Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
55 Cards in this Set
- Front
- Back
|
Obj.
Describe the incorporation of yolk sac endoderm into the primitive gut as a result of cephalocaudal and lateral folding of the trilaminar germ disc. |
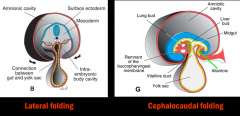
cephalocaudal (longitudinal) and lateral (transverse) folding moves the yolk sac from caudal to more cephalad and central in the embryo, eventually segmenting into the primitive gut
|
|
|
As a result of lateral and cephalocaudal folding the _________ & ______________ remain outside the embryo
|
distal portion of yolk sac & allantois
|
|
|
The primitive gut is divided into:
________ that begins at the buccupharyngeal membrane, ________ connected to the yolk sac by the vitelline duct, and ________ that ends at the cloacal membrane. |
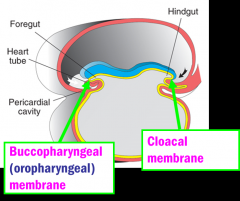
foregut
midgut hindgut |
|
|
Describe the location of the regions of the primitive gut:
Pharyngeal gut Foregut Midgut Hindgut |
Pharyngeal gut- from buccopharyngeal membrane to respiratory diverticulum
Foregut- from respiratory diverticulum to liver bud Midgut- distal to liver bud to left colic (splenic) flexure Hindgut- from left colic flexure to cloacal membrane |
|
|
Obj.
Discuss the blood supply and adult derivatives of the foregut, midgut, and hindgut. |
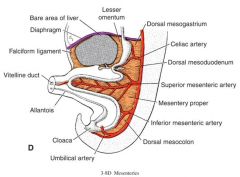
Foregut- celiac trunk
Midgut- superior mesenteric artery Hindgut- inferior mesenteric artery |
|
|
Obj.
Describe the contributions of endoderm and splanchnic mesoderm in development of the digestive tract. |
Endoderm- forms the epithelial lining of the gut & gives rise to the parenchyma of glands
Splanchnic mesoderm- forms smooth muscle, connective tissue, & visceral peritoneum of gut wall |
|
|
Portions of the gut tube are suspended by the ______________
|
mesentaries
|
|
|
Organs that are suspended from the posterior body wall by mesentary & invaginate the peritoneal sac are (intraperitoneal/retroperitoneal)?
|
intraperiotoneal
|
|
|
Organs that lie against the posterior body wall & are only partially covered by the parietal peritoneum are (intraperitoneal/retroperitoneal)?
|
retroperitoneal
*usually covered on their anterior surface be peritoneum |
|
|
Organs that are temporarily intraperitoneal but later become retroperitoneal are referred to as what?
|
secondarily retroperitoneal
|
|
|
What are peritoneal ligaments?
|
double layers of peritoneum that pass from one organ to another or from an organ to the body wall
(may carry vessels & nerves) |
|
|
what are the subdivisions of the dorsal mesentery at the 5th week of development?
|
-dorsal mesogastrium/greater omentum (stomach region)
-dorsal mesoduodenum -mesentary proper (region of jejunum & ileum) -dorsal mesocolon (colon region) |
|
|
The _________ becomes a peritoneal fold that attaches the greater curvature of the stomach & hangs over the transverse colon & loops of jejunum & ileum
|
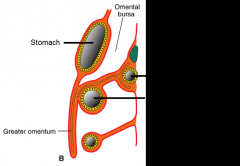
greater omentum
|
|
|
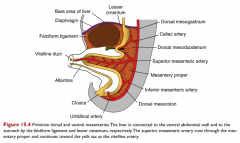
The ______________ is present only in the region of the abdominal esophagus, stomach, & upper duodenum
|
ventral mesentary
|
|
|
As the liver grows into the septum transversum it divides the ventral mesentery into what 2 things?
