Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
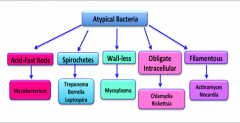
List all the atypical bacteria:
|
|
|
|
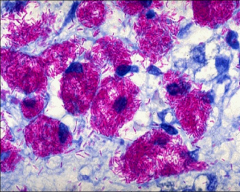
Key points about Mycobacteria:
|

*Slim “atypical” rods
*Nonmotile and nonspore forming *Obligate aerobes; many species are slow-growers *Cell wall is complex and contains long-chain fatty acids called mycolic acids and lipoarabinomannan (LAM), a lipid polysaccharide complex extending from the plasma membrane to the surface. *Acid-fastness = hallmark of Mycobacteria. |
|

|

MYCOBACTERIA
|
|
|
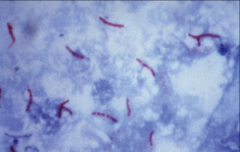
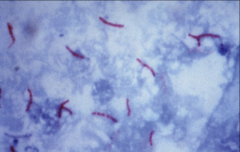
Describe the acid-fastness of Mycobacteria:
Describe the Cord factor: |

*Cannot take up stains; can be stained with Carbol Fuchsin, followed by decolorization with 3% HCL in 70% alcohol. Other organisms would be decolorized but not Mycobacteria. ACID-FAST!
*Cord factor (trehalose dimycolate) is correlated with virulence of the organism! Inhibits IFN-g (less macrophage activation) |
|
|
Describe the CW of mycobacteria:
|

*Complex, glycolipid cell wall
*Mycolic acids linked to arabinogalactan *Lipoarabinomannan (LAM): induces cytokine production *Together, these and additional cell surface proteins are antigenic. Extracted and partially purified preparations of these protein derivatives (PPDs) are used as skin test reagents to measure exposure to M. tuberculosis. |
|
|

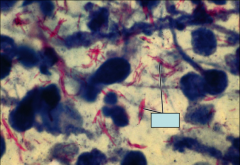
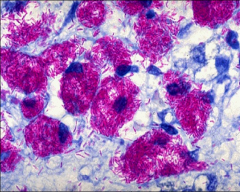
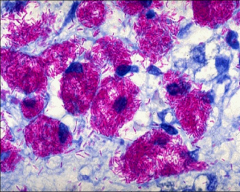
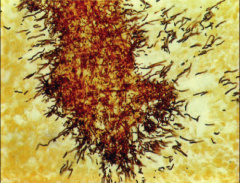
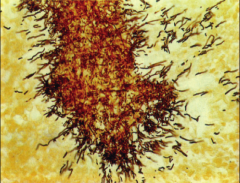
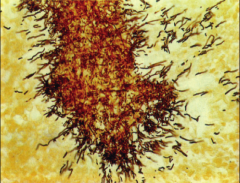
*Corded growth in mycobacteria.
|
|
|
mycobacteria
|
|
|
List clinically relevant mycobacterium species:
|
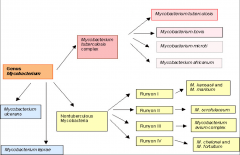
*only Runyon IV are fast-growers
*Runyon I are pigmented yellow *Main focus is on TB *Avium is associated with HIV |
|
|
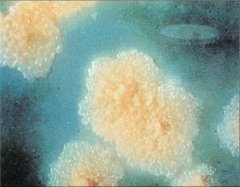
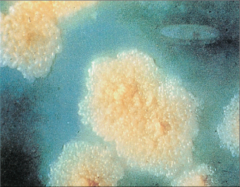
*M. tuberculosis colonies on Lowenstein-Jensen agar after 8 weeks of incubation.
*Agar contains homogenized egg in nutrient base with dyes to inhibit the growth of nonmycobacterial contaminants. |
|
|
Pathogenesis of M. TB:
|
*Mycobacteria include a wide range of species pathogenic for humans and animals.
*M. tuberculosis is a STRICT HUMAN pathogen. *Most nonpathogenic species are widely distributed in the environment. Diseases caused by mycobacteria usually develop slowly, follow a chronic course, and elicit a GRANULOMATOUS response. *Mycobacteria lack classic exotoxins and endotoxins!!!! Disease is related to host immune response (DTH and cell-mediated immunity). |
|
|
HOW IS TB SPREAD???
|
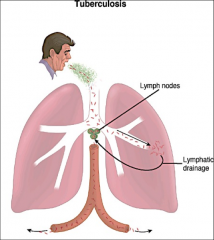
*Spread via aerosol droplet nuclei from patients with active pulmonary TB.
*Brief encounters pose limited risk; usually repeated or prolonged contact is required for transmission. *Initial multiplication is in the alveoli with spread through lymphatic drainage to the hilar lymph nodes. *Lymphatic drainage to the bloodstream can spread organisms throughout the body. |
|
|
What happens with TB once it reaches the alveoli?
|

*Once in alveoli, the organism gets ingested by macrophages.
*Instead of being killed, M. tuberculosis survives as an intracellular pathogen by blocking acidification of phagosome and phagolysosome formation. *Ingested bacteria multiply in the macrophage. |
|
|
What does our immune system do once TB gets into the alveoli?
|

