasia (follow to resolution) Cysts unlikely Investigations: • mammography usually diagnostic • ultrasound may be useful |
|
|
Women over 50 years on hormones |
Any new mass—regard with suspicion Cysts may occur—usually asymptomatic Hormonal change not uncommon Investigations: • mammography usually diagnostic but breast may become more dense • ultrasound may be useful |
|
|
Oestrogen receptors in breast tissue |
unocmmon normally but found in 2/3 of breast cancers, and are a good prognostic indicator |
|
|
Method of aspiration and needle biopsy |
1 Use an aqueous skin preparation without local anaesthesia. 2 Use a 23 gauge needle and 5 mL sterile syringe. 3 Identify the mass accurately and fix it by placing three fingers of the non-dominant hand firmly on the three sides of the mass 4 Introduce the needle directly into the area of the swelling. Once in subcutaneous tissue, apply gentle suction as the needle is being advanced. If a cyst is involved it can be felt to ‘give’ suddenly. 5 If fluid is obtained (usually yellowish-green), aspirate as much as possible. 6 If no fluid is obtained, try to get a core of cells from several areas of the lump in the bore of the needle. 7 Make several passes through the lump at different angles, without exit from the skin and maintain suction. 8 Release suction before exit from the skin to keep cells in the needle (not in the syringe). 9 After withdrawal, remove syringe from needle, fill with 2 mL of air, reattach needle and produce a fine spray on one or two prepared slides. 10 Fix to one slide (in Cytofix or similar) and allow one to air dry, and forward to a reputable pathology laboratory to be examined by a skilled cytologist. |
|
|
patient with breast lump <35 IX |
ultrasound
|
|
|
patient with breast lump presents >35yr Ix? |
mammogram and US |
|
|
If lump is cystic |
aspirate
|
|
|
if lump is solid |
Fine needle biopsy |
|
|
Suscpious features |
excisional biopsy |
|
|
Indications for biospy or excision of a lump |
• The cyst fl uid is bloodstained. • The lump does not disappear completely with aspiration. • The swelling recurs within 1 month. |
|
|
Types of breast cancer |
90% invasive duct carcinoma the rest are lobular carcinoma, papillary, medullary, colloid |
|
|
Breast cancer RF |
age (>40 years), Caucasian race, pre-existing benign breast lumps, alcohol, HRT >5 years, personal history of breast cancer, family history in a fi rst-degree relative (raises risk about threefold), nulliparity, late menopause (after 53), obesity, childless until after 30 years of age, early menarche, ionising radiation exposure. |
|
|
Familial breast cancer - genetic inheritance pattern |
- 5% of all breast ca - most are Autosomal dominate
|
|
|
Main 3 presentations of breast Ca |
• the vast majority present with a local breast lump • ductal carcinoma in situ • some present with metastatic disease |
|
|
Of those who present with local disease, approximately ______% will develop metastatic disease. |
50 |
|
|
Mx of breast Ca |
- immediate referal to surgeon - staging: FBC, LFTs, sentiel nose, bone scan
|
|
|
Single most powerful prognostic and reccurrence feature in breast ca is __________ |
sentiel node
OTHERS: size, histolgy, grading, node, receptor status |
|
|
What is Ductal carcinoma in situ? |
DCIS is a non-invasive abnormal proliferation of milk duct epithelial cells within the ductal–lobular system and is a precursor lesion for invasive breast cancer. |
|
|
Mx of DCIS |
Management decisions are challenging, with options being total mastectomy or breast-conserving therapy with or without radiotherapy |
|
|
DCIS Outcomes |
excellent outcome with low local recurrence rates and a survival of at least 98%. |
|
|
Local therapy |
Tumour excision followed by whole breast irradiation was the most preferred local therapy for most women with stage I or II cancer. |
|
|
Total vs breast conserving therapy - survival - and preference |
- Total mastectomy and breast-conservation surgery had an equivalent effect on survival. - Total mastectomy is preferred for a large tumour, multifocal disease, previous irradiation and extensive tumour on mammography. |
|
|
Recommendations for radiotherapy post-mastectomy |
— tumours >4 cm in diameter — axillary node involvement of >3 nodes — the presence of positive or close tumour margins |