|
falciform ligament & lesser omentum
|
|
|
The falciform ligament contains the ____________ w/i its free lower margin, which will form the ligamentum teres hepatis after birth
|
umbilical vein
|
|
|
The lesser omentum connects the lesser curvature of the stomach via _____________________________
and the first part of the duodeunum via ______________________ |
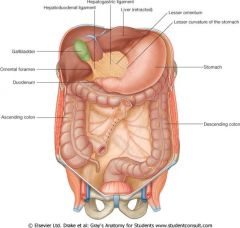
hepatogastric ligament
hepatoduodenal ligament ^ contains portal triad |
|
|
The hepatoduodenal ligament (right free margin of lesser omentum) also forms the anterior border of the ________________, which connects the omental bursa to the greater peritoneal sac.
|
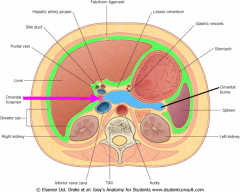
omental (epiploic) foramen
|
|
|
The esophagus has skeletal muscles from pharyngeal arches innervated by __________________ and smooth muscle innervated by ______________________.
|
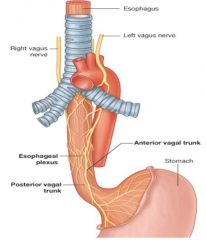
vagus nerves
parasympathetic fibers of the esophageal plexus (also from vagus nerves) |
|
|
Obj.
Discuss esophageal (and/or tracheoesophageal fistula) |
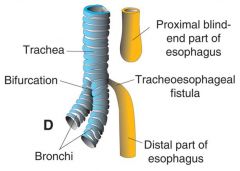
Esophagus ends in blind pouch and/or is connected to the trachea (fistula)
-due to the deviation of the tracheoesophageal septum -may result in polyhyrdamnios |
|
|
Obj.
Discuss esophageal stenosis |
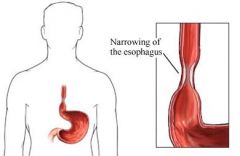
narrowing of the esophagus
-due to incomplete recanalization following an epithelial proliferation phase |
|
|
Obj.
Describe a congenital hiatal hernia |
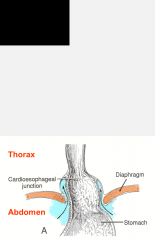
part of the stomach is pulled up through the esophagueal hiatus of the diaphram
-due to congenitally short esophagus |
|
|
Obj.
Describe rotation of the stomach and its consequences. |
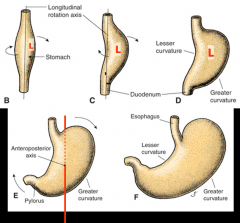
-Initially stomach develops as a fusiform swelling of gut
-first rotates 90 degrees around longitudinal axis --> original L side becomes anterior -then rotates 90 degrees around anterioposterior axis----> lesser curvature faces up/R & greater faces down/L |
|
|
Due to rotation of the stomach during development, the left vagus nerve forms most of _________________
& the right vagus nerve forms most of ______________ |
anteriorvagal trunk (left)
posteriorvagal trunk (right) |
|
|
What part of the stomach is connected to the esophagus via the gastroesophageal junction?
What part is continuous w/ the duodenum? |
cardial portion (most proximal)
pyloric part (most distal) |
|
|
As the stomach rotates, the dorsal mesogastrium is pulled (right/left) creating the ________________, behind the stomach & lesser omentum.
|
left
omental bursal |
|
|
Obj.
Describe development of the spleen |
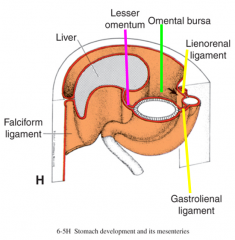
-develops from mesoderm of dorsal mesogastrium
-is divided into gastrosplenic (gastrolienal) & splenorenal (lienorenal)ligaments -the spleen is intraperiotneal |
|
|
The ___________ enters the splenorenal ligament, where it is in danger during splenectomy
|
tail of pancreas
|
|
|
The duodenum forms a C-shape around the head of the pancreas. The proximal part, to the origin of the liver bud, develops from the _____________ & the distal part from the ______________
|
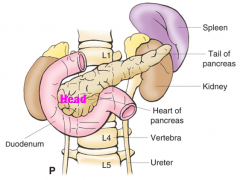
foregut
midgut |
|
|
The dorsal mesoduodenum disappears from all of the duodenum except for what part?
|
duodenal cap (ampulla)
**therefor most of duodenum = secondarily retroperitoneal |
|
|
Obj.