*Th1 cellular immune responses attempt to activate the macrophage by secreting cytokines. If successful, the disease is arrested.
*Inflammatory elements of DTH are attracted and cause destruction. *If activation is not successful, disease and injury continue. If the Th1 process is effective, the source of DTH stimulation wanes and the disease resolves. *Success depends on size of the inoculum. If dose is too large, you get remaining dormant infections. |
|
|
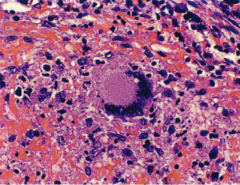
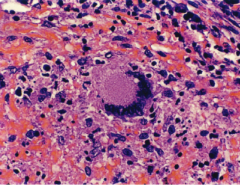
The response to TB manifests in the formation of a granuloma.
|
|
|
DTH in response to TB leads to caseous necrosis in the center of the lesion. Visible in x-rays.
|
|
|
Describe dormant TB reactivation:
|
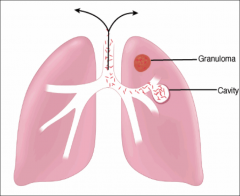
*Dormant TB reactivation typically starts in the upper lobes of the lung (more oxygen up there) with granuloma formation.
*DTH-mediated destruction can form a cavity, which allows the organisms to be coughed up to infect another person. *Have to immune compromised for this to happen (aging for example). |
|
|
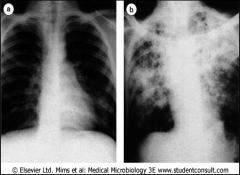
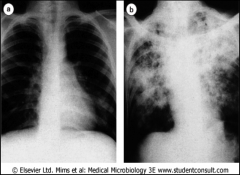
Chest radiographs of (a) primary tuberculosis, showing the Ghon focus in the lower left lung, and (b) post-primary pulmonary tuberculosis showing advanced disease.
|
|
|
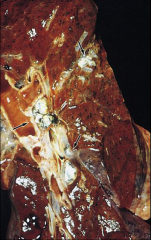
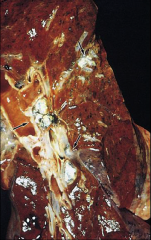
*miliary TB--it has seeded entire lung. Can occur with severe immune compromise like HIV.
|
|
|
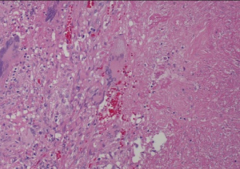
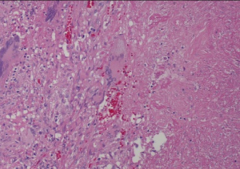
Overview picture of TB pathology:
|
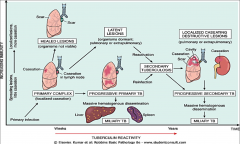
*several scenarios for reactivation
|
|
|
Key points about M. avium-intracellulare complex (MAC):
|
*Frequently recovered from soil and water
*Some cause TB in birds but do not infect humans; whereas others infect a variety of mammals including humans. *Both species produce disease in immunocompromised individuals. *M. avium is the most common opportunistic bacterial infection seen in late AIDS patients. |
|
|
M. avium-intracellulare complex (MAC)
|
|
|
Key points about Mycobacterium leprae:
|
*Cannot be cultured; grows only in armadillos
*Obligate intracellular parasite of macrophages and Schwann cells *Prolonged exposure with a household contact, i.e. from exudates of skin lesions from a leprosy patient, is required to become infected. *The incubation period for leprosy is 5-7 years; clinical disease may develop several years after initial contact with organism. *Rare in U.S.; wider problem worldwide where about 10-12 million are infected (India, China, Brazil, Nigeria); in U.S. most often seen in immigrants from endemic areas. |
|
|
Damage and Disease from m. leprae:
|
*Leprosy (Hansen’s Disease) is a chronic granulomatous condition of the peripheral nerves and mucocutaneous tissues, particularly the nasal mucosa.
*The disease occurs in two major forms with a spectrum of illness in between: -Tuberculoid form: few M. leprae are seen in lesions, which are granulomatous with extensive epithelioid cells, giant cells, and lymphocytic infiltration; skin and nerve involvement. -Lepromatous form: the cellular response is minimal, and growth of M leprae is thus relatively unimpeded. Lesions are infiltrative and diffuse. *Success of immune response determines which form. |
|

|

Mycobacterium leprae. Acid-fast stains of skin biopsies from patients with (A) tuberculoid leprosy, (B) borderline tuberculoid leprosy, (C) borderline lepromatous leprosy, and (D) lepromatous leprosy. Note that there is a progressive increase in bacteria going from the tuberculoid form to the lepromatous form of the disease.
|
|

|

Mycobacterium leprae. Leprosy lesions.
|
|
|
Key points about Actinomyces:
|
*Slow-growing anaerobic branching Gram-positive rods.
*Part of normal flora of oral cavity. *Most infections due to Actinomyces israelii. *After local trauma such as a broken jaw or dental extraction, it may invade tissues forming filaments surrounded by areas of inflammation. *In pus and tissues, the most characteristic form is the sulfur granule. *Lesions typically involve face and neck. |
|
|
actinomyces - sulfur granules
|
|
|
Key points about Mycoplasma:
|

*Lack a cell wall.
*They are bounded by a single triple-layered membrane that contains sterols. *They are highly plastic and pleomorphic and may appear as coccoid bodies, filaments, and large multinucleoid forms. *Numerous Mycoplasma species have been isolated from animals and humans, but only two species have been significantly associated with human disease: -Mycoplasma pneumonia: a lower respiratory tract pathogen. -Mycoplasma genitalium: causes genitourinary tract infections. |
|

|

mycoplasma
|