|
|
Chemotherapy |
• Cytotoxic chemotherapy has an important place in management. Newer regimens containing anthracyclines (e.g. epirubicin) and a taxane (e.g. docetaxel) have largely replaced the traditional CMF (cyclophosphamide, methotrexate and fl uorouracil) regimen. • Adjuvant hormonal therapy by the anti-oestrogen agent tamoxifen 20 mg (o) daily, which is a specific modulating agent, is widely used and is most suitable in postmenopausal women. |
|
|
Adjunct agents available for treatment include |
• anti-oestrogens: tamoxifen, toremifene • aromatase inhibitors: anastrozole, letrozole, exemestane • monoclonal antibodies: trastuzumab (Herceptin) • progesterones (e.g. medroxyprogesterone acetate) |
|
|
Mammary dysplasia clinical features |
• Most common in women between 30 and 50 years • Hormone-related (between menarche and menopause) • Pain and tenderness and swelling • Premenstrual discomfort or pain and increased swelling • Fluctuation in the size of the mass • Usually settles after the period • Unilateral or bilateral • Nodularity ± a discrete mass • Ache may extend down inner aspect of upper arm • Nipple discharge may occur (various colours, mainly green–grey) • Most cysts are premenopausal (fi nal 5 years before menopause) |
|
|
Examination of a mammry dysplastic breast |
Look for lumpiness in one or both breasts, usually upper outer quadrant. |
|
|
Managment of mammary dysplasia |
• Consider mammography if diffuse lumpiness is present in patient >40 years. • Perform needle biopsy if a discrete lump is present and aspirate palpable cysts. • Reassure patient that there is no cancer. • Give medication to alleviate mastalgia. • Use analgesics as necessary. • Surgically remove undiagnosed mass lesions. |
|
|
Breast cyst age |
• Common in women aged 40–50 years (perimenopausal) • Rare under 30 years |
|
|
Breast cyst cancer risk |
1 in 1000 |
|
|
Breast cyst examination |
Look for a discrete mass, firm, relatively mobile, that is rarely fluctuant. |
|
|
Dx of breast cyst |
• Mammography • Ultrasound (investigation of choice) • Cytology of aspirate |
|
|
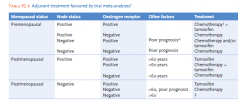
Adjuvant tx in breast cancer |
|
|
|
Lactation cysts (galactoceles) What are they? their size? how are they treated? |
• These milk-containing cysts arise during pregnancy and present postpartum with similar signs to perimenopausal cysts. • They vary from 1–5 cm in diameter. • Treat by aspiration: fl uid may be clear or milky. |
|
|
Fibroadenoma - clinically |
• A discrete, asymptomatic lump • Usually in 20s (range: second to sixth decade, commonly 15–35 years) • Firm, smooth and mobile (the ‘breast mouse’) • Usually rounded • Usually in upper outer quadrant • They double in size about every 12 months7 |
|
|
Fibroadenoma Mx |
Ultrasound and fine-needle aspiration or core biopsy with cytology is recommended plus mammography in older women. If needle aspiration or core biopsy is negative the patient can be reassured. The lump may be left in those in the late teens but as a rule it is removed to be certain of the diagnosis in all patients. |
|
|
Phyllodes tumour |
These are giant fi broadenoma-like tumours that are usually benign but 25% are malignant and metastasise. They are completely excised with a rim of normal breast tissue. |
|
|
Fat necrosis |
Fat necrosis is usually the end result of a large bruise or trauma that may be subtle, such as protracted breastfeeding. The mass that results is often accompanied by skin or nipple retraction and thus closely resembles cancer. If untreated it usually disappears but the diagnosis can only be made on excision biopsy. |
|
|
Duct papillomas |
These are benign hyperplastic lesions within large mammary ducts and are not premalignant (nor usually palpable). They present with nipple bleeding or a bloodstained discharge and must be differentiated from infiltrating carcinoma. Mammography and ductography are usually of limited value. The involved duct and affected breast segment should be excised. |
|
|
Mammary duct ectasia |