Discuss congenital pyloric stenosis and duodenal atresia and how their presentations may differ. |
congenital pyloric stenosis:
*non-bile stained projectile vomiting -results from hypertrophy of smooth muscle pyloric sphincer -results in obstructed passage of food from stomach to duodenum duodenal atresia (stenosis): *bile stained projectile vomiting -results from incomplete recanalization of duodenum, occurs shortly after birth -results in "double bubble sign" (shown in ultrasound scan) *polyhydraminos present in both* |
|
|
Obj.
Describe the development of the liver |
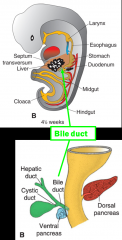
-begins as hepatic diverticulum/liver bud on the duodenum
-grows into the septum transversum -remains connected to the duodenum via bile duct once fully developed |
|
|
Obj.
Describe the development of the gallbladder. |
The gallblader & cystic duct develop from a small ventral outgrowth on the hepatic diverticulum/liver bud
|
|
|
Obj.
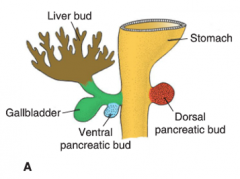
Describe the development of the pancreas. |

-initally an endodermal proliferation off the liver bud, the ventral pancreatic bud & dorsal pancreatic bud in dorsal mesoduodenum
-as duodenum rotates the ventral bud moves dorsally & fuses w/ dorsal bud -ventral bud forms the unicate process & inferior part of the head -dorsal bud forms remainder of pancreas |
|
|
Which portion of the pancreas do the main & accessory ducts form from?
Where do they open? |
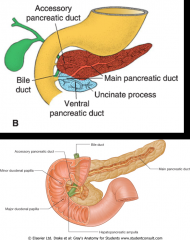
main pancreatic duct (of Wirsung):
-develops from distal dorsal pancreatic duct & entire ventral pancreatic duct -opens at major duodenal papilla accessory pancreatic duct (of Santorini): -develops from proximal part of dorsal pancreatic duct -opens at the minor duodenal papilla |
|
|
The hepatic diverticulum forms epithelial cords that differentiate into glandular__________________, enclosing ___________ formed mainly by the vitelline veins.
|

glandular parenchyma (hepatic cells)
enclosing hepatic sinusoids |
|
|
The connective tissue framework of the liver (stroma) develops from what?
|
mesoderm of the septum transversum
|
|
|
What important function does the liver have from 6wks-6mnths of fetal development?
What specific cell of the fetal liver perform this function? |
hematopoietic function (blood production)
performed by hematopoietic stem cells located in the aorta-gonad-mesonephros region |
|
|
At 12wks, the liver also begins to perform what function?
|
bile secretion
*excess bile is stored & concentrated in pancreas |
|
|
obj
Discuss the following: extrahepatic biliary atresia |

-hepatic or bile duct fails to recanalize following phase of epithelial proliferation
|
|
|
obj
Discuss the following: annular pancreas |
2 components of the ventral pancreatic duct migrate in opposite directions & encircle the duodenum
-may obstruct duodenum |
|
|
The midgut communicates w/ the yolk sac via the _______________
It is supplied by the __________________ artery |
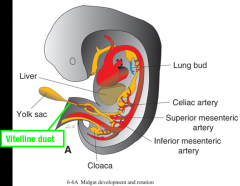
vitelline duct
Superior mesenteric artery |
|
|
Obj.
