Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
8 Cards in this Set
- Front
- Back

1-Bladder Extrophy def?
2-Pathology bladder extrophy? |
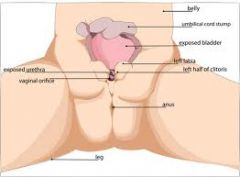
1-A cong diz musculoskeletal & genitourinary sys. 2- abn ant rupture cloacal membrane early in embryonic period; mesenchymal ingrowth into abd wall is also inhibited; altered migration of sclerotomes that comprise ant elements (pubis)
|
|

PE-bladder extrophy? (acetbuli & gait)
tx of BE? |
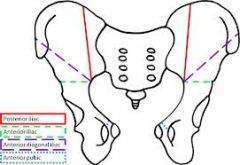
1-acetabuli 12 deg ER w/out pubis to tether ant ring, pos elements ER;-gait external ft progression; 2 stg I: 1^ closure bladdr; stg II: epispadias repair M; stg III: bladder neck recon; pelvic osteotomies perfrmd @ any stage
|
|
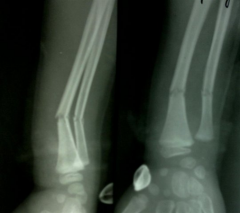
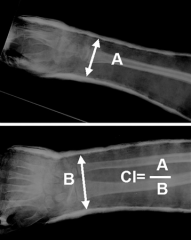
8yo B fell ridg bike & landad on outstretched arm. xrays Fig A. Which inc risk of displacement follwg CR & castg? 1-LAC; 2-SAC; 3-Cast index > 0.85; 4. Conscious sedation during reduction; 5. Plaster cast immobilization
|
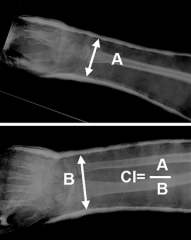
cast index = sagittal width of cast / coronal width. average cast index of patients who lost reduction >0.79 vs < 0.70 patients who did NOT lose reduction. Ans3
|
|
prepg to cast a child w/ both-bn forearm fx in ER. Durg cast app, all are directly related to the risk of thermal injury except? 1-Layers thickness castg; 2-Water temp used to dip castg ; 3-Placg limb on pillow durg the cast curg;
|

4-Fiberglass overwrappg plaster casts; 5-Type of fx pattern:excessively thick plaster, dip-h20 temp >24 deg, placg the limb on a pillow during the curing proc, & fiberglass overwrappg all inc risk ->thermal injury w/ skin burns.Ans5
|
|

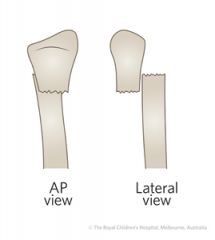
Isolated pronation forearm will most likely achieve redctn of what type of fx in a 7yo B? 1-Sup inj apex-volar greenstick both bn forearm fx; 2-Pron inj apex-dorsal greenstick both bn forearm fx;3-Sup inj apex-dorsal
|

greenstick both bn forearm fx; 4-Complete both bn forearm fx w/ bayonete apposition of both the radius & ulna; 5-Dis radius fx w/ 25 deg of apex-dorsal angul; As a rule of thumb, reduced pointing the palm ->direction defrm.Ans1
|
|

Acceptable Angul for CR Pedi Forearm Fx (controversial)
Shaft / Both bn fx & Dis rad/ulna |
Acceptable->(MAD Bayonetg) Malrotation:Angul;Dorsal Angul; Bayonetg;
<10 mad bayoneting:m-45; a-15; d-30; bay-<1 cm >10 MAD BAYONETING :M-30; A-10; D-20; BAY--<1 cm |
|

18yo G w/ deformity L leg limits ability to play b'ball. c/o pain->lat jt line w/ vigorous act. supine pos. Fig A. standg alignment Fig B w/ mech lat dis fem ang @ 73° (mLDFA 88°), mech med prox tib ang of 87° (mMPTA 87°) & tib fem ang 25°.
|
Which is the most appropriate S Tx?1-Lat closg wedge prox fem osteotomy w/ med openg wedge tib osteotmy; 2-Lat closg wedge tib osteotmy; 3-Med openg wedge fem osteotmy; 4-Med closg wedge tib osteotmy; 5-Med closg wedge fem osteotmyAns5
|
|

12yo skeletally immtur B c/o several yr hx low extrmty defrmty. medical hx (+): asthma & eczema. (-) constitut sx. neurovascularly intact b/l low extrmty. xray Fig A. most appropriate Tx? 1-(HKAFO) orthotic; 2-Dis fem ostetmy w/ plate fix b/l dis fem
|

3-Tensn band plate across b/l med dis fem grwth plts
4-Tension band plt across R med dis fem growth plt; 5-Lat hemiepiphys b/l dis fem growth plts; Surg Tx: if mech axis line drawn cntr head fem-> cntr ankle falls > outr 25% tib platu > 10yrAns3 |