In this benign condition a whole breast quadrant may be indurated and tender. The larger breast ducts are dilated. The lump is usually located near the margin of the areola and is a fi rm or hard, tender, poorly defined swelling. There may be a toothpastelike nipple discharge. It is a troublesome condition with a tendency to repeated episodes of periareolar inflammation with recurrent abscesses and fistula formation. Many cases settle but often surgical intervention is necessary to make the diagnosis. The condition is most common in the decade around the menopause. |
|
|
Problems with breast prostheses |
- can still develop cancer and need palpation, fortunately most of the tissue is superfical and can be palpated but with difficulty at the axillary tail - mammgrams are of limited use - ultrasounds are helpful |
|
|
Lymphoedema of arm |
- complications of surgery (skin is tight and heavy) - exclude DVT with doppler US - skin changes can occur (cellulitis, abrasions..) |
|
|
Managment of lymphoedema |
• Encourage movement; elevation of the arm on a pillow at night; avoid slings • Physiotherapy: a reduction phase with non-elasticised bandages then maintenance with graduated pressure support sleeves • Elastic sleeves worn all day but not at night • Lymphoedema massage at home • Skin hygiene: regular use of non-perfumed emollients, prevention of infection and injury. Avoid sunburn and insect bites • Avoid BP measurement, venesection and IV therapy in that arm • Consider diuretics to relieve pressure |
|
|
Breast lumps in children Neonatal enlargement |
Newborn babies of either sex can present with breast hyperplasia and secretion of breast milk This is due to transplacental passage of lactogenic hormones. The swelling usually lasts 7–10 days if left alone. Any attempts to manipulate the breasts to facilitate emptying will prolong the problem. |
|
|
Premature hyperplasia in children |
The usual presentation is the development of one breast in girls commonly 7–9 years of age but sometimes younger. The feature is a fi rm discoid lump 1–2 cm in diameter, situated deep to the nipple. The same change may follow in the other breast within 3–12 months. Reassurance and explanation is the management and biopsy must be avoided at all costs. |
|
|
Premature mamillary hyperplasia in a child do you biopsy? |
AVOID at all costs |
|
|
Screening mamograms |
50-70yrs (less dense tissue) every 2 years 90% specificty and those aged 40–49 who request it. |
|
|
Breast self examinations? Controversial |
Breast self-examination is a controversial issue and has no proven benefi t in reducing morbidity and mortality. The false positive rate is high, especially in those under 40 years. However, regular BSE is recommended for all women 35 years and over. |
|
|
Mx women at high risk of breast cancer |
Monthly breast self-examination At least an annual consultation with GP—if aged 40 or older Aspiration of cysts Mammography, ultrasound and/or fi ne-needle biopsy to diagnose any localised mass Ultrasound alone for further assessment of young, dense breasts Regular screening mammography after 50 years of age—every 2 years |
|
|
Lumos that require investigation and referral |
A stony, hard lump or area, regardless of size, history or position A new palpable ‘anything’ in a postmenopausal woman A persisting painless asymmetrical thickening An enlarging mass—cyclic or not A ‘slow-to-resolve’ or recurrent infl ammation A bloodstained or serous nipple discharge Skin dimpling, of even a minor degree, or retraction of the nipple A new thickening or mass in the vicinity of a scar |
|
|
Most common cause of a lump in a women over 50 |
cancer |
|
|
Ezcema of the nipple |
Any eczematous rash appearing on the nipple or areola indicates underlying breast cancer |
|
|
Disease that cant be distinguished clinically from breast Ca |
Mammary duct ectasia and fat necrosis can be clinically indistinguishable from breast cancer |
|
|
__ out of 10 women with breast Ca dont have a stong family hx |
9 |
|
|
OCP with breast cancer risk |
show not to alter the risk of breast Ca |
|
|
Things to never do |
• Never assume that a lump is due to trauma unless you have seen the bruising and can observe the lump decrease in size. • Never assume a lesion is a cyst—prove it with ultrasound or successful aspiration. • Never ignore skin dimpling even if no underlying mass is palpable. • Never ignore a woman’s insistence that an area of her breast is different or has changed |