Describe the rotation of the midgut and the portions of the digestive system that become secondarily retroperitoneal as a result. |
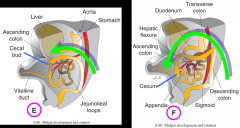
-The midgut rapidly elongates during development forming the primary intestinal loop
-primary intestinal loop has 2 limbs, cephalic & caudal -cephalic limb forms distal duodenum, jejunum, & part of ileum -caudal limb forms lower ileum, cecum, appendix, & ascending colon, & proximal 2/3 of transverse colon -as the primary loop grows it rotates 270 degrees clockwise around the superior mesenteric artery & enters the umbilical cord bc the abdomen is too small -during 10th week it returns to enlarged abdomin -in final location, the caudal limb intestines are secondarily retroperitoneal & cephalic are intraperitoneal |
|
|
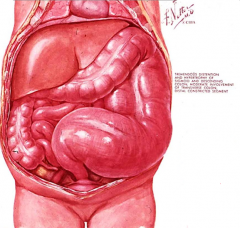
Obj.
Describe physiological herniation of the midgut |
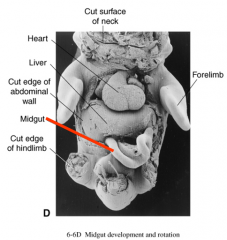
Physiological umbilical herniation occurs due to rapid growth of the liver & intestines. The abdominal cavity is too small to fit both the liver & intestines, so the intestinal loop enters the umbilical cord
*normally returns to abdomen once it enlarges |
|
|
The appendix develops from the ________ as a result of colon descent from right upper quadrant to right lower quadrant
|
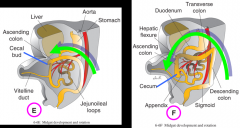
cecal bud
|
|
|
When the ascending & decending colons reach their final position, their mesentaries fuse w/ the peritoneum of the posterior abdominal wall, making them ___________________
|
secondarily retroperitoneal
|
|
|
The mesentaries of the jejunum & ileum obtain new attachments (root of mesentery) from the _________________ to the ____________)
|
duodenojejunal to the ileocecal junction
|
|
|
The transverse colon (suspended by transverse mesocolon) and sigmoid colon (by sigmoid mesocolon) both remain ___________
|
intraperitoneal
|
|
|
obj
Discuss the following anomalies: sigmoid volvulus. |
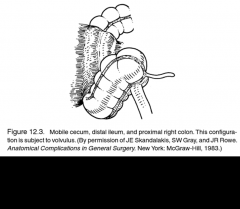
cecal (sigmoid) volvulus- mesentery of the lower ascending colon fails to fuse w/ posterior body wall & the cecum becomes twisted on it
|
|
|
The hingut forms the distal 1/3 of the transverse colon, the descending colon, sigmoid colon, rectum, upper anal canal, & ends in the ______________
What is the hindgut supplied by? |
cloaca
inferior mesenteric artery |
|
|
The _____________ is a common chamber of the urinary & digestive system
|
cloaca
|
|
|
Obj.
Describe the division of the cloaca by the urorectal septum and the clinical significance of the pectinate line. |

-The urorectal septum divides the cloaca into an anterior urogenital sinus & posterior anorectal canal
-The pectinate line divides the anal canal into a cranial & caudal portion -The cranial portion of the canal develops from endoderm & the caudal from ectoderm -The cranial & caudal portions have SEPARATE innervation, blood supply, & lymph drainage = infections, cancer, etc does not spread btwn 2 |
|
|
Differentiate btwn imperforate anus & urorectal or rectovaginal fistuala
|

imperforate anus:
-failure of recanalization of lower anal canal following epithelial proliferation =no anal canal present urorectal or rectovaginal fistuala:: -opening of hingut shifts anteriorly bc urorectal septum does not extend far enough caudally =no opening to anal canal |
|
|
Obj.
Discuss what digestive tract disorders are likely to be associated with polyhydramnios and why. |
-congential pyloric stenosis
-duodenal atresia -esophageal atresia |
|
|
obj
Discuss the following anomalies: congenital megacolon (Hirschsprung's disease) |
-autonomic (parasympathetic) ganglia are absent from a segment of the intestine
-dilated "mega" section forms proximal to the segment lacking ganglia |